Label: TOBRAMYCIN AND DEXAMETHASONE suspension/ drops

- NDC Code(s): 61314-647-05, 61314-647-10, 61314-647-25
- Packager: Sandoz Inc
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated May 28, 2021
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
DESCRIPTION
Tobramycin and dexamethasone ophthalmic suspension is a sterile, multiple dose antibiotic and steroid combination for topical ophthalmic use.
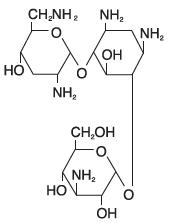
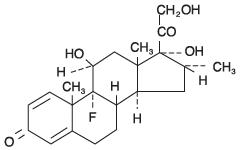
The chemical structures for tobramycin and dexamethasone are presented below:
Tobramycin Empirical Formula: C18H37N5O9
Chemical Name: O-3-Amino-3-deoxy-α- D-glucopyranosyl-(1→4)-O-[2,6-diamino-2,3,6-trideoxy-α-D-ribo-hexopyranosyl- (1→6)]-2-deoxy-L-streptamine
Molecular Weight: 467.52
Dexamethasone Empirical Formula: C22H29FO5
Chemical Name: 9-Fluoro-11β,17,21-trihydroxy-16α-methylpregna-1,4-diene-3,20-dione
Molecular Weight: 392.47
Each mL of tobramycin and dexamethasone ophthalmic suspension contains: Actives: tobramycin 0.3% (3 mg) and dexamethasone 0.1% (1 mg). Preservative: benzalkonium chloride 0.01%. Inactives: edetate disodium, hydroxyethyl cellulose, purified water, sodium chloride, sodium sulfate, sulfuric acid and/or sodium hydroxide (to adjust pH), and tyloxapol.
-
CLINICAL PHARMACOLOGY
Corticoids suppress the inflammatory response to a variety of agents and they probably delay or slow healing. Since corticoids may inhibit the body's defense mechanism against infection, a concomitant antimicrobial drug may be used when this inhibition is considered to be clinically significant. Dexamethasone is a potent corticoid.
The antibiotic component in the combination (tobramycin) is included to provide action against susceptible organisms. In vitro studies have demonstrated that tobramycin is active against susceptible strains of the following microorganisms:
Staphylococci, including S. aureus and S. epidermidis (coagulase-positive and coagulase-negative), including penicillin-resistant strains.
Streptococci, including some of the Group A-beta-hemolytic species, some nonhemolytic species, and some Streptococcus pneumoniae.
Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes, Proteus mirabilis, Morganella morganii, most Proteus vulgaris strains, Haemophilus influenzae and H. aegyptius, Moraxella lacunata, Acinetobacter calcoaceticus and some Neisseria species.
No data are available on the extent of systemic absorption from tobramycin and dexamethasone ophthalmic suspension; however, it is known that some systemic absorption can occur with ocularly applied drugs.
-
INDICATIONS AND USAGE
Tobramycin and dexamethasone ophthalmic suspension is indicated for steroid-responsive inflammatory ocular conditions for which a corticosteroid is indicated and where superficial bacterial ocular infection or a risk of bacterial ocular infection exists.
Ocular steroids are indicated in inflammatory conditions of the palpebral and bulbar conjunctiva, cornea and anterior segment of the globe where the inherent risk of steroid use in certain infective conjunctivitides is accepted to obtain a diminution in edema and inflammation. They are also indicated in chronic anterior uveitis and corneal injury from chemical, radiation or thermal burns, or penetration of foreign bodies.
The use of a combination drug with an anti-infective component is indicated where the risk of superficial ocular infection is high or where there is an expectation that potentially dangerous numbers of bacteria will be present in the eye.
The particular anti-infective drug in this product is active against the following common bacterial eye pathogens:
Staphylococci, including S. aureus and S. epidermidis (coagulase-positive and coagulase-negative), including penicillin-resistant strains.
Streptococci, including some of the Group A-beta-hemolytic species, some nonhemolytic species, and some Streptococcus pneumoniae.
Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes, Proteus mirabilis, Morganella morganii, most Proteus vulgaris strains, Haemophilus influenzae and H. aegyptius, Moraxella lacunata, Acinetobacter calcoaceticus and some Neisseria species.
- CONTRAINDICATIONS
-
WARNINGS
FOR TOPICAL OPHTHALMIC USE. NOT FOR INJECTION INTO THE EYE. Sensitivity to topically applied aminoglycosides may occur in some patients. Severity of hypersensitivity reactions may vary from local effects to generalized reactions, such as erythema, itching, urticaria, skin rash, anaphylaxis, anaphylactoid reactions, or bullous reactions. If a sensitivity reaction does occur, discontinue use.
Prolonged use of steroids may result in glaucoma, with damage to the optic nerve, defects in visual acuity and fields of vision, and posterior subcapsular cataract formation. Intraocular pressure (IOP) should be routinely monitored even though it may be difficult in pediatric patients and uncooperative patients. Prolonged use may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions and parasitic infections of the eye, steroids may mask infection or enhance existing infection.
In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids.
-
PRECAUTIONS
General
The possibility of fungal infections of the cornea should be considered after long-term steroid dosing. As with other antibiotic preparations, prolonged use may result in overgrowth of nonsusceptible organisms, including fungi. If superinfection occurs, appropriate therapy should be initiated. When multiple prescriptions are required, or whenever clinical judgement dictates, the patient should be examined with the aid of magnification, such as slit lamp biomicroscopy and, where appropriate, fluorescein staining.
Cross-sensitivity to other aminoglycoside antibiotics may occur; if hypersensitivity develops with this product, discontinue use and institute appropriate therapy.
Information for Patients
Do not touch dropper tip to any surface, as this may contaminate the contents. Contact lenses should not be worn during the use of this product.
Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies have been conducted to evaluate the carcinogenic or mutagenic potential. No impairment of fertility was noted in studies of subcutaneous tobramycin in rats at doses of 50 and 100 mg/kg/day.
Pregnancy
Corticosteroids have been found to be teratogenic in animal studies. Ocular administration of 0.1% dexamethasone resulted in 15.6% and 32.3% incidence of fetal anomalies in two groups of pregnant rabbits. Fetal growth retardation and increased mortality rates have been observed in rats with chronic dexamethasone therapy. Reproduction studies have been performed in rats and rabbits with tobramycin at doses up to 100 mg/kg/day parenterally and have revealed no evidence of impaired fertility or harm to the fetus.
There are no adequate and well-controlled studies in pregnant women. However, prolonged or repeated corticoid use during pregnancy has been associated with an increased risk of intra-uterine growth retardation. Tobramycin and dexamethasone ophthalmic suspension should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Infants born of mothers who have received substantial doses of corticosteroids during pregnancy should be observed carefully for signs of hypoadrenalism.
-
Nursing Mothers
Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk. Because many drugs are excreted in human milk, caution should be exercised when tobramycin and dexamethasone ophthalmic suspension is administered to a nursing woman.
- Pediatric Use
- Geriatric Use
-
ADVERSE REACTIONS
Adverse reactions have occurred with steroid/anti-infective combination drugs which can be attributed to the steroid component, the anti-infective component, or the combination. Exact incidence figures are not available.
The most frequent adverse reactions to topical ocular tobramycin (tobramycin ophthalmic solution 0.3%) are hypersensitivity and localized ocular toxicity, including lid itching and swelling, and conjunctival erythema. These reactions occur in less than 4% of patients. The reactions due to the steroid component are: elevation of IOP with possible development of glaucoma, and infrequent optic nerve damage; posterior subcapsular cataract formation; and delayed wound healing.
Secondary Infection: The development of secondary infection has occurred after use of combinations containing steroids and antimicrobials. Fungal infections of the cornea are particularly prone to develop coincidentally with long-term applications of steroids. The possibility of fungal invasion must be considered in any persistent corneal ulceration where steroid treatment has been used. Secondary bacterial ocular infection following suppression of host responses also occurs.
Postmarketing Experience
Additional adverse reactions identified from postmarketing use include anaphylactic reaction, erythema multiforme.
The following additional adverse reactions have been reported with the individual components listed below:
Dexamethasone: Cushing’s syndrome and adrenal suppression may occur after use of dexamethasone in excess of the listed dosing instructions in predisposed patients, including children and patients treated with CYP3A4 inhibitors.
Aminoglycosides: Neurotoxicity, ototoxicity, and nephrotoxicity have occurred in patients receiving systemic aminoglycoside therapy. Aminoglycosides may aggravate muscle weakness in patients with known or suspected neuromuscular disorders, such as myasthenia gravis or Parkinson’s disease, because of their potential effect on neuromuscular function.
-
DOSAGE AND ADMINISTRATION
One or two drops instilled into the conjunctival sac(s) every four to six hours. During the initial 24 to 48 hours, the dosage may be increased to one or two drops every two (2) hours. Frequency should be decreased gradually as warranted by improvement in clinical signs. Care should be taken not to discontinue therapy prematurely.
Not more than 20 mL should be prescribed initially and the prescription should not be refilled without further evaluation as outlined in PRECAUTIONS above.
-
HOW SUPPLIED
Sterile ophthalmic suspension in 2.5 mL (NDC61314-647-25), 5 mL (NDC61314-647-05) and 10 mL (NDC61314-647-10) dispensers.
STORAGE
Store at 8°C to 27°C (46°F to 80°F).
Store suspension upright and shake well before using.
After opening, tobramycin and dexamethasone ophthalmic suspension can be used until the expiration date on the bottle.
Distributed by Sandoz Inc.
Princeton, NJ 08540
May 2021
T2021-123
775950 US
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
TOBRAMYCIN AND DEXAMETHASONE
tobramycin and dexamethasone suspension/ dropsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:61314-647 Route of Administration OPHTHALMIC Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TOBRAMYCIN (UNII: VZ8RRZ51VK) (TOBRAMYCIN - UNII:VZ8RRZ51VK) TOBRAMYCIN 3 mg in 1 mL DEXAMETHASONE (UNII: 7S5I7G3JQL) (DEXAMETHASONE - UNII:7S5I7G3JQL) DEXAMETHASONE 1 mg in 1 mL Inactive Ingredients Ingredient Name Strength TYLOXAPOL (UNII: Y27PUL9H56) EDETATE DISODIUM (UNII: 7FLD91C86K) SODIUM CHLORIDE (UNII: 451W47IQ8X) SODIUM SULFATE (UNII: 0YPR65R21J) SULFURIC ACID (UNII: O40UQP6WCF) SODIUM HYDROXIDE (UNII: 55X04QC32I) WATER (UNII: 059QF0KO0R) BENZALKONIUM CHLORIDE (UNII: F5UM2KM3W7) HYDROXYETHYL CELLULOSE (2000 MPA.S AT 1%) (UNII: S38J6RZN16) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:61314-647-25 2.5 mL in 1 BOTTLE; Type 0: Not a Combination Product 01/02/2009 2 NDC:61314-647-05 5 mL in 1 BOTTLE; Type 0: Not a Combination Product 01/02/2015 3 NDC:61314-647-10 10 mL in 1 BOTTLE; Type 0: Not a Combination Product 01/02/2009 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA authorized generic NDA050592 01/02/2009 Labeler - Sandoz Inc (005387188)