ABRAXANE
-
paclitaxel injection, powder, lyophilized, for suspension
Abraxis BioScience, LLC
----------
ABRAXANE® for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension)(albumin-bound)
Rx Only
(Patient Information Enclosed)
WARNING
ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) should be administered under the supervision of a physician experienced in the use of cancer chemotherapeutic agents. Appropriate management of complications is possible only when adequate diagnostic and treatment facilities are readily available.
ABRAXANE therapy should not be administered to patients with metastatic breast cancer who have baseline neutrophil counts of less than 1,500 cells/mm3. In order to monitor the occurrence of bone marrow suppression, primarily neutropenia, which may be severe and result in infection, it is recommended that frequent peripheral blood cell counts be performed on all patients receiving ABRAXANE.
Note: An albumin form of paclitaxel may substantially affect a drug's functional properties relative to those of drug in solution. DO NOT SUBSTITUTE FOR OR WITH OTHER PACLITAXEL FORMULATIONS.
DESCRIPTION
ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) is an albumin-bound form of paclitaxel with a mean particle size of approximately 130 nanometers. Paclitaxel exists in the particles in a non-crystalline, amorphous state. ABRAXANE is supplied as a white to yellow, sterile, lyophilized powder for reconstitution with 20 mL of 0.9% Sodium Chloride Injection, USP prior to intravenous infusion. Each single-use vial contains 100 mg of paclitaxel and approximately 900 mg of human albumin. Each milliliter (mL) of reconstituted suspension contains 5 mg paclitaxel. ABRAXANE is free of solvents.
The active agent in ABRAXANE® is paclitaxel, a natural product with antitumor activity. Paclitaxel is obtained from Taxus media. The chemical name for paclitaxel is 5β,20-Epoxy-1,2α,4,7β,10β,13α-hexahydroxytax-11-en-9-one 4,10-diacetate 2-benzoate 13-ester with (2R,3S)-N-benzoyl-3-phenylisoserine.
Paclitaxel has the following structural formula:
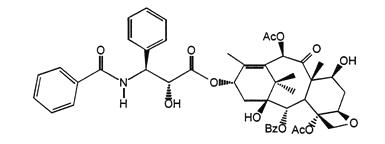
Paclitaxel is a white to off-white crystalline powder with the empirical formula C47H51NO14 and a molecular weight of 853.91. It is highly lipophilic, insoluble in water, and melts at approximately 216°C to 217°C.
CLINICAL PHARMACOLOGY
Mechanism of Action
ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) is an antimicrotubule agent that promotes the assembly of microtubules from tubulin dimers and stabilizes microtubules by preventing depolymerization. This stability results in the inhibition of the normal dynamic reorganization of the microtubule network that is essential for vital interphase and mitotic cellular functions. Paclitaxel induces abnormal arrays or "bundles" of microtubules throughout the cell cycle and multiple asters of microtubules during mitosis.
Human Pharmacokinetics
The pharmacokinetics of total paclitaxel following 30 and 180-minute infusions of ABRAXANE at dose levels of 80 to 375 mg/m2 were determined in clinical studies. Dose levels of mg/m2 refer to mg of paclitaxel in ABRAXANE. Following intravenous administration of ABRAXANE, paclitaxel plasma concentrations declined in a biphasic manner, the initial rapid decline representing distribution to the peripheral compartment and the slower second phase representing drug elimination. The terminal half-life was about 27 hours.
The drug exposure (AUCs) was dose proportional over 80 to 375 mg/m2 and the pharmacokinetics of paclitaxel for ABRAXANE® were independent of the duration of administration. At the recommended ABRAXANE clinical dose, 260 mg/m2, the mean maximum concentration of paclitaxel, which occurred at the end of the infusion, was 18,741 ng/mL. The mean total clearance was 15 L/hr/m2. The mean volume of distribution was 632 L/m2; the large volume of distribution indicates extensive extravascular distribution and/or tissue binding of paclitaxel.
The pharmacokinetic data of 260 mg/m2 ABRAXANE administered over 30 minutes was compared to the pharmacokinetics of 175 mg/m2 paclitaxel injection over 3 hours. The clearance of ABRAXANE was larger (43%) than for the clearance of paclitaxel injection and the volume of distribution of ABRAXANE was also higher (53%). Differences in Cmax and Cmax corrected for dose reflected differences in total dose and rate of infusion. There were no differences in terminal half-lives.
In vitro studies of binding to human serum proteins, using paclitaxel concentrations ranging from 0.1 to 50 µg/mL, indicate that between 89% to 98% of drug is bound; the presence of cimetidine, ranitidine, dexamethasone, or diphenhydramine did not affect protein binding of paclitaxel.
After a 30-minute infusion of 260 mg/m2 doses of ABRAXANE, the mean values for cumulative urinary recovery of unchanged drug (4%) indicated extensive non-renal clearance. Less than 1% of the total administered dose was excreted in urine as the metabolites 6α-hydroxypaclitaxel and 3'-p-hydroxypaclitaxel. Fecal excretion was approximately 20% of the total dose administered.
In vitro studies with human liver microsomes and tissue slices showed that paclitaxel was metabolized primarily to 6α-hydroxypaclitaxel by CYP2C8; and to two minor metabolites, 3'-p-hydroxypaclitaxel and 6α, 3'-p-dihydroxypaclitaxel, by CYP3A4. In vitro, the metabolism of paclitaxel to 6α-hydroxypaclitaxel was inhibited by a number of agents (ketoconazole, verapamil, diazepam, quinidine, dexamethasone, cyclosporin, teniposide, etoposide, and vincristine), but the concentrations used exceeded those found in vivo following normal therapeutic doses. Testosterone, 17α-ethinyl estradiol, retinoic acid, and quercetin, a specific inhibitor of CYP2C8, also inhibited the formation of 6α-hydroxypaclitaxel in vitro. The pharmacokinetics of paclitaxel may also be altered in vivo as a result of interactions with compounds that are substrates, inducers, or inhibitors of CYP2C8 and/or CYP3A4 (see PRECAUTIONS: Drug Interactions).
The pharmacokinetic profile of ABRAXANE administered as a 30-minute infusion was evaluated in 15 out of 30 solid tumor patients with mild to severe hepatic impairment defined by serum bilirubin levels and AST levels. Patients with AST > 10 × ULN and bilirubin > 5.0 × ULN were not enrolled. ABRAXANE doses were assigned based on the degree of hepatic impairment as described:
- Mild (bilirubin > ULN to ≤ 1.25 × ULN and AST > ULN and < 10 × ULN): 260 mg/m2
- Moderate (bilirubin 1.26 to 2.0 × ULN and AST > ULN and < 10 × ULN): 200 mg/m2
- Severe (bilirubin 2.01 to 5.0 × ULN and AST > ULN and < 10 × ULN): 130 mg/m2
The 260 mg/m2 dose for mild impairment and the 200 mg/m2 dose for moderate hepatic impairment adjusted the paclitaxel exposure to the range seen in patients with normal hepatic function (mean AUC0-∞ = 14789 ± 6703). The 130 mg/m2 dose in patients with severe hepatic impairment resulted in lower paclitaxel exposures than those seen in normal subjects. In addition, patients with severe hepatic impairment had higher mean cycle 1 absolute neutrophil count (ANC) nadir values than those with mild and moderate hepatic impairment.
| Mild (n=5) | Moderate (n=5) | Severe*
(n=5) |
|
|---|---|---|---|
| Dose | 260 mg/m2 | 200 mg/m2 | 130 mg/m2 |
| AUCinf(hr*ng/mL) | |||
|
|||
| Mean ± SD | 17434 ± 11454 | 14159 ± 13346 | 9187 ± 6475 |
| Median (range) | 13755 (7618, 35262) | 7866 (5919, 37613) | 6134 (5627, 20684) |
A starting dose of 130 mg/m2 is recommended in patients with severe hepatic impairment. Escalation of the dose up to 200 mg/m2 should be considered for subsequent cycles in patients with severe hepatic impairment based on individual tolerance. The 200 mg/m2 dose has not been evaluated in patients with severe hepatic impairment, but it is predicted to adjust the paclitaxel AUC to the range observed in patients with normal hepatic function. A starting dose reduction is also needed for patients with moderate hepatic impairment. There are no data for patients with AST > 10 × ULN and bilirubin > 5.0 × ULN. (see DOSAGE and ADMINISTRATION: Hepatic Impairment).
The effect of renal dysfunction on the disposition of ABRAXANE® has not been investigated.
Possible interactions of paclitaxel with concomitantly administered medications have not been formally investigated.
CLINICAL STUDIES
Metastatic Breast Carcinoma
Data from 106 patients accrued in two single arm open label studies and from 460 patients enrolled in a randomized comparative study were available to support the use of ABRAXANE in metastatic breast cancer.
Single Arm Open Label Studies
In one study, ABRAXANE was administered as a 30-minute infusion at a dose of 175 mg/m2 to 43 patients with metastatic breast cancer. The second trial utilized a dose of 300 mg/m2 as a 30 minute infusion in 63 patients with metastatic breast cancer. Cycles were administered at 3 week intervals. Objective responses were observed in both studies.
Randomized Comparative Study
This multicenter trial was conducted in 460 patients with metastatic breast cancer. Patients were randomized to receive ABRAXANE at a dose of 260 mg/m2 given as a 30-minute infusion, or paclitaxel injection at 175 mg/m2 given as a 3-hour infusion. Sixty-four percent of patients had impaired performance status (ECOG 1 or 2) at study entry; 79% had visceral metastases; and 76% had > 3 sites of metastases. Fourteen percent of the patients had not received prior chemotherapy; 27% had received chemotherapy in the adjuvant setting, 40% in the metastatic setting and 19% in both metastatic and adjuvant settings. Fifty-nine percent received study drug as second or greater than second-line therapy. Seventy-seven percent of the patients had been previously exposed to anthracyclines.
In this trial, patients in the ABRAXANE® treatment arm had a statistically significantly higher reconciled target lesion response rate (the trial primary endpoint) of 21.5% (95% CI: 16.2% to 26.7%), compared to 11.1% (95% CI: 6.9% to 15.1%) for patients in the paclitaxel injection treatment arm. See Table 2. There was no statistically significant difference in overall survival between the two study arms.
| ABRAXANE 260 mg/m2 | Paclitaxel Injection 175 mg/m2 |
||
|---|---|---|---|
| Reconciled Target Lesion Response Rate (primary endpoint) * | |||
|
|||
| All randomized patients | Response Rate [95% CI] | 50/233 (21.5%) [16.19% – 26.73%] | 25/227 (11.1%) [6.94% – 15.09%] |
| P-value † | 0.003 | ||
| Patients who had failed combination chemotherapy or relapsed within 6 months of adjuvant chemotherapy‡ | Response Rate [95% CI] | 20/129 (15.5%) [9.26% – 21.75%] | 12/143 (8.4%) [3.85% – 12.94%] |
INDICATION
ABRAXANE® for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) is indicated for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated.
CONTRAINDICATIONS
ABRAXANE should not be used in patients who have baseline neutrophil counts of < 1,500 cells/mm3.
WARNINGS
Bone marrow suppression (primarily neutropenia) is dose dependent and a dose limiting toxicity. ABRAXANE should not be administered to patients with baseline neutrophil counts of < 1,500 cells/mm3. Frequent monitoring of blood counts should be instituted during ABRAXANE treatment. Patients should not be retreated with subsequent cycles of ABRAXANE until neutrophils recover to a level >1,500 cells/mm3 and platelets recover to a level >100,000 cells/mm3.
The use of ABRAXANE has not been studied in patients with renal dysfunction. In the randomized controlled trial, patients were excluded for baseline serum bilirubin >1.5 mg/dL or baseline serum creatinine >2 mg/dL.
Pregnancy
Teratogenic Effects
Pregnancy Category D
ABRAXANE can cause fetal harm when administered to a pregnant woman. Administration of paclitaxel protein-bound particles to rats on gestation days 7 to 17 at doses of 6 mg/m2 (approximately 2% of the daily maximum recommended human dose on a mg/m2 basis) caused embryo- and fetotoxicity, as indicated by intrauterine mortality, increased resorptions (up to 5-fold), reduced numbers of litters and live fetuses, reduction in fetal body weight and increase in fetal anomalies. Fetal anomalies included soft tissue and skeletal malformations, such as eye bulge, folded retina, microphthalmia, and dilation of brain ventricles. A lower incidence of soft tissue and skeletal malformations were also exhibited at 3 mg/m2 (approximately 1% of the daily maximum recommended human dose on a mg/m2 basis).
There are no adequate and well-controlled studies in pregnant women using ABRAXANE®. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with ABRAXANE.
Use in Males
Men should be advised to not father a child while receiving treatment with ABRAXANE (see PRECAUTIONS: Carcinogenesis, Mutagenesis, Impairment of Fertility for discussion of effects of ABRAXANE exposure on male fertility and embryonic viability).
Albumin (Human)
ABRAXANE contains albumin (human), a derivative of human blood. Based on effective donor screening and product manufacturing processes, it carries an extremely remote risk for transmission of viral diseases. A theoretical risk for transmission of Creutzfeldt-Jakob Disease (CJD) also is considered extremely remote. No cases of transmission of viral diseases or CJD have ever been identified for albumin.
PRECAUTIONS
Drug Interactions
No drug interaction studies have been conducted with ABRAXANE.
The metabolism of paclitaxel is catalyzed by CYP2C8 and CYP3A4. In the absence of formal clinical drug interaction studies, caution should be exercised when administering ABRAXANE concomitantly with medicines known to inhibit (e.g. ketoconazole and other imidazole antifungals, erythromycin, fluoxetine, gemfibrozil, cimetidine, ritonavir, saquinavir, indinavir, and nelfinavir) or induce (e.g. rifampicin, carbamazepine, phenytoin, efavirenz, nevirapine) either CYP2C8 or CYP3A4. (see CLINICAL PHARMACOLOGY).
Hematology
ABRAXANE® therapy should not be administered to patients with baseline neutrophil counts of less than 1,500 cells/mm3. In order to monitor the occurrence of myelotoxicity, it is recommended that frequent peripheral blood cell counts be performed on all patients receiving ABRAXANE. Patients should not be retreated with subsequent cycles of ABRAXANE until neutrophils recover to a level >1,500 cells/mm3 and platelets recover to a level >100,000 cells/mm3. In the case of severe neutropenia (<500 cells/mm3 for seven days or more) during a course of ABRAXANE therapy, a dose reduction for subsequent courses of therapy is recommended (see DOSAGE and ADMINISTRATION).
Nervous System
Sensory neuropathy occurs frequently with ABRAXANE. The occurrence of grade 1 or 2 sensory neuropathy does not generally require dose modification. If grade 3 sensory neuropathy develops, treatment should be withheld until resolution to grade 1 or 2 followed by a dose reduction for all subsequent courses of ABRAXANE (see DOSAGE and ADMINISTRATION).
Hepatic Impairment
Because the exposure and toxicity of paclitaxel can be increased with hepatic impairment, administration of ABRAXANE in patients with hepatic impairment should be performed with caution. The starting dose should be reduced for patients with moderate and severe hepatic impairment . (See CLINICAL PHARMACOLOGY and DOSAGE and ADMINISTRATION, Hepatic Impairment).
Injection Site Reaction
Injection site reactions occur infrequently with ABRAXANE and were mild in the randomized clinical trial. Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration.
Carcinogenesis, Mutagenesis, Impairment of Fertility
The carcinogenic potential of ABRAXANE has not been studied.
Paclitaxel has been shown to be clastogenic in vitro (chromosome aberrations in human lymphocytes) and in vivo (micronucleus test in mice). ABRAXANE was not mutagenic in the Ames test or the CHO/HGPRT gene mutation assay.
Administration of paclitaxel protein-bound particles to male rats at 42 mg/m2 on a weekly basis (approximately 16% of the daily maximum recommended human exposure on a mg/m2 basis) for 11 weeks prior to mating with untreated female rats resulted in significantly reduced fertility accompanied by decreased pregnancy rates and increased loss of embryos in mated females. A low incidence of skeletal and soft tissue fetal anomalies was also observed at doses of 3 and 12 mg/m2/week in this study (approximately 1 to 5% of the daily maximum recommended human exposure on a mg/m2 basis). Testicular atrophy/degeneration has also been observed in single-dose toxicology studies in rodents administered paclitaxel protein-bound particles at 54 mg/m2 and dogs administered 175 mg/m2 (see WARNINGS).
Pregnancy
Teratogenic Effects
Pregnancy Category D
(See WARNINGS section).
Nursing Mothers
It is not known whether paclitaxel is excreted in human milk. Following intravenous administration of carbon-14 labeled paclitaxel to rats on days 9 to 10 postpartum, concentrations of radioactivity in milk were higher than in plasma and declined in parallel with the plasma concentrations. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants, it is recommended that nursing be discontinued when receiving ABRAXANE® therapy.
Pediatric Use
The safety and effectiveness of ABRAXANE in pediatric patients have not been evaluated.
Geriatric use
Of the 229 patients in the randomized study who received ABRAXANE, 11% were at least 65 years of age and < 2% were 75 years or older. No toxicities occurred notably more frequently among elderly patients who received ABRAXANE.
Ability to Drive and Use Machines
Adverse events such as fatigue, lethargy, and malaise may affect the ability to drive and use machines.
Information for Patients
(See Patient Information Leaflet).
ADVERSE REACTIONS
The following table shows the frequency of important adverse events in the randomized comparative trial for the patients who received either single-agent ABRAXANE® or paclitaxel injection for the treatment of metastatic breast cancer.
| Percent of Patients | ||
|---|---|---|
| ABRAXANE®
260/30min† (n=229) | Paclitaxel Injection 175/3h‡,§ (n=225) |
|
|
||
| Bone Marrow | ||
| Neutropenia | ||
| < 2.0 × 109/L | 80 | 82 |
| < 0.5 × 109/L | 9 | 22 |
| Thrombocytopenia | ||
| < 100 × 109/L | 2 | 3 |
| < 50 × 109/L | <1 | <1 |
| Anemia | ||
| < 11 g/dL | 33 | 25 |
| < 8 g/dL | 1 | <1 |
| Infections | 24 | 20 |
| Febrile Neutropenia | 2 | 1 |
| Bleeding | 2 | 2 |
| Hypersensitivity Reaction¶ | ||
| All | 4 | 12 |
| Severe# | 0 | 2 |
| Cardiovascular | ||
| Vital Sign ChangesÞ | ||
| Bradycardia | <1 | <1 |
| Hypotension | 5 | 5 |
| Severe Cardiovascular Events# | 3 | 4 |
| Abnormal ECG | ||
| All patients | 60 | 52 |
| Patients with Normal Baseline | 35 | 30 |
| Respiratory | ||
| Cough | 7 | 6 |
| Dyspnea | 12 | 9 |
| Sensory Neuropathy | ||
| Any Symptoms | 71 | 56 |
| Severe Symptoms# | 10 | 2 |
| Myalgia / Arthralgia | ||
| Any Symptoms | 44 | 49 |
| Severe Symptoms# | 8 | 4 |
| Asthenia | ||
| Any Symptoms | 47 | 39 |
| Severe Symptoms# | 8 | 3 |
| Fluid Retention/Edema | ||
| Any Symptoms | 10 | 8 |
| Severe Symptoms# | 0 | <1 |
| Gastrointestinal | ||
| Nausea | ||
| Any symptoms | 30 | 22 |
| Severe symptoms# | 3 | <1 |
| Vomiting | ||
| Any symptoms | 18 | 10 |
| Severe Symptoms# | 4 | 1 |
| Diarrhea | ||
| Any Symptoms | 27 | 15 |
| Severe Symptoms# | <1 | 1 |
| Mucositis | ||
| Any Symptoms | 7 | 6 |
| Severe Symptoms# | <1 | 0 |
| Alopecia | 90 | 94 |
| Hepatic (Patients with Normal Baseline) | ||
| Bilirubin Elevations | 7 | 7 |
| Alkaline Phosphatase Elevations | 36 | 31 |
| AST (SGOT) Elevations | 39 | 32 |
| Injection Site Reaction | <1 | 1 |
Myelosuppression and sensory neuropathy were dose related.
Adverse Event Experiences by Body System
Unless otherwise noted, the following discussion refers to the primary safety database of 229 patients with metastatic breast cancer treated with single-agent ABRAXANE® in the randomized controlled trial. The frequency and severity of important adverse events for the study are presented above in tabular form. In some instances, rare severe events observed with paclitaxel injection may be expected to occur with ABRAXANE.
Hematologic
Neutropenia, the most important hematologic toxicity, was dose dependent and reversible. Among patients with metastatic breast cancer in the randomized trial, neutrophil counts declined below 500 cells/mm3 (Grade 4) in 9% of the patients treated with a dose of 260 mg/m2 compared to 22% in patients receiving paclitaxel injection at a dose of 175 mg/m2.
In the randomized metastatic breast cancer study, infectious episodes were reported in 24% of the patients treated with a dose of 260 mg/m2 given as a 30-minute infusion. Oral candidiasis, respiratory tract infections and pneumonia were the most frequently reported infectious complications. Febrile neutropenia was reported in 2% of patients in the ABRAXANE arm and 1% of patients in the paclitaxel injection arm.
Thrombocytopenia was uncommon. In the randomized metastatic breast cancer study, bleeding episodes were reported in 2% of the patients in each treatment arm.
Anemia (Hb <11 g/dL) was observed in 33% of patients treated with ABRAXANE in the randomized trial and was severe (Hb <8 g/dL) in 1% of the cases. Among all patients with normal baseline hemoglobin, 31% became anemic on study and 1% had severe anemia.
Rare reports of pancytopenia have been observed in clinical trials and during postmarketing surveillance of ABRAXANE.
Hypersensitivity Reactions (HSRs)
In the randomized controlled metastatic breast cancer study, Grade 1 or 2 HSRs occurred on the day of ABRAXANE administration and consisted of dyspnea (1%) and flushing, hypotension, chest pain, and arrhythmia (all <1%). The use of ABRAXANE® in patients previously exhibiting hypersensitivity to paclitaxel injection or human albumin has not been studied.
During postmarketing surveillance, rare occurrences of severe hypersensitivity reactions have been reported with ABRAXANE. The use of ABRAXANE in patients previously exhibiting hypersensitivity to paclitaxel injection or human albumin has not been studied. Patients who experience a severe hypersensitivity reaction to ABRAXANE should not be rechallenged with the drug.
Cardiovascular
Hypotension, during the 30-minute infusion, occurred in 5% of patients in the randomized metastatic breast cancer trial. Bradycardia, during the 30-minute infusion, occurred in <1% of patients. These vital sign changes most often caused no symptoms and required neither specific therapy nor treatment discontinuation.
Severe cardiovascular events possibly related to single-agent ABRAXANE occurred in approximately 3% of patients in the randomized trial. These events included chest pain, cardiac arrest, supraventricular tachycardia, edema, thrombosis, pulmonary thromboembolism, pulmonary emboli, and hypertension. Cases of cerebrovascular attacks (strokes) and transient ischemic attacks have been reported rarely.
Electrocardiogram (ECG) abnormalities were common among patients at baseline. ECG abnormalities on study did not usually result in symptoms, were not dose-limiting, and required no intervention. ECG abnormalities were noted in 60% of patients in the metastatic breast cancer randomized trial. Among patients with a normal ECG prior to study entry, 35% of all patients developed an abnormal tracing while on study. The most frequently reported ECG modifications were non-specific repolarization abnormalities, sinus bradycardia, and sinus tachycardia.
During postmarketing surveillance, rare reports of congestive heart failure and left ventricular dysfunction have been observed among individuals receiving ABRAXANE. Most of the individuals were previously exposed to cardiotoxic drugs, such as anthracyclines, or had underlying cardiac history.
Respiratory
Reports of dyspnea (12%) and cough (6%) were reported after treatment with ABRAXANE in the randomized trial. Rare reports (<1%) of pneumothorax were reported after treatment with ABRAXANE. Rare reports of interstitial pneumonia, lung fibrosis, and pulmonary embolism have been received as part of the continuing surveillance of paclitaxel injection safety and may occur following ABRAXANE treatment. Rare reports of radiation pneumonitis have been received in paclitaxel injection patients receiving concurrent radiotherapy. There is no experience with the use of ABRAXANE with concurrent radiotherapy.
Neurologic
The frequency and severity of neurologic manifestations were influenced by prior and/or concomitant therapy with neurotoxic agents.
In general, the frequency and severity of neurologic manifestations were dose-dependent in patients receiving single-agent ABRAXANE®. In the randomized trial, sensory neuropathy was observed in 71% of patients (10% severe) in the ABRAXANE arm and in 56% of patients (2% severe) in the paclitaxel injection arm. The frequency of sensory neuropathy increased with cumulative dose. Sensory neuropathy was the cause of ABRAXANE discontinuation in 7/229 (3%) patients in the randomized trial. In the randomized comparative study, 24 patients (10%) treated with ABRAXANE developed Grade 3 peripheral neuropathy; of these patients, 14 had documented improvement after a median of 22 days; 10 patients resumed treatment at a reduced dose of ABRAXANE and 2 discontinued due to peripheral neuropathy. Of the 10 patients without documented improvement, 4 discontinued the study due to peripheral neuropathy.
No incidences of grade 4 sensory neuropathies were reported in the clinical trial. Only one incident of motor neuropathy (grade 2) was observed in either arm of the controlled trial.
Cranial nerve palsies and vocal cord paresis have been reported during postmarketing surveillance of ABRAXANE. Because these events have been reported during clinical practice, true estimates of frequency cannot be made and a causal relationship to the events has not been established.
Reports of autonomic neuropathy resulting in paralytic ileus have been received as part of the continuing surveillance of paclitaxel injection safety.
Ocular/visual disturbances occurred in 13% of all patients (n=366) treated with ABRAXANE in single arm and randomized trials and 1% were severe. The severe cases (keratitis and blurred vision) were reported in patients in a single arm study who received higher doses than those recommended (300 or 375 mg/m2). These effects generally have been reversible. However, rare reports in the literature of abnormal visual evoked potentials in patients treated with paclitaxel injection have suggested persistent optic nerve damage.
Arthralgia/Myalgia
Forty-four percent of patients treated in the randomized trial experienced arthralgia/myalgia; 8% experienced severe symptoms. The symptoms were usually transient, occurred two or three days after ABRAXANE® administration, and resolved within a few days.
Hepatic
Among patients with normal baseline liver function treated with ABRAXANE in the randomized trial, 7%, 36%, and 39% had elevations in bilirubin, alkaline phosphatase, and AST (SGOT), respectively. Grade 3 or 4 elevations in GGT were reported for 14% of patients treated with ABRAXANE and 10% of patients treated with paclitaxel injection in the randomized trial.
Rare reports of hepatic necrosis and hepatic encephalopathy leading to death have been received as part of the continuing surveillance of paclitaxel injection safety and may occur following ABRAXANE treatment.
Renal
Overall 11% of patients experienced creatinine elevation, 1% severe. No discontinuations, dose reductions, or dose delays were caused by renal toxicities.
Gastrointestinal (GI)
Nausea/vomiting, diarrhea, and mucositis were reported by 33%, 27%, and 7% of ABRAXANE treated patients in the randomized trial.
Rare reports of intestinal obstruction, intestinal perforation, pancreatitis, and ischemic colitis have been received as part of the continuing surveillance of paclitaxel injection safety and may occur following ABRAXANE treatment. Rare reports of neutropenic enterocolitis (typhlitis), despite the coadministration of G-CSF, were observed in patients treated with paclitaxel injection alone and in combination with other chemotherapeutic agents.
Injection Site Reaction
Injection site reactions have occurred infrequently with ABRAXANE and were mild in the randomized clinical trial. Recurrence of skin reactions at a site of previous extravasation following administration of paclitaxel injection at a different site, i.e., "recall", has been reported rarely.
Rare reports of more severe events such as phlebitis, cellulitis, induration, skin exfoliation, necrosis, and fibrosis have been received as part of the continuing surveillance of paclitaxel injection safety. In some cases the onset of the injection site reaction in paclitaxel injection patients either occurred during a prolonged infusion or was delayed by a week to ten days.
Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration.
Asthenia
Asthenia was reported in 47% of patients (8% severe) treated with ABRAXANE® in the randomized trial. Asthenia included reports of asthenia, fatigue, weakness, lethargy and malaise.
Other Clinical Events
Rare cases of cardiac ischemia/infarction and thrombosis/embolism possibly related to ABRAXANE treatment have been reported. Alopecia was observed in almost all of the patients. Nail changes (changes in pigmentation or discoloration of nail bed) were uncommon. Edema (fluid retention) was infrequent (10% of randomized trial patients); no patients had severe edema. In clinical trials and during postmarketing surveillance of ABRAXANE, dehydration was common and pyrexia was very common.
The following rare adverse events have been reported as part of the continuing surveillance of paclitaxel injection safety and may occur following ABRAXANE treatment: skin abnormalities related to radiation recall as well as reports of Stevens-Johnson syndrome, toxic epidermal necrolysis, conjunctivitis, and increased lacrimation. As part of the continuing surveillance of ABRAXANE, skin reactions including generalized or maculo-papular rash, erythema, and pruritis have been observed. Additionally, there have been case reports of photosensitivity reactions, radiation recall phenomenon, and in some patients previously exposed to capecitabine, reports of palmar-plantar erythrodysaesthesiae. Because these events have been reported during clinical practice, true estimates of frequency cannot be made and a causal relationship to the events has not been established.
Accidental Exposure
No reports of accidental exposure to ABRAXANE® have been received. However, upon inhalation of paclitaxel, dyspnea, chest pain, burning eyes, sore throat, and nausea have been reported. Following topical exposure, events have included tingling, burning, and redness.
OVERDOSAGE
There is no known antidote for ABRAXANE overdosage. The primary anticipated complications of overdosage would consist of bone marrow suppression, sensory neurotoxicity, and mucositis.
DOSAGE AND ADMINISTRATION
After failure of combination chemotherapy for metastatic breast cancer or relapse within 6 months of adjuvant chemotherapy, the recommended regimen for ABRAXANE for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) is 260 mg/m2 administered intravenously over 30 minutes every 3 weeks.
Hepatic Impairment
No dose adjustment is necessary for patients with mild hepatic impairment. Patients with moderate and severe hepatic impairment treated with ABRAXANE may be at increased risk of toxicities known to paclitaxel. Patients should not receive ABRAXANE if AST > 10 × ULN or bilirubin > 5.0 × ULN. Recommendations for dosage adjustment for the first course of therapy are shown in Table 4. The dose of ABRAXANE can be increased up to 200 mg/m2 in patients with severe hepatic impairment in subsequent cycles based on individual tolerance. Patients should be monitored closely. (see CLINICAL PHARMACOLOGY : Hepatic Impairment and PRECAUTIONS: Hepatic Impairment)
| SGOT (AST) Levels | Bilirubin Levels | ABRAXANE* | ||
|---|---|---|---|---|
| Mild | <10 × ULN | AND | >ULN to ≤ 1.25 × ULN | 260 mg/m2 |
| Moderate | <10 × ULN | 1.26 to 2.0 × ULN | 200 mg/m2 | |
| Severe | <10 × ULN | 2.01 to 5.0 × ULN | 130 mg/m2† | |
| > 10 × ULN | OR | > 5.0 × ULN | not eligible | |
Dose Reduction
Patients who experience severe neutropenia (neutrophil <500 cells/mm3 for a week or longer) or severe sensory neuropathy during ABRAXANE therapy should have dosage reduced to 220 mg/m2 for subsequent courses of ABRAXANE. For recurrence of severe neutropenia or severe sensory neuropathy, additional dose reduction should be made to 180 mg/m2. For grade 3 sensory neuropathy hold treatment until resolution to grade 1 or 2, followed by a dose reduction for all subsequent courses of ABRAXANE.
Preparation and Administration Precautions
ABRAXANE is a cytotoxic anticancer drug and, as with other potentially toxic paclitaxel compounds, caution should be exercised in handling ABRAXANE. The use of gloves is recommended. If ABRAXANE (lyophilized cake or reconstituted suspension) contacts the skin, wash the skin immediately and thoroughly with soap and water. Following topical exposure to paclitaxel, events may include tingling, burning and redness. If ABRAXANE® contacts mucous membranes, the membranes should be flushed thoroughly with water.
Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration. Limiting the infusion of ABRAXANE to 30 minutes, as directed, reduces the likelihood of infusion-related reactions (see PRECAUTIONS: Injection Site Reaction).
No premedication to prevent hypersensitivity reactions is required prior to administration of ABRAXANE.
Preparation for Intravenous Administration
ABRAXANE is supplied as a sterile lyophilized powder for reconstitution before use. AVOID ERRORS, READ ENTIRE PREPARATION INSTRUCTIONS PRIOR TO RECONSTITUTION.
|

Each mL of the reconstituted formulation will contain 5 mg/mL paclitaxel.
Calculate the exact total dosing volume of 5 mg/mL suspension required for the patient: Dosing volume (mL) = Total dose (mg)/5 (mg/mL)
The reconstituted suspension should be milky and homogenous without visible particulates. If particulates or settling are visible, the vial should be gently inverted again to ensure complete resuspension prior to use. Discard the reconstituted suspension if precipitates are observed. Discard any unused portion.
Inject the appropriate amount of reconstituted ABRAXANE® into an empty, sterile IV bag (plasticized polyvinyl chloride (PVC) containers, PVC or non-PVC type IV bag). The use of specialized DEHP-free solution containers or administration sets is not necessary to prepare or administer ABRAXANE infusions. The use of an in-line filter is not recommended.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.
Stability
Unopened vials of ABRAXANE are stable until the date indicated on the package when stored between 20°C to 25°C (68°F to 77°F), in the original package. Neither freezing nor refrigeration adversely affects the stability of the product.
Stability of Reconstituted Suspension in the Vial
Reconstituted ABRAXANE should be used immediately, but may be refrigerated at 2°C to 8°C (36°F to 46°F) for a maximum of 8 hours if necessary. If not used immediately, each vial of reconstituted suspension should be replaced in the original carton to protect it from bright light. Discard any unused portion.
Stability of Reconstituted Suspension in the Infusion Bag
The suspension for infusion prepared as recommended in an infusion bag should be used immediately, but may be stored at ambient temperature (approximately 25° C) and lighting conditions for up to 8 hours.
HOW SUPPLIED
Product No. 103450
NDC No. 68817-134-50 100 mg of paclitaxel in a single use vial, individually packaged in a carton.
Storage
Store the vials in original cartons at 20° C to 25° C (68° F to 77°F). Retain in the original package to protect from bright light.
Handling and Disposal
Procedures for proper handling and disposal of anticancer drugs should be considered. Several guidelines on this subject have been published.1-8 There is no general agreement that all of the procedures recommended in the guidelines are necessary or appropriate.
U.S. Patent Numbers: 5,439,686; 5,498,421; 6,096,331; 6,506,405;
6,537,579; 6,749,868; 6,753,006
REFERENCES
- Recommendations for the Safe Handling of Parenteral Antineoplastic Drugs. Publication No. 83-2621. For sale by the Superintendent of Documents, US Government NIH Printing Office, Washington, DC 20402.
- AMA Council Report. Guidelines for Handling Parenteral Antineoplastics. JAMA, 1985; 253(11):1590-1592.
- National Study Commission on Cytotoxic Exposure Recommendations for Handling Cytotoxic Agents. Available from Louis R Jeffrey, ScD, Chairman, National Study Commission on Cytotoxic Exposure. Massachusetts College of Pharmacy and Allied Health Sciences. 179 Longwood Avenue, Boston, Massachusetts 02115.
- Clinical Oncological Society of Australia. Guidelines and Recommendations for Safe Handling of Antineoplastic Agents. Med J Australia, 1983; 1:426-428.
- Jones RB, et al: Safe Handling of Chemotherapeutic Agents: A Report from the Mount Sinai Medical Center. CA-A Cancer Journal for Clinicians, 1983; (Sept/Oct) 258-263.
- American Society of Hospital Pharmacists Technical Assistance Bulletin on Handling Cytotoxic and Hazardous Drugs. Am J Hosp Pharm, 1990; 47:1033-1049.
- Controlling Occupational Exposure to Hazardous Drugs. (OSHA WORK-PRACTICE GUIDELINES.) Am J Health-Syst Pharm, 1996; 53:1669-1686.
- ONS Clinical Practice Committee. Cancer Chemotherapy Guidelines and Recommendations for Practice Pittsburgh, Pa: Oncology Nursing Society; 1999:32-41.
Revised: March 2010
ABRAXIS
BIOSCIENCE
Distributed by Abraxis BioScience, LLC
Bridgewater, NJ 08807
PATIENT INFORMATION
ABRAXANE® for Injectable Suspension
[generic name = (paclitaxel protein-bound particles for injectable suspension) (albumin-bound)]
WHAT IS ABRAXANE?
ABRAXANE is a prescription cancer medicine. It is injected into a vein and it is used to treat advanced breast cancer.
WHAT IS CANCER?
Under normal conditions, the cells in your body divide and grow in an orderly, controlled way. Cell division and growth are necessary for the human body to perform its functions and to repair itself, when necessary. Cancer cells are different from normal cells because they are not able to control their own growth. The reasons for this abnormal growth are not yet fully understood. A tumor is a mass of unhealthy cells that are dividing and growing fast and in an uncontrolled way. When a tumor invades surrounding healthy body tissue it is known as a malignant tumor. A malignant tumor can spread (metastasize) from its original site to other parts of the body if not found and treated early.
HOW DOES ABRAXANE WORK?
ABRAXANE is a type of medical treatment called chemotherapy. The purpose of chemotherapy is to kill cancer cells or prevent their growth.
All cells, whether they are healthy cells or cancer cells, go through several stages of growth. During one of the stages, the cell starts to divide. ABRAXANE may stop the cells from dividing and growing, so they eventually die. In addition, normal cells may also be affected by ABRAXANE causing some of the side effects. (see WHAT ARE THE POSSIBLE SIDE EFFECTS OF ABRAXANE? below).
WHO SHOULD NOT TAKE ABRAXANE?
ABRAXANE should not be given to patients with dangerously low white blood cell counts.
HOW IS ABRAXANE® GIVEN?
ABRAXANE is injected into a vein [intravenous (I.V.) infusion] over 30 minutes.
WHAT PREMEDICATION IS REQUIRED WITH ABRAXANE?
While reactions can occur to any medication, severe allergic reactions to ABRAXANE are uncommon and premedication is not required. However, you should make your doctor aware of any allergies you may have so he/she can determine the course of action required.
WHAT ARE THE POSSIBLE SIDE EFFECTS OF ABRAXANE?
Most patients taking ABRAXANE will experience side effects, although it is not always possible to tell whether such effects are caused by ABRAXANE, another medicine they may be taking, or the cancer itself. Important side effects are described below; however, some patients may experience other side effects that are less common. Report any unusual symptoms to your doctor.
Important side effects observed in studies of patients taking ABRAXANE were as follows:
Hair Loss: Complete hair loss, or alopecia, almost always occurs with ABRAXANE. This usually involves the loss of eyebrows, eyelashes, and pubic hair, as well as scalp hair. It can occur suddenly after treatment has begun, but usually happens 14 to 21 days after treatment. Hair generally grows back after you've finished your ABRAXANE treatment.
Infections Due to Low White Blood Cell Count: Among the body's defenses against bacterial infections are white blood cells. Between your ABRAXANE treatment cycles, you will often have blood tests to check your white blood cell counts. ABRAXANE usually causes a brief drop in white blood cells. If you have a fever (temperature above 100.4°F) or other sign of infection, tell your doctor right away. Sometimes serious infections develop that require treatment in the hospital with antibiotics. Serious illness or death could result if such infections are not treated when white blood cell counts are low.
Numbness, Tingling, or Burning in the Hands and/or Feet (Neuropathy): These symptoms occur often with ABRAXANE® and usually get better or go away without medication within three weeks of interrupting treatment. Be sure to tell your doctor about any numbness, tingling or burning that you have in your hands or feet so that he/she can decide the best approach for relief of your symptoms. Sometimes it is necessary to interrupt treatment with ABRAXANE until these symptoms improve. After improvement, treatment can be restarted at a lower dose.
Fatigue and Weakness: ABRAXANE may cause asthenia, fatigue, weakness, lethargy and malaise. These side effects are usually self-limited and do not require dose modification or interruption.
Low Red Blood Cell Count: Red blood cells deliver oxygen to tissues throughout all parts of the body and take carbon dioxide from the tissues by using a protein called hemoglobin. A lowering of the volume of red blood cells may occur following ABRAXANE treatment causing anemia. Some patients may need a blood transfusion to treat the anemia. Patients can feel tired, tire easily, appear pale, and become short of breath. Contact your doctor if you experience any of these symptoms following ABRAXANE treatment.
Mouth or Lip Sores (Mucositis): Some patients develop redness and/or sores in the mouth or on the lips. These symptoms might occur a few days after the ABRAXANE treatment and usually decrease or disappear within one week. Talk with your doctor about proper mouth care and other ways to prevent or reduce your chances of developing mucositis.
Joint and Muscle Pain: You may get joint and muscle pain a few days after your ABRAXANE treatment. These symptoms usually disappear in a few days. Although pain medicine may not be necessary, tell your doctor if you are uncomfortable.
Stomach Upset and Diarrhea: Some patients experience nausea, vomiting, and/or diarrhea following ABRAXANE use. If you experience nausea or stomach upset, tell your doctor because medicines can be given that almost always reduce or eliminate these symptoms. Diarrhea will usually disappear without treatment; however, if you experience severe abdominal or stomach area pain and/or severe diarrhea, tell your doctor right away.
Heart and Blood Vessel (Cardiovascular) Effects: ABRAXANE® may cause a drop in heart rate (bradycardia) and low blood pressure (hypotension). The patient usually does not notice these changes. These changes usually do not require treatment. You should notify your doctor if you have a history of heart disease.
Irritation at the Injection Site: ABRAXANE may cause irritation at the site where it enters the vein. Reactions may include discomfort, redness, swelling, inflammation (of the surrounding skin or of the vein itself), and ulceration (open sores). These reactions are usually caused by the I.V. (intravenous) fluid leaking into the surrounding area. If you notice anything unusual at the site of the injection (needle), either during or after treatment, tell your doctor right away.
Ability to Drive and Use Machines: Adverse events may affect your ability to drive and use machines.
Talk with your doctor or other healthcare professional to discuss ways to prevent or reduce some of these side effects. Because this leaflet does not include all possible side effects that can occur with ABRAXANE, it is important to talk with your doctor about other possible side effects.
CAN I TAKE ABRAXANE IF I AM PREGNANT OR NURSING A BABY?
ABRAXANE could harm the fetus when given to a pregnant woman. Women should avoid becoming pregnant while they are undergoing treatment with ABRAXANE. Tell your doctor if you become pregnant or plan to become pregnant while taking ABRAXANE.
Men should be advised not to father a child while receiving treatment with ABRAXANE.
Because studies have shown the active agent (paclitaxel) in ABRAXANE to be present in the breast milk of animals receiving the active agent, it may be present in human breast milk as well. Therefore, nursing a baby while taking ABRAXANE is NOT recommended. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants, it is recommended that nursing be discontinued when receiving ABRAXANE therapy.
This medicine was prescribed for your particular condition. This summary does not include everything there is to know about ABRAXANE®. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information Leaflet. If you have questions or concerns, or want more information about ABRAXANE, your doctor and pharmacist have the complete prescribing information upon which this guide is based. You may want to read it and discuss it with your doctor. Remember, no written summary can replace careful discussion with your doctor.
ABRAXIS
BIOSCIENCE
Distributed by Abraxis BioScience, LLC
Bridgewater, NJ 08807
This Patient Information Leaflet has been approved by the U.S. Food and Drug Administration.
Based on: ABRAXANE Package Insert Revised: March 2010
Revised: March 2010
PRINCIPAL DISPLAY PANEL - 100 mg Vial
NDC 68817-134-50
103450
Abraxane®
for Injectable Suspension
(paclitaxel protein-bound particles for injectable suspension)
(albumin-bound)
100 mg
Single Use Vial
For IV Use Only
Rx only
Functional properties differ from other
paclitaxel products. DO NOT SUBSTITUTE.

| ABRAXANE
paclitaxel injection, powder, lyophilized, for suspension |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021660 | 02/10/2005 | |
| Labeler - Abraxis BioScience, LLC (832108497) |