NEOSTIGMINE METHYLSULFATE- neostigmine methylsulfate injection
Cardinal Health
Disclaimer: This drug has not been found by FDA to be safe and effective, and this labeling has not been approved by FDA. For further information about unapproved drugs, click here.
----------
Neostigmine
Methylsulfate Injection, USP
DESCRIPTION
Neostigmine methylsulfate is the dimethylcarbamate of (m-hydroxyphenyl) trimethylammonium methylsulfate.
The chemical structure is:
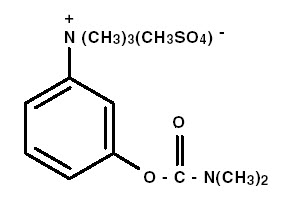
C13H22N2O6S MW 334.39
Neostigmine methylsulfate, an anticholinesterase agent, is a bitter tasting, white crystalline powder and is very soluble in water and soluble in alcohol. Neostigmine Methylsulfate Injection is a sterile solution intended for intramuscular, subcutaneous or slow intravenous use.
Each mL of the 1:1000 concentration contains neostigmine methylsulfate 1 mg, methylparaben 1.8 mg and propylparaben 0.2 mg in water for injection qs; pH adjusted with sodium hydroxide if necessary. pH: 5.0-6.5. Each mL of the 1:2000 concentration contains neostigmine methylsulfate 0.5 mg, methylparaben 1.8 mg, propylparaben 0.2 mg, sodium acetate anhydrous 0.2 mg, water for injection qs; pH adjusted with acetic acid and/or sodium hydroxide if necessary. pH: 5.0-6.5.
CLINICAL PHARMACOLOGY
Neostigmine inhibits the hydrolysis of acetylcholine by competing with acetylcholine for attachment to acetylcholinesterase at sites of cholinergic transmission. It enhances cholinergic action by facilitating the transmission of impulses across neuromuscular junctions. It also has a direct cholinominetic effect on skeletal muscle and possibly on autonomic ganglion cells and neurons of the central nervous system. Neostigmine undergoes hydrolysis by cholinesterase and is also metabolized by microsomal enzymes in the liver. Protein binding to human serum albumin ranges from 15 to 25 percent.
Following intramuscular administration, neostigimine is rapidly absorbed and eliminated. In a study of five patients with myasthenia gravis, peak plasma levels were observed at 30 minutes and the half-life ranged from 51 to 90 minutes. Approximately 80 percent of the drug was eliminated in urine within 24 hours; approximately 50 percent as the unchanged drug and 30 percent as metabolites. Following intravenous administration, plasma half-life ranges from 47 to 60 minutes have been reported with a mean half-life of 53 minutes.
The clinical effects of neostigmine usually begin within 20 to 30 minutes after intramuscular injection and last from 2.5 to 4 hours.
INDICATIONS AND USAGE
Neostigmine Methylsulfate Injection is indicated for:
-the symptomatic control of myasthenia gravis when oral therapy is impractical.
-the prevention and treatment of postoperative distention and urinary retention after mechanical obstruction has been excluded.
-reversal of effects of nondepolarizing neuromuscular blocking agents (e.g., tubocurarine, metocurine, gallamine or pancuronium) after surgery.
CONTRAINDICATIONS
Neostigmine Methylsulfate Injection is contraindicated in patients with known hypersensitivity to the drug. It is also contraindicated in patients with peritonitis or mechanical obstruction of the intestinal or urinary tract.
WARNINGS
Neostigmine should be used with caution in patients with epilepsy, bronchial asthma, bradycardia, recent coronary occlusion, vagotonia, hyperthyroidism, cardiac arrhythmias or peptic ulcer. When large doses of neostigmine are administered, the prior or simultaneous injection of atropine sulfate may be advisable. Separate syringes should be used for neostigmine and atropine. Because of the possibility of hypersensitivity in an occasional patient, atropine and antishock medication should always be readily available.
PRECAUTIONS
General
It is important to differentiate between myasthenic crisis and cholinergic crisis caused by overdosage of neostigmine. Both conditions result in extreme muscle weakness but require radically different treatment. (See OVERDOSAGE section).
Drug Interactions
Neostigmine does not antagonize, and may in fact prolong, the phase I block of depolarizing muscle relaxants such as succinylcholine or decamethonium. Certain antibiotics, especially neomycin, streptomycin and kanamycin, have a mild but definite nondepolarizing blocking action which may accentuate neuromuscular block. These antibiotics should be used in the myasthenic patient only where definitely indicated, and then careful adjustment should be made of the anticholinesterase dosage. Local and some general anesthetics, antiarrhythmic agents and other drugs that interfere with neuromuscular transmission should be used cautiously, if at all, in patients with myasthenia gravis; the dose of neostigmine may have to be increased accordingly.
Carcinogenesis, Mutagenesis and Impairment of Fertility
There have been no studies with neostigmine which would permit an evaluation of its carcinogenic or mutagenic potential. Studies on the effect of neostigmine on fertility and reproduction have not been performed.
Pregnancy
TERATOGENIC EFFECTS - PREGNANCY CATEGORY C
There are no adequate or well-controlled studies of neostigmine in either laboratory animals or in pregnant women. It is not known whether neostigmine can cause fetal harm when administered to pregnant women or can affect reproductive capacity. Neostigmine should be given to pregnant women only if clearly needed.
Nursing Mothers
It is not known whether neostigmine is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions from neostigmine in nursing infants, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
ADVERSE REACTIONS
Side effects are generally due to an exaggeration of pharmacological effects of which salivation and fasciculation are the most common. Bowel cramps and diarrhea may also occur.
The following additional adverse reactions have been reported following the use of either neostigmine bromide or neostigmine methylsulfate.
Allergic: Allergic reaction and anaphylaxis.
Neurologic: Dizziness, convulsions, loss of consciousness, drowsiness, headache, dysarthria, miosis and visual changes.
Cardiovascular: Cardiac arrhythmias (including bradycardia, tachycardia, A-V block and nodal rhythm) and nonspecific EKG changes have been reported, as well as cardiac arrest, syncope and hypotension. These have been predominantly noted following the use of the injectable form of neostigmine.
Respiratory: Increased oral, pharyngeal and bronchial secretions, dyspnea, respiratory depression, respiratory arrest and bronchospasm.
Dermatologic: Rash and urticaria.
Gastrointestinal: Nausea, emesis, flatulence and increased peristalsis.
Genitourinary: Urinary frequency.
Musculoskeletal: Muscle cramps and spasms, arthralgia.
Miscellaneous: Diaphoresis, flushing and weakness.
OVERDOSAGE
Overdosage of neostigmine can cause cholinergic crisis, which is characterized by increasing muscle weakness, and through involvement of the muscles of respiration, may result in death. Myasthenic crisis, due to an increase in the severity of the disease, is also accompanied by extreme muscle weakness and may be difficult to distinguish from cholinergic crisis on a symptomatic basis. However, such differentiation is extremely important because increases in the dose of neostigmine or other drugs in this class, in the presence of cholinergic crisis or of a refractory or "insensitive" state, could have grave consequences. The two types of crisis may be differentiated by the use of edrophonium chloride as well as by clinical judgement.
Treatment of the two conditions differs radically. Whereas the presence of myasthenic crisis requires more intensive anticholinesterase therapy, cholinergic crisis calls for the prompt withdrawal of all drugs of this type. The immediate use of atropine in cholinergic crisis is also recommended.
Atropine may also be used to abolish or minimize gastrointestinal side effects or other muscarinic reactions; but such use by masking signs of overdosage, can lead to inadvertent induction of cholinergic crisis.
The LD50 of neostigmine methylsulfate in mice is 0.3 ± 0.02 mg/kg intravenously, 0.54 ± 0.03 mg/kg subcutaneously and 0.395 ± 0.025 mg/kg intramuscularly; in rats the LD50 is 0.315 ± 0.019 mg/kg intravenously, 0.445 ± 0.032 mg/kg subcutaneously and 0.423 ± 0.032 mg/kg intramuscularly.
DOSAGE AND ADMINISTRATION
Symptomatic control of myasthenia gravis: One mL of the 1:2000 solution (0.5 mg) subcutaneously or intramuscularly. Subsequent doses should be based on the individual patient's response. In most patients, however, oral treatment with neostigmine bromide tablets, 15 mg each, is adequate for control of symtoms.
Prevention of postoperative distention and urinary retention: 0.25 mg subcutaneously or intramuscularly as soon as possible after operation; repeat every 4 to 6 hours for two or three days.
Treatment of postoperative distention: One mL of 1:2000 solution (0.5 mg) subcutaneously or intramuscularly, as required.
Treatment of urinary retention: One mL of the 1:2000 solution (0.5 mg) subcutaneously or intramuscularly. If urination does not occur within an hour, the patient should be catheterized. After the patient has voided, or the bladder has been emptied, continue the 0.5 mg injections every three hours for at least 5 injections.
Reversal of Effects on Nondepolarizing Neuromuscular Blocking Agents: When Neostigmine Methylsulfate Injection is administered intravenously, it is recommended that atropine sulfate (0.6 to 1.2 mg) also be given intravenously using separate syringes. Some authorities have recommended that the atropine be injected several minutes before the neostigmine rather than concomitantly. The usual dose is 0.5 to 2 mg Neostigmine Methylsulfate Injection given by slow intravenous injection, repeated as required. Only in exceptional cases should the total dose neostigmine exceed 5 mg. It is recommended that the patient be well ventilated and a patent airway maintained until complete recovery of normal respiration is assured. The optimum time for administration of the drug is during hyperventilation when the carbon dioxide level of the blood is low. It should never be administered in the presence of high concentrations of halothane or cyclopropane. In cardiac cases and severely ill patients, it is advisable to titrate the exact dose of neostigmine required, using a peripheral nerve stimulator device. In the presence of bradycardia, the pulse rate should be increased to about 80/minute with atropine before administering neostigmine.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
HOW SUPPLIED
Neostigmine Methylsulfate Injection, USP is available in the following:
1:1000 (1 mg/mL)
10 mL Multiple Dose Vial packaged in 10s (NDC 0641-6077-10)
1:2000 (0.5 mg/mL)
10 mL Multiple Dose Vial packaged in 10s (NDC 0641-6076-10)

| NEOSTIGMINE METHYLSULFATE
neostigmine methylsulfate injection |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Cardinal Health (188557102) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Cardinal Health | 188557102 | REPACK(55154-2882) | |