OXYCODONE HYDROCHLORIDE IMMEDIATE-RELEASE
-
oxycodone hydrochloride capsule
Mallinckrodt, Inc.
Disclaimer: This drug has not been found by FDA to be safe and effective, and this labeling has not been approved by FDA. For further information about unapproved drugs, click here.
----------
DESCRIPTION
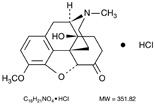
Oxycodone hydrochloride is 4,5α-epoxy-14-hydroxy-3-methoxy-17-methylmorphinan-6-one hydrochloride, a white, odorless, crystalline powder which is derived from the opium alkaloid, thebaine, and may be represented by the structural formula:
Each Oxycodone Hydrochloride Immediate-Release Oral Capsule contains:
Oxycodone Hydrochloride USP .................5 mg
In addition, each capsule contains the following inactive ingredients: black iron oxide, gelatin, lactose, red iron oxide, silicon dioxide, stearic acid, titanium dioxide, yellow iron oxide.
ACTIONS
The analgesic ingredient, oxycodone, is a semisynthetic narcotic with multiple actions qualitatively similar to those of morphine; the most prominent of these involve the central nervous system and organs composed of smooth muscle. The principal actions of therapeutic value of oxycodone are analgesia and sedation.
CLINICAL PHARMACOLOGY
Central Nervous System
Oxycodone is a pure agonist opioid whose principal therapeutic action is analgesia. Other therapeutic effects of oxycodone include anxiolysis, euphoria and feelings of relaxation. Like all pure opioid agonists, there is no ceiling effect to analgesia, such as is seen with partial agonists or non-opioid analgesics.
The precise mechanism of the analgesic action is unknown. However, specific CNS opioid receptors for endogenous compounds with opioid-like activity have been identified throughout the brain and spinal cord and play a role in the analgesic effects of this drug.
Oxycodone produces respiratory depression by direct action on brain stem respiratory centers. The respiratory depression involves both a reduction in the responsiveness of the brain stem respiratory centers to increases in carbon dioxide tension and to electrical stimulation.
Oxycodone depresses the cough reflex by direct effect on the cough center in the medulla. Antitussive effects may occur with doses lower than those usually required for analgesia.
Oxycodone causes miosis, even in total darkness. Pinpoint pupils are a sign of opioid overdose but are not pathognomonic. Marked mydriasis rather than miosis may be seen due to hypoxia in overdose situations.
Gastrointestinal Tract and Other Smooth Muscle
Oxycodone causes a reduction in motility associated with an increase in smooth muscle tone in the antrum of the stomach and duodenum. Digestion of food in the small intestine is delayed and propulsive contractions are decreased. Propulsive peristaltic waves in the colon are decreased, while tone may be increased to the point of spasm resulting in constipation. Other opioid-induced effects may include a reduction in gastric, biliary and pancreatic secretions, spasm of sphincter of Oddi, and transient elevations in serum amylase.
Cardiovascular System
Oxycodone may produce release of histamine with or without associated peripheral vasodilation. Manifestations of histamine release and/or peripheral vasodilation may include pruritus, flushing, red eyes, sweating, and/or orthostatic hypotension.
Concentration—Effect Relationships (Pharmacodynamics)
Studies in normal volunteers and patients reveal predictable relationships between oxycodone dosage and plasma oxycodone concentrations, as well as between concentration and certain expected opioid effects. In normal volunteers these include pupillary constriction, sedation and overall “drug effect” and in patients, analgesia and feelings of “relaxation.” In non-tolerant patients, analgesia is not usually seen at a plasma oxycodone concentration of less than 5 to 10 ng/mL.
As with all opioids, the minimum effective plasma concentration for analgesia will vary widely among patients, especially among patients who have been previously treated with potent agonist opioids. As a result, patients need to be treated with individualized titration of dosage to the desired effect. The minimum effective analgesic concentration of oxycodone for any individual patient may increase with repeated dosing due to an increase in pain and/or the development of tolerance.
Concentration—Adverse Experience Relationships
Oxycodone hydrochloride capsules are associated with typical opioid-related adverse experiences similar to those seen with all opioids. There is a general relationship between increasing oxycodone plasma concentration and increasing frequency of dose-related opioid adverse experiences such as nausea, vomiting, CNS effects and respiratory depression. In opioid-tolerant patients, the situation is altered by the development of tolerance to opioid-related side effects, and the relationship is poorly understood.
As with all opioids, the dose must be individualized (see DOSAGE AND ADMINISTRATION), because the effective analgesic dose for some patients will be too high to be tolerated by other patients.
CONTRAINDICATIONS
Oxycodone hydrochloride capsules are contraindicated in patients with known hypersensitivity to oxycodone, or in any situation where opioids are contraindicated. This includes patients with significant respiratory depression (in unmonitored settings or the absence of resuscitative equipment), and patients with acute or severe bronchial asthma or hypercarbia. Oxycodone hydrochloride capsules are contraindicated in any patient who has or is suspected of having paralytic ileus.
WARNINGS
Respiratory Depression
Respiratory depression is the chief hazard from all opioid agonist preparations. Respiratory depression occurs most frequently in elderly or debilitated patients, usually following large initial doses in non-tolerant patients, or when opioids are given in conjunction with other agents that depress respiration.
Oxycodone should be used with extreme caution in patients with significant chronic obstructive pulmonary disease or cor pulmonale, and in patients having a substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression. In such patients, even usual therapeutic doses of oxycodone may decrease respiratory drive to the point of apnea. In these patients alternative non-opioid analgesics should be considered, and opioids should be employed only under careful medical supervision at the lowest effective dose.
Hypotensive Effect
Oxycodone hydrochloride capsules, like all opioid analgesics, may cause severe hypotension in an individual whose ability to maintain blood pressure has been compromised by a depleted blood volume, or after concurrent administration with drugs such as phenothiazines or other agents which compromise vasomotor tone. Oxycodone hydrochloride capsules may produce orthostatic hypotension in ambulatory patients. Oxycodone hydrochloride capsules, like all opioid analgesics, should be administered with caution to patients in circulatory shock, since vasodilation produced by the drug may further reduce cardiac output and blood pressure.
Drug Dependence
Oxycodone can produce drug dependence of the morphine type, and therefore, has the potential for being abused. Psychic dependence, physical dependence and tolerance may develop upon repeated administration of this drug, and it should be prescribed and administered with the same degree of caution appropriate to the use of other oral narcotic containing medications. Like other narcotic containing medications, this drug is subject to the Federal Controlled Substances Act.
Usage in Ambulatory Patients
Oxycodone may impair the mental and/or physical abilities required for the performance of potentially hazardous tasks such as driving a car or operating machinery. The patient using this drug should be cautioned accordingly.
Interaction with Other Central Nervous System Depressants
Patients receiving other narcotic analgesics, general anesthetics, phenothiazines, other tranquilizers, sedative-hypnotics or other CNS depressants (including alcohol) concomitantly with oxycodone hydrochloride may exhibit an additive CNS depression. When such combined therapy is contemplated, the dose of one or both agents should be reduced.
PRECAUTIONS
General
Opioid analgesics given on a fixed-dosage schedule have a narrow therapeutic index in certain patient populations, especially when combined with other drugs, and should be reserved for cases where the benefits of opioid analgesia outweigh the known risks of respiratory depression, altered mental state, and postural hypotension.
Use of oxycodone hydrochloride capsules is associated with increased potential risks and should be used only with caution in the following conditions: acute alcoholism; adrenocortical insufficiency (e.g., Addison’s disease); CNS depression or coma; delirium tremens; debilitated patients; kyphoscoliosis associated with respiratory depression; myxedema or hypothyroidism; prostatic hypertrophy or urethral stricture; severe impairment of hepatic, pulmonary or renal function; and toxic psychosis.
The administration of oxycodone, like all opioid analgesics, may obscure the diagnosis or clinical course in patients with acute abdominal conditions. Oxycodone may aggravate convulsions in patients with convulsive disorders, and all opioids may induce or aggravate seizures in some clinical settings.
Interactions with Mixed Agonist/Antagonist Opioid Analgesics
Agonist/antagonist and partial agonist analgesics (i.e., pentazocine, nalbuphine, butorphanol and buprenorphine) should be administered with caution to a patient who has received or is receiving a course of therapy with a pure opioid agonist analgesic such as oxycodone. In this situation, mixed agonist/antagonist and partial agonist analgesics may reduce the analgesic effect of oxycodone and/or may precipitate withdrawal symptoms in these patients.
Use in Pancreatic/Biliary Tract Disease
Oxycodone may cause spasm of the sphincter of Oddi and should be used with caution in patients with biliary tract disease, including acute pancreatitis. Opioids like oxycodone may cause increases in the serum amylase level.
Head Injury and Increased Intracranial Pressure
The respiratory depressant effects of opioids and their capacity to elevate cerebrospinal fluid pressure may be markedly exaggerated in the presence of head injury, other intracranial lesions or a pre-existing increase in intracranial pressure. Furthermore, opioids produce adverse reactions which may obscure the clinical course of patients with head injuries.
Acute Abdominal Conditions
The administration of this drug or other opioids may obscure the diagnosis or clinical course in patients with acute abdominal conditions.
Information for Patients/Caregivers
If clinically advisable, patients receiving oxycodone hydrochloride capsules or their caregivers should be given the following information by the physician, nurse, pharmacist or caregiver:
- Patients should be advised not to adjust the dose of this drug without consulting the prescribing professional.
- Patients should be advised that this drug may impair mental and/or physical ability required for the performance of potentially hazardous tasks (e.g., driving, operating heavy machinery).
- Patients should not combine this drug with alcohol or other central nervous system depressants (sleep aids, tranquilizers) except by the orders of the prescribing physician, because additive effects may occur.
- Women of childbearing potential who become, or are planning to become, pregnant should be advised to consult their physician regarding the effects of analgesics and other drug use during pregnancy on themselves and their unborn child.
- Patients should be advised that this drug is a potential drug of abuse. They should protect it from theft, and it should never be given to anyone other than the individual for whom it was prescribed.
- Patients should be advised that if they have been receiving treatment with this drug for more than a few weeks and cessation of therapy is indicated, it may be appropriate to taper this drug dose, rather than abruptly discontinue it, due to the risk of precipitating withdrawal symptoms. Their physician can provide a dose schedule to accomplish a gradual discontinuation of the medication.
Laboratory Monitoring
Due to the broad range of plasma concentrations seen in clinical populations, the varying degrees of pain, and the development of tolerance, plasma oxycodone measurements are usually not helpful in clinical management. Plasma concentrations of the active drug substance may be of value in selected, unusual or complex cases.
Use in Drug and Alcohol Addiction
Oxycodone hydrochloride capsules are opioids with no approved use in the management of addictive disorders. Their proper usage in individuals with drug or alcohol dependence, either active or in remission, is for the management of pain requiring opioid analgesia.
Drug-Drug Interactions
The CNS depressant effects of oxycodone hydrochloride may be additive with that of other CNS depressants (see WARNINGS).
Opioid analgesics, including oxycodone hydrochloride capsules, may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression.
Oxycodone is metabolized in part to oxymorphone via CYP2D6. While this pathway may be blocked by a variety of drugs (e.g., certain cardiovascular drugs and antidepressants), such blockade has not yet been shown to be of clinical significance with this agent. Clinicians should be aware of this possible interaction, however.
Mutagenicity/Carcinogenicity
Oxycodone was not mutagenic in the following assays: Ames Salmonella and E. Coli test with and without metabolic activation at doses of up to 5000 mcg, chromosomal aberration test in human lymphocytes in the absence of metabolic activation at doses of up to 1500 mcg/mL and with activation 48 hours after exposure at doses of up to 5000 mcg/mL, and in the in vivo bone marrow micronucleus test in mice (at plasma levels of up to 48 mcg/mL). Mutagenic results occurred in the presence of metabolic activation in the human chromosomal aberration test (at greater than or equal to 1250 mcg/mL) at 24 but not 48 hours of exposure and in the mouse lymphoma assay at doses of 50 mcg/mL or greater with metabolic activation and at 400 mcg/mL or greater without metabolic activation. The data from these tests indicate that the genotoxic risk to humans may be considered low.
Studies of oxycodone in animals to evaluate its carcinogenic potential have not been conducted owing to the length of clinical experience with the drug substance.
Labor and Delivery
Oxycodone hydrochloride capsules are not recommended for use in women during and immediately prior to labor and delivery because oral opioids may cause respiratory depression in the newborn.
Nursing Mothers
Low concentrations of oxycodone have been detected in breast milk. Withdrawal symptoms can occur in breast-feeding infants when maternal administration of an opioid analgesic is stopped. Ordinarily, nursing should not be undertaken while a patient is receiving oxycodone hydrochloride capsules since oxycodone may be excreted in the milk.
ADVERSE REACTIONS
The most frequently observed reactions include light-headedness, dizziness, sedation, nausea and vomiting. These effects seem to be more prominent in ambulatory than in nonambulatory patients, and some of these adverse reactions may be alleviated if the patient lies down. Many of these adverse events will cease or decrease in intensity as oxycodone therapy is continued and some degree of tolerance is developed.
Other adverse reactions include euphoria, dysphoria, constipation, skin rash and pruritus.
DRUG ABUSE AND DEPENDENCE (Addiction)
Oxycodone products are common targets for both drug abusers and drug addicts.
Drug addiction (drug dependence, psychological dependence) is characterized by a preoccupation with the procurement, hoarding, and abuse of drugs for non-medicinal purposes. Drug dependence is treatable, utilizing a multi-disciplinary approach, but relapse is common. “Drug seeking” behavior is very common to addicts. Tolerance and physical dependence in pain patients are not signs of psychological dependence. Preoccupation with achieving adequate pain relief can be appropriate behavior in a patient with poor pain control. Most chronic pain patients limit their intake of opioids to achieve a balance between the benefits of the drug and dose-limiting side effects. Physicians should be aware that psychological dependence may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true psychological dependence and is characterized by misuse for non-medical purposes, often in combination with other psychoactive substances.
MANAGEMENT OF OVERDOSAGE
Signs and Symptoms
Serious overdose of oxycodone hydrochloride is characterized by respiratory depression (a decrease in respiratory rate and/or tidal volume, Cheyne-Stokes respiration, cyanosis), extreme somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, and sometimes bradycardia and hypotension. In severe overdosage, apnea, circulatory collapse, cardiac arrest and death may occur.
Treatment
Primary attention should be given to the re-establishment of adequate respiratory exchange through provision of a patent airway and the institution of assisted or controlled ventilation. The narcotic antagonist naloxone is a specific antidote against respiratory depression which may result from overdosage or unusual sensitivity to narcotics, including oxycodone. Therefore, an appropriate dose of naloxone (usual initial adult dose: 0.4 mg) should be administered, preferably by the intravenous route, simultaneously with efforts at respiratory resuscitation. Since the duration of action of oxycodone may exceed that of the antagonist, the patient should be kept under continued surveillance and repeated doses of the antagonist should be administered as needed to maintain adequate respiration. An antagonist should not be administered in the absence of clinically significant respiratory or cardiovascular depression.
Oxygen, intravenous fluids, vasopressors and other supportive measures should be employed as indicated.
Gastric emptying may be useful in removing unabsorbed drug.
DOSAGE AND ADMINISTRATION
Dosage should be adjusted to the severity of the pain and the response of the patient. It may occasionally be necessary to exceed the usual dosage recommended below in cases of more severe pain or in those patients who have become tolerant to the analgesic effects of opioids. This drug is given orally. The usual adult dosage is 5 mg every 6 hours as needed for pain.
HOW SUPPLIED
Oxycodone Hydrochloride Immediate-Release Oral Capsules, 5 mg are available as opaque brown cap, imprinted “0554”, and opaque light brown body imprinted 
- Bottles of 100.......................................NDC 0406-0554-01
Dispense in a tight, light-resistant container with a child-resistant closure.
Protect from moisture. Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.

COVIDIEN™
Mallinckrodt
Mallinckrodt Inc.,
Hazelwood, MO 63042 USA.
Rev 020409
PACKAGE LABEL - PRINCIPAL DISPLAY PANEL - 5 mg Bottle
NDC 0406-0554-01
100 CAPSULES
OXYCODONE HYDROCHLORIDE
IMMEDIATE-RELEASE CAPSULES
CII
5 mg
Each capsule contains:
Oxycodone Hydrochloride USP . . . . . . . 5 mg
Rx only
Mallinckrodt
| OXYCODONE HYDROCHLORIDE
IMMEDIATE-RELEASE
oxycodone hydrochloride capsule |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| UNAPPROVED DRUG OTHER | 06/18/2009 | 07/31/2012 | |
| Labeler - Mallinckrodt, Inc. (047021092) |
| Establishment | |||
| Name | Address | ID/FEI | Operations |
| MALLINCKRODT INC | 957414238 | ANALYSIS, MANUFACTURE | |
Revised: 07/2012 Mallinckrodt, Inc.