M.V.I. PEDIATRIC- ascorbic acid, retinol, ergocalciferol, thiamine hydrochloride, riboflavin 5-phosphate sodium, pyridoxine hydrochloride, niacinamide, dexpanthenol, .alpha.-tocopherol acetate, dl-, biotin, folic acid, cyanocobalamin, and phytonadione injection, powder, lyophilized, for solution
Hospira, Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use M.V.I. Pediatric® safely and effectively. See full prescribing information for M.V.I. Pediatric.
M.V.I. Pediatric (multiple vitamins for injection), for intravenous use Initial U.S. Approval: 1983 RECENT MAJOR CHANGES
INDICATIONS AND USAGEM.V.I. Pediatric is a combination of vitamins indicated for the prevention of vitamin deficiency in pediatric patients up to 11 years of age receiving parenteral nutrition (1) DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHSCONTRAINDICATIONSWARNINGS AND PRECAUTIONS
ADVERSE REACTIONSAdverse reactions have included anaphylaxis, rash, erythema, pruritus, headache, dizziness, agitation, anxiety, diplopia, urticaria, shortness of breath, wheezing and angioedema (6) To report SUSPECTED ADVERSE REACTIONS, contact Hospira, Inc. at 1-800-441-4100 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. DRUG INTERACTIONSDrug Interactions Affecting Co-administered Drugs:
Drug Interactions Affecting Vitamin Levels: USE IN SPECIFIC POPULATIONSSee 17 for PATIENT COUNSELING INFORMATION. Revised: 2/2019 |
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
M.V.I. Pediatric is a combination of vitamins indicated for the prevention of vitamin deficiency in pediatric patients up to 11 years of age receiving parenteral nutrition.
The physician should not await the development of clinical signs of vitamin deficiency before initiating vitamin therapy.
2 DOSAGE AND ADMINISTRATION
2.1 Important Dosage and Administration Instructions
M.V.I. Pediatric is a combination product that contains the following vitamins: ascorbic acid, vitamin A, vitamin D, thiamine, riboflavin, pyridoxine, niacinamide, dexpanthenol, vitamin E, vitamin K, folic acid, biotin, and vitamin B12 [see Dosage and Administration (2.2)].
M.V.I. Pediatric is supplied as a single-dose vial of lyophilized powder for reconstitution and intended for administration by intravenous infusion after dilution.
Do not administer M.V.I. Pediatric as a direct, undiluted intravenous injection as it may cause dizziness, faintness and tissue irritation.
2.2 Dosage Information
- The recommended daily dosage volume of 1.5 mL, 3.25 mL, or 5 mL of the reconstituted solution is based on the patient's actual weight of less than 1 kg, 1 kg to less than 3 kg, and more than or equal to 3 kg, respectively (see Table 1).
| Less than 1 kg | 1 kg to less than 3 kg | More than or equal to 3 kg | |
|---|---|---|---|
| Daily Dosage Volume | 1.5 mL | 3.25 mL | 5 mL |
| Vitamin A* (retinol) | 690 IU† (equals approx. 0.207 mg) | 1,495 IU (equals approx. 0.449 mg) | 2,300 IU (equals approx. 0.690 mg) |
| Vitamin D‡ (ergocalciferol) | 120 IU (equals 3 mcg) | 280 IU (equals 7 mcg) | 400 IU (equals 10 mcg) |
| Vitamin E§ (dl-alpha-tocopheryl acetate) | 2.1 IU (equals 2 mg) | 4.6 IU (equals 5 mg) | 7 IU (equals 7 mg) |
| Vitamin K1 (phytonadione) | 0.1 mg | 0.1 mg | 0.2 mg |
| Vitamin B2 (as riboflavin 5-phosphate sodium) | 0.4 mg | 0.9 mg | 1.4 mg |
| Vitamin C (ascorbic acid) | 24 mg | 52 mg | 80 mg |
| Vitamin B6 (pyridoxine hydrochloride) | 0.3 mg | 0.7 mg | 1 mg |
| Niacinamide | 5.1 mg | 11.1 mg | 17 mg |
| Dexpanthenol (as d-pantothenyl alcohol) | 1.5 mg | 3.3 mg | 5 mg |
| Vitamin B1 (thiamine hydrochloride) | 0.4 mg | 0.8 mg | 1.2 mg |
| Biotin | 6 mcg | 13 mcg | 20 mcg |
| Folic acid | 42 mcg | 91 mcg | 140 mcg |
| Vitamin B12 (cyanocobalamin) | 0.3 mcg | 0.7 mcg | 1 mcg |
- One daily dose of the reconstituted solution (1.5 mL, 3.25 mL or 5 mL) is then added directly to the intravenous fluid [see Dosage and Administration (2.3)].
- Patients with multiple vitamin deficiencies or with increased vitamin requirements may need multiple daily dosages as indicated or additional doses of individual vitamins. However, additional daily dosages in infants are not recommended [see Warnings and Precautions (5.8)]. Supplemental vitamin A may be required for low-birth weight infants.
2.3 Preparation and Administration Instructions
- M.V.I Pediatric is to be reconstituted and diluted only in a suitable work area such as a laminar flow hood (or an equivalent clean air compounding area).
- Reconstitue the single-dose vial of M.V.I. Pediatric by adding 5 mL of Sterile Water for Injection USP, or Dextrose Injection USP 5%, or Sodium Chloride Injection USP to the 10 mL vial.
- Swirl the vial gently after the addition of the diluent to hasten reconstitution. The reconstituted solution is ready within three minutes for use.
- Visually inspect for particulate matter and discoloration prior to administration.
- Once reconstituted, immediately withdraw the dose to be added to the appropriate intravenous fluids [see Dosage Information (2.2)] and discard any unused portion. After reconstitution, complete withdrawal of vial contents within 4 hours. The reconstituted solution may be refrigerated and stored for up to 4 hours.
- After M.V.I. Pediatric is diluted in an intravenous infusion, refrigerate the resulting solution unless it is to be used immediately, and use the solution within 24 hours after dilution.
- Minimize exposure to light because some of the vitamins in M.V.I.Pediatric, particularly A, D and riboflavin, are light sensitive.
2.4 Monitoring Vitamin Blood Levels
Monitor blood vitamin concentrations to ensure maintenance of adequate levels, particularly in patients receiving parenteral multivitamins as the only source of vitamins for long periods of time.
2.5 Drug Incompatibilities
- M.V.I. Pediatric is not physically compatible with alkaline solutions such as a sodium bicarbonate solution and other alkaline drugs such as acetazolamide sodium, aminophylline, ampicillin sodium, tetracycline HCl and chlorothiazide sodium.
- Folic acid is unstable in the presence of calcium salts such as calcium gluconate.
- Vitamin A and thiamine in M.V.I. Pediatric may react with bisulfite solutions such as sodium bisulfite or vitamin K bisulfite.
- Do not add M.V.I. Pediatric directly to intravenous fat emulsions.
- Consult appropriate references for listings of physical and chemical compatibility of solutions and drugs with M.V.I. Pediatric. In such circumstances, admixture or Y-site administration with M.V.I. Pediatrc should be avoided.
3 DOSAGE FORMS AND STRENGTHS
M.V.I. Pediatric for injection is available as a single-dose vial of yellow to amber colored lyophilized powder for reconstitution.
See Description section for vitamin strengths [see Description (11)].
4 CONTRAINDICATIONS
M.V.I. Pediatric is contraindicated in patients who have:
- A history of known hypersensitivity to any of the vitamins or excipients in M.V.I. Pediatric [see Warnings and Precautions (5.2), Adverse Reactions (6)]
- An existing hypervitaminosis
5 WARNINGS AND PRECAUTIONS
5.1 Aluminum Toxicity
M.V.I. Pediatric contains aluminum, up to 42 mcg/L that may be toxic. Aluminum may reach toxic levels with prolonged parenteral administration in patients with renal impairment. Premature neonates are particularly at risk because their kidneys are immature, and they require large amounts of calcium and phosphate solutions, which contain aluminum.
Patients with impaired kidney function, including premature neonates, who receive parenteral levels of aluminum at greater than 4 to 5 micrograms per kg per day, accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration. To prevent aluminum toxicity, periodically monitor aluminum levels with prolonged parenteral administration of M.V.I. Pediatric.
5.2 Allergic Reactions to Thiamine
Allergic reactions such as urticaria, shortness of breath, wheezing and angioedema have been reported following intravenous administration of thiamine, an ingredient in M.V.I. Pediatric. There have been rare reports of anaphylaxis following intravenous doses of thiamine. No fatal anaphylaxis reactions associated with M.V.I. Pediatric have been reported.
5.3 Hypervitaminosis A
Hypervitaminosis A, manifested by nausea, vomiting, headache, dizziness, and blurred vision, has been reported in patients with renal failure receiving 1.5 mg per day retinol and in patients with liver disease. Therefore, supplementation of patients with renal failure and patients with liver diseases with vitamin A, an ingredient found in M.V.I. Pediatric, should be undertaken with caution [see Use in Specific Populations (8.6, 8.7)]. Blood levels of Vitamin A should be monitored periodically.
5.4 Decreased Anticoagulant Effect of Warfarin
M.V.I. Pediatric contains Vitamin K, which may decrease the anticoagulant effect of warfarin. In patients who are on warfarin anticoagulant therapy receiving M.V.I. Pediatric, prothrombin time/INR should be periodically monitored to determine if the dose of warfarin needs to be adjusted.
5.5 Interference with Diagnosis of Megaloblastic Anemia
M.V.I. Pediatric contains folic acid and cyanocobalamin, which can mask serum deficits of folic acid and cyanocobalamin in patients with megaloblastic anemia. Avoid the use of M.V.I. Pediatric in patients with suspected or diagnosed megaloblastic anemia prior to blood sampling for the detection of the folic acid and cyanocobalamin deficiencies.
5.6 Potential to Develop Vitamin Deficiencies or Excesses
In patients receiving parenteral multivitamins, such as with M.V.I. Pediatric, blood vitamin concentrations should be periodically monitored to determine if vitamin deficiencies or excesses are developing. M.V.I. Pediatric may not correct long-standing specific vitamin deficiencies. The administration of additional doses of specific vitamins may be required [see Dosage and Administration (2.2)].
5.7 Interference with Urine Glucose Testing
M.V.I. Pediatric contains Vitamin C, which is also known as ascorbic acid. Ascorbic acid in the urine may cause false negative urine glucose determinations.
5.8 Vitamin E Overdose in Infants Receiving Additional Vitamin E
Additional vitamin E supplementation of patients receiving M.V.I Pediatric may result in elevated blood concentrations of vitamin E and potential vitamin E toxicity in infants. Avoid additional oral or parenteral doses of vitamin E in infants. A daily dose of M.V.I. Pediatric contains adequate concentrations of vitamin E required to achieve normal blood levels of vitamin E.
5.9 Risk of Low Vitamin A Levels
Vitamin A may adhere to plastic, resulting in lower vitamin A concentrations after administration of M.V.I. Pediatric. Therefore, blood vitamin A concentrations should be periodically monitored and the administration of additional therapeutic doses of Vitamin A may be required, especially in low birth weight infants.
5.10 Risk of E-Ferol syndrome
E-Ferol syndrome, manifested by thrombocytopenia, renal dysfunction, hepatomegaly, cholestasis, ascites, hypotension and metabolic acidosis, has been reported in low-birth weight infants following administration of polysorbates, which are found in M.V.I. Pediatric. No E-Ferol syndrome associated with M.V.I. Pediatric has been reported.
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the label.
- Allergic Reactions to Thiamine [see Warnings and Precautions (5.2)].
- Hypervitaminosis A [see Warnings and Precautions (5.3)].
The following adverse reactions have been identified during post approval use of M.V.I. Pediatric. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Allergic: anaphylaxis, urticaria, shortness of breath, wheezing, angioedema
CNS: headache, dizziness, agitation, anxiety
Dermatologic: rash, erythema, pruritus
Ophthalmic: diplopia
7 DRUG INTERACTIONS
7.1 Effect of M.V.I. Pediatric on Other Drugs
Warfarin: Vitamin K, a component of M.V.I. Pediatric, antagonizes the anticoagulant action of warfarin. In patients who are co-administered warfarin and M.V.I. Pediatric, monitor blood levels of prothrombin/INR periodically to determine if the dose of warfarin needs to be adjusted.
Phenytoin: Folic acid may increase phenytoin metabolism and lower the serum concentration of phenytoin, resulting in increased seizure frequency.
Levodopa: Pyridoxine may increase the metabolism of levodopa (decrease blood level of levodopa) and decrease its efficacy.
7.2 Effect of Other Drugs on M.V.I. Pediatric
Hydralazine or Isoniazid: Concomitant administration of hydralazine or isoniazid may increase pyridoxine requirements.
8 USE IN SPECIFIC POPULATIONS
8.4 Pediatric Use
The safety and effectiveness of M.V.I. Pediatric for the prevention of vitamin deficiency have been established in pediatric patients up to 11 years of age receiving parenteral nutrition. The safety and effectiveness of M.V.I. Pediatric have not been established in pediatric patients older than 11 years of age.
M.V.I. Pediatric contains aluminum that may be toxic for premature neonates. Aluminum levels should be monitored periodically during administration of M.V.I. Pediatric to premature neonates [see Warnings and Precautions (5.1)].
Additional vitamin E supplementation of infants receiving M.V.I. Pediatric may result in elevated blood concentrations of vitamin E and potential vitamin E toxicity [see Warnings and Precautions (5.8)].
E-Ferol syndrome has been reported in low-birth weight infants following administration of polysorbates, which are found in M.V.I. Pediatric [see Warnings and Precautions (5.10)].
8.6 Renal Impairment
M.V.I. Pediatric has not been studied in patients with renal impairment. Monitor renal function, calcium, phosphorus and vitamin A levels in patients with renal impairment [see Warnings and Precautions (5.1, 5.3)].
8.7 Hepatic Impairment
M.V.I. Pediatric has not been studied in patients with hepatic impairment. Monitor vitamin A level in patients with liver disease [see Warnings and Precautions (5.3)].
10 OVERDOSAGE
Signs and symptoms of acute or chronic overdosage may be those of individual M.V.I. Pediatric component toxicity.
11 DESCRIPTION
M.V.I. Pediatric (multiple vitamins for injection) is a yellow to amber colored lyophilized, sterile powder for reconstitution intended for administration by intravenous infusion after dilution [see Dosage and Administration (2.3)].
Table 2 provides the strengths of the vitamins provided in each 5 mL of reconstituted product:
| Ingredient | Amount per Unit Dose |
|---|---|
| With Butylated Hydroxyanisole – 14 mcg; Butylated Hydroxytoluene – 58 mcg; Mannitol – 375 mg; Polysorbate 20 - 0.8 mg; Polysorbate 80 - 50 mg; Sodium hydroxide for pH adjustment. | |
| Fat Soluble Vitamins* | |
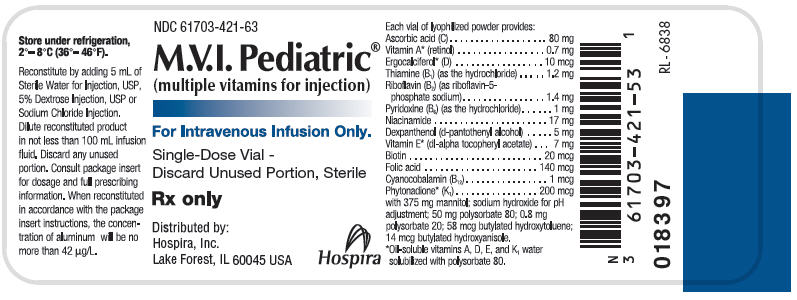
| Vitamin A†* (retinol) | 2,300 IU‡ (equals 0.7 mg) |
| Vitamin D§* (ergocalciferol) | 400 IU (equals 10 mcg) |
| Vitamin E¶* (dl-alpha-tocopheryl acetate) | 7 IU (equals 7 mg) |
| Vitamin K1* (phytonadione) | 200 mcg |
| Water Soluble Vitamins | |
| Vitamin B2 (as riboflavin 5-phosphate sodium) | 1.4 mg |
| Vitamin C (ascorbic acid) | 80 mg |
| Vitamin B6 (pyridoxine hydrochloride) | 1 mg |
| Niacinamide | 17 mg |
| Dexpanthenol (as d-pantothenyl alcohol) | 5 mg |
| Vitamin B1 (thiamine hydrochloride) | 1.2 mg |
| Biotin | 20 mcg |
| Folic acid | 140 mcg |
| Vitamin B12 (cyanocobalamin) | 1 mcg |
M.V.I. Pediatric (multiple vitamins for injection) provides a combination of oil-soluble and water-soluble vitamins, formulated for incorporation into intravenous infusions after reconstitution. The liposoluble vitamins A, D, E and K1 have been solubilized in an aqueous medium with polysorbate 80, permitting intravenous administration of these vitamins.
16 HOW SUPPLIED/STORAGE AND HANDLING
M.V.I. Pediatric for injection is supplied as a single-dose vial of lyophilized powder for reconstitution available as:
- Box of 10 single-dose glass fliptop vials (NDC 61703-421-53)
See Description section for vitamin strengths [see Description (11)].
17 PATIENT COUNSELING INFORMATION
Instruct patients (if age appropriate) and caregivers:
- To watch for and immediately report signs of allergic reactions (i.e., urticaria, shortness of breath, wheezing, and angioedema).
- To watch for and immediately report signs of hypervitaminosis A, manifested by nausea, vomiting, headache, dizziness, and blurred vision, if patients have renal impairment.
- To report other adverse reactions such as rash, erythema, pruritus, headache, dizziness, agitation, anxiety, and diplopia.
- That patients on warfarin anticoagulant therapy will be monitored periodically for blood prothrombin levels to determine the appropriate dose of warfarin.
- About the significance of periodic monitoring of blood vitamin concentrations to determine if vitamin deficiencies or excesses are developing.
- About the need to monitor renal function, calcium, phosphorus, aluminum, and vitamin A levels in patients with renal impairment.

PRINCIPAL DISPLAY PANEL - 5 mL Vial Label
NDC 61703-421-63
M.V.I. Pediatric®
(multiple vitamins for injection)
For Intravenous Infusion Only.
Single-Dose Vial -
Discard Unused Portion, Sterile
Rx only
Distributed by:
Hospira, Inc.
Lake Forest, IL 60045 USA
Hospira
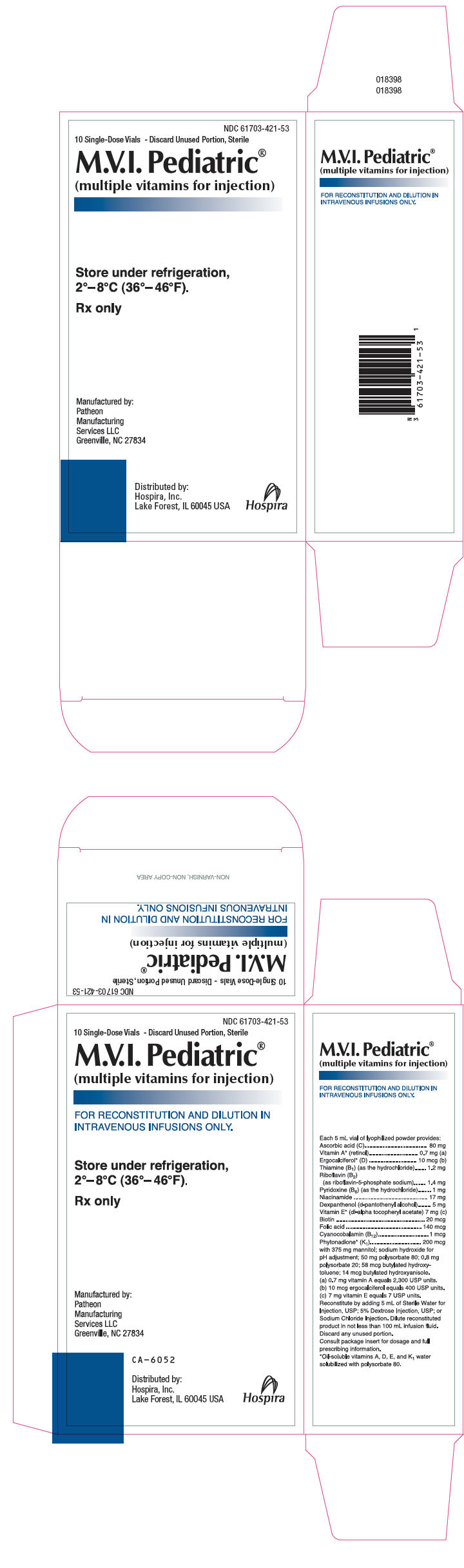
PRINCIPAL DISPLAY PANEL - 5 mL Vial Box
NDC 61703-421-53
10 Single-Dose Vials - Discard Unused Portion, Sterile
M.V.I. Pediatric®
(multiple vitamins for injection)
Store under refrigeration,
2°–8°C (36°–46°F).
Rx only
Manufactured by:
Patheon
Manufacturing
Services LLC
Greenville, NC 27834
Distributed by:
Hospira, Inc.
Lake Forest, IL 60045 USA
Hospira
| M.V.I. PEDIATRIC
ascorbic acid, retinol, ergocalciferol, thiamine hydrochloride, riboflavin 5-phosphate sodium, pyridoxine hydrochloride, niacinamide, dexpanthenol, .alpha.-tocopherol acetate, dl-, biotin, folic acid, cyanocobalamin, and phytonadione injection, powder, lyophilized, for solution |
|||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||
| Labeler - Hospira, Inc. (141588017) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Patheon Manufacturing Services LLC | 079415560 | ANALYSIS(61703-421) , LABEL(61703-421) , MANUFACTURE(61703-421) , PACK(61703-421) | |