Label: THERACODOPHEN-LOW-90- hydrocodone bitartrate, acetaminophen, .gamma.-aminobutyric acid kit



-
Contains inactivated NDC Code(s)
NDC Code(s): 52959-312-30, 68405-298-36 - Packager: Physician Therapeutics LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: unapproved drug other
DISCLAIMER: This drug has not been found by FDA to be safe and effective, and this labeling has not been approved by FDA. For further information about unapproved drugs, click here.
Drug Label Information
Updated August 1, 2011
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
PRINCIPAL DISPLAY PANEL
NDC 53746-111-05
Hydrocodone
Bitartrate and
Acetominophen
Tablets, USP
Multiple Strengths:
Do not dispense unless
strength is stated.
Rx only 500 TABLETS
Each tablet contains:
hydrocodone bitartrate 5 mg
acetaminophen 500 mg
Usual adult dosage: See package insert.
Store at 25 degrees C (77 degrees F); excursions permitted to 15 degrees - 30 degrees C
(59 - 86 degrees F). [See USP Controlled Room Temperature].
Dispense in tight, light-resistant container as defined in the USP.
Protect from light.
Do not accept if inner seal is broken or missing.
Manufactured by: Amneal Pharmaceticals of NY
Hauppauge, NY 11788
Distributed by: Amneal Pharmaceuticals
Glasgow, KY 42141
-
DESCRIPTION
Hydrocodone bitartrate and acetaminophen is supplied in tablet form for oral administration.
Hydrocodone bitartrate is an opioid analgesic and antitussive and occurs as fine, white crystals or as a crystalline powder. It is affected by light.
The chemical name is 4,5α-epoxy-3-methoxy-17-methylmorphinan-6-one tartrate (1:1) hydrate (2:5). It has the following structural formula:
- DESCRIPTION
-
DESCRIPTION
Hydrocodone Bitartrate and Acetaminophen Tablets USP for oral administration
are available in a variety of strengths as described in the following table.Strength Hydrocodone Bitartrate Acetaminophen
2.5 mg/500mg 2.5mg 500mg
5mg/500mg 5mg 500mg
7.5mg/325mg 7.5mg 325mg
7.5mg/500mg 7.5mg 500mg
7.5mg/650mg 7.5mg 650mg
7.5mg/750mg 7.5mg 750mg
10mg/325mg 10mg 325mg
10mg/500mg 10mg 500mg
10mg/650mg 10mg 650mg
10mg/660mg 10mg 660mg
10mg/750mg 10mg 750mgIn addition, each tablet contains the following inactive ingredients:
anhydrous lactose, croscarmellose sodium, crospovidone, magnesium stearate, microcrystalline cellulose, povidone, starch and stearic acid; except the 7.5 mg/325 mg, 10 mg/325 mg and 10 mg/500 mg tablets do not contain anhydrous lactose. The 7.5 mg/325 mg tablets include FD and C Yellow Number 6 Aluminum Lake; the 7.5 mg/650 mg tablets include FD and C Red Number 40 Aluminum Lake; the 10 mg/325 mg and 10 mg/750 mg tablets include D and C Yellow Number 10 Aluminum Lake; the 10 mg/500 mg include FD and C Blue Number 2 Aluminum Lake; and the 10 mg/650 mg tablets include FD and C Blue Number 1 Aluminum Lake and D and C Yellow number 10 Aluminum Lake. Meets USP Dissolution Test 1. -
CLINICAL PHARMACOLOGY
Hydrocodone is a semisynthetic narcotic analgesic and antitussive with multiple actions qualitatively similar to those of codeine. Most of these involve the central nervous system and smooth muscle. The precise mechanism of action of hydrocodone and other opiates is not known, although it is believed to relate to the existence of opiate receptors in the central nervous system. In addition to analgesia, narcotics may produce drowsiness, changes in mood and mental clouding.
The analgesic action of acetaminophen involves peripheral influences, but the specific mechanism is as yet undetermined. Antipyretic activity is mediated through hypothalamic heat regulating centers. Acetaminophen inhibits prostaglandin synthetase. Therapeutic doses of acetaminophen have negligible effects on the cardiovascular or respiratory systems; however, toxic doses may cause circulatory failure and rapid, shallow breathing.
Pharmacokinetics: The behavior of the individual components is described below.
Hydrocodone: Following a 10 mg oral dose of hydrocodone administered to five adult male subjects, the mean peak concentration was 23.6 ± 5.2 ng/mL. Maximum serum levels were achieved at 1.3 ± 0.3 hours and the half-life was determined to be 3.8 ± 0.3 hours. Hydrocodone exhibits a complex pattern of metabolism including O-demethylation, N-demethylation and 6-keto reduction to the corresponding 6-α- and 6-β-hydroxymetabolites.
See OVERDOSAGE for toxicity information.
Acetaminophen: Acetaminophen is rapidly absorbed from the gastrointestinal tract and is distributed throughout most body tissues. The plasma half-life is 1.25 to 3 hours, but may be increased by liver damage and following overdosage.
Elimination of acetaminophen is principally by liver metabolism (conjugation) and subsequent renal excretion of metabolites. Approximately 85% of an oral dose appears in the urine within 24 hours of administration, most as the glucuronide conjugate, with small amounts of other conjugates and unchanged drug.
See OVERDOSAGE for toxicity information.
- INDICATIONS & USAGE
- CONTRAINDICATIONS
-
WARNINGS
Respiratory Depression: At high doses or in sensitive patients, hydrocodone may produce dose-related respiratory depression by acting directly on the brain stem respiratory center. Hydrocodone also affects the center that controls respiratory rhythm, and may
produce irregular and periodic breathing.
Head Injury and Increased Intracranial Pressure: The respiratory depressant effects of narcotics and their capacity to elevate cerebrospinal fluid pressure may be markedly exaggerated in the presence of head injury, other intracranial lesions or a pre-existing increase in intracranial pressure. Furthermore, narcotics produce adverse reactions which may obscure the clinical course of patients with head injuries.
Acute Abdominal Conditions: The administration of narcotics may obscure the diagnosis or clinical course of patients with acute abdominal conditions.
-
PRECAUTIONS
General:
Special Risk Patients: As with any narcotic analgesic agent, hydrocodone bitartrate and acetaminophen tablets should be used with caution in elderly or debilitated patients, and those with severe impairment of hepatic or renal function, hypothyroidism, Addison’s disease, prostatic hypertrophy or urethral stricture. The usual precautions should be observed and the possibility of respiratory depression should be kept in mind.
Cough Reflex: Hydrocodone suppresses the cough reflex; as with all narcotics, caution should be exercised when hydrocodone bitartrate and acetaminophen tablets are used postoperatively and in patients with pulmonary disease.
Information for Patients: Hydrocodone, like all narcotics, may impair mental and/or physical abilities required for the performance of potentially hazardous tasks such as driving a car or operating machinery; patients should be cautioned accordingly.
Alcohol and other CNS depressants may produce an additive CNS depression, when taken with this combination product, and should be avoided.
Hydrocodone may be habit-forming. Patients should take the drug only for as long as it is prescribed, in the amounts prescribed, and no more frequently than prescribed.
Laboratory Tests: In patients with severe hepatic or renal disease, effects of therapy should be monitored with serial liver and/or renal function tests.
Drug Interactions: Patients receiving narcotics, antihistamines, antipsychotics, antianxiety agents, or other CNS depressants (including alcohol) concomitantly with hydrocodone bitartrate and acetaminophen tablets may exhibit an additive CNS
depression. When combined therapy is contemplated, the dose of one or both agents should be reduced.
The use of MAO inhibitors or tricyclic antidepressants with hydrocodone preparations may increase the effect of either the antidepressant or hydrocodone.
Drug/Laboratory Test Interactions: Acetaminophen may produce false-positive test results for urinary 5-hydroxyindoleacetic acid.
Carcinogenesis, Mutagenesis, Impairment of Fertility: No adequate studies have been conducted in animals to determine whether hydrocodone or acetaminophen have a potential for carcinogenesis, mutagenesis, or impairment of fertility.
Pregnancy: Teratogenic Effects: Pregnancy Category C: There are no adequate and well-controlled studies in pregnant women. Hydrocodone bitartrate and acetaminophen tablets should be used during pregnancy only if the potential benefit justifies the potential
risk to the fetus.
Nonteratogenic Effects: Babies born to mothers who have been taking opioids regularly prior to delivery will be physically dependent. The withdrawal signs include irritability and excessive crying, tremors, hyperactive reflexes, increased respiratory rate, increased
stools, sneezing, yawning, vomiting and fever. The intensity of the syndrome does not always correlate with the duration of maternal opioid use or dose. There is no consensus on the best method of managing withdrawal.
Labor and Delivery: As with all narcotics, administration of this product to the mother shortly before delivery may result in some degree of respiratory depression in the newborn, especially if higher doses are used.
Nursing Mothers: Acetaminophen is excreted in breast milk in small amounts, but the significance of its effects on nursing infants is not known. It is not known whether hydrocodone is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from hydrocodone, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use: Safety and effectiveness in pediatric patients have not been established.
Geriatric Use: Clinical studies of hydrocodone bitartrate 5 mg and acetaminophen 500 mg did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Hydrocodone and the major metabolites of acetaminophen are known to be substantially excreted by the kidney. Thus the risk of toxic reactions may be greater in patients with impaired renal function due to the accumulation of the parent compound and/or metabolites in the plasma. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Hydrocodone may cause confusion and over-sedation in the elderly; elderly patients generally should be started on low doses of hydrocodone bitartrate and acetaminophen tablets and observed closely. -
ADVERSE REACTIONS
The most frequently reported adverse reactions are lightheadedness, dizziness, sedation, nausea and vomiting. These effects seem to be more prominent in ambulatory than in nonambulatory patients, and some of these adverse reactions may be alleviated if the
patient lies down.
Other adverse reactions include:
Central Nervous System: Drowsiness, mental clouding, lethargy, impairment of mental and physical performance, anxiety, fear, dysphoria, psychic dependence, mood changes.
Gastrointestinal System: Prolonged administration of hydrocodone bitartrate and acetaminophen tablets may produce constipation.
Genitourinary System: Ureteral spasm, spasm of vesical sphincters and urinary retention have been reported with opiates.
Respiratory Depression: Hydrocodone bitartrate may produce dose-related respiratory depression by acting directly on brain stem respiratory centers (see OVERDOSAGE).
Special Senses: Cases of hearing impairment or permanent loss have been reported predominantly in patients with chronic overdose.
Dermatological: Skin rash, pruritus.
The following adverse drug events may be borne in mind as potential effects of acetaminophen: allergic reactions, rash, thrombocytopenia, agranulocytosis.
Potential effects of high dosage are listed in the OVERDOSAGE section.
-
DRUG ABUSE AND DEPENDENCE
Controlled Substance: Hydrocodone Bitartrate and Acetaminophen Tablets are classified as a Schedule III controlled substance.
Abuse and Dependence: Psychic dependence, physical dependence, and tolerance may develop upon repeated administration of narcotics; therefore, this product should be prescribed and administered with caution. However, psychic dependence is unlikely
to develop when hydrocodone bitartrate and acetaminophen tablets are used for a short time for the treatment of pain.
Physical dependence, the condition in which continued administration of the drug is required to prevent the appearance of a withdrawal syndrome, assumes clinically significant proportions only after several weeks of continued narcotic use, although some mild degree of physical dependence may develop after a few days of narcotic therapy. Tolerance, in which increasingly large doses are required in order to produce the same degree of analgesia, is manifested initially by a shortened duration of analgesic effect, and subsequently by decreases in the intensity of analgesia. The rate of development of tolerance varies among patients.
-
OVERDOSAGE
Following an acute overdosage, toxicity may result from hydrocodone or acetaminophen.
Signs and Symptoms
Hydrocodone: Serious overdose with hydrocodone is characterized by respiratory depression (a decrease in respiratory rate and/or tidal volume, Cheyne-Stokes respiration, cyanosis), extreme somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, and sometimes bradycardia and hypotension. In severe overdosage, apnea, circulatory collapse, cardiac arrest and death may occur.
Acetaminophen: In acetaminophen overdosage: dose-dependent, potentially fatal hepatic necrosis is the most serious adverse effect. Renal tubular necrosis, hypoglycemic coma and thrombocytopenia may also occur.
Early symptoms following a potentially hepatotoxic overdose may include: nausea, vomiting, diaphoresis and general malaise. Clinical and laboratory evidence of hepatic toxicity may not be apparent until 48 to 72 hours post-ingestion.
In adults, hepatic toxicity has rarely been reported with acute overdoses of less than 10 grams, or fatalities with less than 15 grams.
Treatment: A single or multiple overdose with hydrocodone and acetaminophen is a potentially lethal polydrug overdose, and consultation with a regional poison control center is recommended.
Immediate treatment includes support of cardiorespiratory function and measures to reduce drug absorption. Vomiting should be induced mechanically, or with syrup of ipecac, if the patient is alert (adequate pharyngeal and laryngeal reflexes). Oral activated charcoal (1 g/kg) should follow gastric emptying. The first dose should be accompanied by an appropriate cathartic. If repeated doses are used, the cathartic might be included with alternate doses as required. Hypotension is usually hypovolemic and should respond to fluids. Vasopressors and other supportive measures should be employed as indicated. A cuffed endotracheal tube should be inserted before gastric lavage of the unconscious patient and, when necessary, to provide assisted respiration.
Meticulous attention should be given to maintaining adequate pulmonary ventilation. In severe cases of intoxication, peritoneal dialysis, or preferably hemodialysis may be considered. If hypoprothrombinemia occurs due to acetaminophen overdose, vitamin K
should be administered intravenously.
Naloxone, a narcotic antagonist, can reverse respiratory depression and coma associated with opioid overdose. Naloxone hydrochloride 0.4 mg to 2 mg is given parenterally. Since the duration of action of hydrocodone may exceed that of the naloxone, the patient should
be kept under continuous surveillance and repeated doses of the antagonist should be administered as needed to maintain adequate respiration. A narcotic antagonist should not be administered in the absence of clinically significant respiratory or cardiovascular depression.
If the dose of acetaminophen may have exceeded 140 mg/kg, acetylcysteine should be administered as early as possible. Serum acetaminophen levels should be obtained, since levels four or more hours following ingestion help predict acetaminophen toxicity. Do not await acetaminophen assay results before initiating treatment. Hepatic enzymes should be obtained initially, and repeated at 24-hour intervals.
Methemoglobinemia over 30% should be treated with methylene blue by slow intravenous administration.
The toxic dose for adults for acetaminophen is 10 g. -
DOSAGE & ADMINISTRATION
Dosage should be adjusted according to the severity of the pain and the response of the patient. However, it should be kept in mind that tolerance to hydrocodone can develop with continued use and that the incidence of untoward effects is dose related.
2.5 mg/500 mg
5 mg/500 mgThe usual adult dosage is one or two tablets every four to six
hours as needed for pain. The total daily dose should not
exceed 8 tablets.7.5 mg/325 mg
7.5 mg/500 mg
7.5 mg/650 mg
The usual adult dosage is one tablet every four to six hours
as needed for pain. The total daily dose should not exceed
6 tablets.7.5 mg/750 mg The usual adult dosage is one tablet every four to six hours
as needed for pain. The total daily dose should not exceed
5 tablets.10 mg/325 mg
10 mg/500 mg
10 mg/650 mg
10 mg/660 mg
The usual adult dosage is one tablet every four to six hours
as needed for pain. The total daily dose should not exceed
6 tablets.10 mg/750 mg The usual adult dosage is one tablet every four to six hours
as needed for pain. The total daily dose should not exceed
5 tablets.
-
HOW SUPPLIED
Hydrocodone Bitartrate and Acetominophen Tablets USP are available in the following strengths:
2.5 mg/500 mg 2.5 mg hydrocodone bitartrate and 500 mg acetaminophen, oblong, white tablets bisected on one side and debossed with WATSON 388on the other side, supplied in bottles of 100.
5 mg/500 mg 5 mg hydrocodone bitartrate and 500 mg acetaminophen, capsule-shaped, white tablets bisected on one side and debossed with WATSON 349 on the other side, supplied in bottles of 100 and 500.
7.5 mg/325 mg 7.5 mg hydrocodone bitartrate and 325 mg acetaminophen, capsule-shaped, light orange tablets bisected on one side and debossed with WATSON 3203 on the other side, supplied in bottles of 100.
7.5 mg/500 mg 7.5 mg hydrocodone bitartrate and 500 mg acetaminophen, capsule-shaped, white tablets bisected on one side and debossed with WATSON 385on the other side, supplied in bottles of 100 and 500.
7.5 mg/650 mg 7.5 mg hydrocodone bitartrate and 650 mg acetaminophen,capsule-shaped, pink tablets bisected on one side and debossed with WATSON 502 on the other side, supplied in bottles of 100 and 500.
7.5 mg/750 mg 7.5 mg hydrocodone bitartrate and 750 mg acetaminophen, capsule-shaped, white tablets bisected on one side and debossed with WATSON 387 on the other side, supplied in bottles of 100 and 500.
10 mg/325 mg 10 mg hydrocodone bitartrate and 325 mg acetaminophen,capsule-shaped, yellow tablets bisected on one side and debossed with WATSON 853 on the other side, supplied in bottles of 100 and 500.
10 mg/500 mg 10 mg hydrocodone bitartrate and 500 mg acetaminophen, capsule-shaped, blue tablets bisected on one side and debossed with WATSON 540 on the other side, supplied in bottles of 100 and 500.
10 mg/650 mg 10 mg hydrocodone bitartrate and 650 mg acetaminophen,capsule-shaped, light green tablets bisected on one side and debossed with WATSON 503 on the other side, supplied in bottles of 100 and 500.
10 mg/660 mg 10 mg hydrocodone bitartrate and 660 mg acetaminophen,oval-shaped, white tablets bisected on one sideand debossed with WATSON 517 on the other side,supplied in bottles of 100 and 500.
10 mg/750 mg 10 mg hydrocodone bitartrate and 750 mg acetaminophen, capsule-shaped, yellow tablets bisected on one side and debossed with WATSON 3228 on the other side, supplied in bottles of 100.
Store at 20 degrees - 25 degrees C (68 degrees - 77 degrees F). [See USP controlled room temperature.]
Dispense in a tight, light-resistant container with a child-resistant closure.
Watson Laboratories, Inc. Revised: March 2007
Corona, CA 92880 USA 0907B
14715
- SPL UNCLASSIFIED SECTION
-
SPL UNCLASSIFIED SECTION
Theramine (U.S. patent pending) capsules by oral administration. A specially formulated Medical Food product, consisting of a proprietary blend of amino acids and polyphenol ingredients in specific proportions, for the dietary management of the metabolic processes associated with pain disorders and inflammatory conditions. (PD) (IC).
Must be administered under physician supervision.
-
SPL UNCLASSIFIED SECTION
Medical Foods
Medical Food products are often used in hospitals (e.g., for burn victims or kidney dialysis patients) and outside of a hospital setting under a physician’s care for the dietary management of diseases in patients with particular medical or metabolic needs due to their disease or condition. Congress defined "Medical Food" in the Orphan Drug Act and Amendments of 1988 as "a food which is formulated to be consumed or administered enterally [or orally] under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation." Medical Foods are complex formulated products, requiring sophisticated and exacting technology. Theramine has been developed, manufactured, and labeled in accordance with both the statutory and the FDA regulatory definition of a Medical Food. Theramine must be used while the patient is under the ongoing care of a physician. -
SPL UNCLASSIFIED SECTION
PAIN DISORDERS (PD) INFLAMMATORY CONDITIONS (IC)
PD and IC as a Metabolic Deficiency Disease
A critical component of the definition of a Medical Food is the requirement for a distinctive nutritional deficiency. FDA scientists have proposed a physiologic definition of a distinctive nutritional deficiency as follows: “the dietary management of patients with specific diseases requires, in some instances, the ability to meet nutritional requirements that differ substantially from the needs of healthy persons. For example, in establishing the recommended dietary allowances for general, healthy population, the Food and Nutrition Board of the Institute of Medicine National Academy of Sciences, recognized that different or distinctive physiologic requirements may exist for certain persons with "special nutritional needs arising from metabolic disorders, chronic diseases, injuries, premature birth, other medical conditions and drug therapies. Thus, the distinctive nutritional needs associated with a disease reflects the total amount needed by a healthy person to support life or maintain homeostasis, adjusted for the distinctive changes in the nutritional needs of the patient as a result of the effects of the disease process on absorption, metabolism and excretion.” It was also proposed that in patients with certain disease states who respond to nutritional therapies, a physiologic deficiency of the nutrient is assumed to exist. For example, if a patient with pain disorders responds to a tryptophan formulation by decreasing perceived pain, a deficiency of tryptophan is assumed to exist.Patients with pain disorders and inflammatory conditions are known to have nutritional deficiencies of tryptophan, choline, arginine, GABA, flavonoids, and certain antioxidants. Patients with pain disorders and inflammatory conditions frequently exhibit reduced plasma levels of tryptophan and GABA and have been shown to respond to oral administration of GABA, arginine, tryptophan, or a 5-hydoxytryptophan formulation. Research has shown that tryptophan, arginine or GABA reduced diets result in a fall of circulating tryptophan, arginine, and/or GABA. Patients with pain disorders frequently exhibit activation of the degradation pathways that increases the turnover of GABA, arginine and/or tryptophan leading to a reduced level of production of serotonin, GABA or nitric oxide for a given precursor blood level. Research has also shown that a genetic predisposition to accelerated degradation can lead to increased precursor requirements in certain patients with pain disorders and inflammatory conditions.
Choline is required to fully potentiate acetylcholine synthesis by brain neurons. A deficiency of choline leads to reduced acetylcholine production by the neurons. Flavonoids potentiate the production of acetylcholine by the neurons thereby reducing delta pain. Diets deficient in flavonoid rich foods and choline result in inadequate flavonoid concentrations, impeding acetylcholine production in certain patients with pain disorders and/or inflammatory conditions. Acetylcholine in pre-synaptic ganglia is necessary for the production of serotonin and nitric oxide in post-synaptic ganglia. Provision of tryptophan, arginine, GABA, choline and flavonoids with antioxidants, in specific proportions can restore the production of beneficial serotonin, nitric oxide, and acetylcholine, thereby reducing the perception of pain and reducing inflammation. L-Histidine is known to produce brain histamine that stimulates production of ACTH.
-
DESCRIPTION
PRODUCT DESCRIPTION
Primary Ingredients
Theramine consists of a proprietary blend of amino acids, cocoa, caffeine, cinnamon, and flavonoids in specific proportions. These ingredients fall into the category of Generally Regarded as Safe” (GRAS) as defined by the Food and Drug Administration (FDA) (Sections 201(s) and 409 of the Federal Food, Drug, and Cosmetic Act). A GRAS substance is distinguished from a food additive on the basis of the common knowledge about the safety of the substance for its intended use. The standard for an ingredient to achieve GRAS status requires not only technical demonstration of non-toxicity and safety, but also general recognition of safety through widespread usage and agreement of that safety by experts in the field. Many ingredients have been determined by the U.S. Food and Drug Administration (FDA) to be GRAS, and are listed as such by regulation, in Volume 21 Code of Federal Regulations (CFR) Sections 182, 184, and 186.Amino Acids
Amino Acids are the building blocks of protein. All amino acids are GRAS listed as they have been ingested by humans for thousands of years. The doses of the amino acids in Theramine are equivalent to those found in the usual human diet. Patients with pain disorders may require an increased amount of certain amino acids that cannot be obtained from normal diet alone. Tryptophan, for example, is an obligatory amino acid. The body cannot make tryptophan and must obtain tryptophan from the diet. Tryptophan is needed to produce serotonin. Serotonin is required to reduce pain. Patients with pain disorders and inflammatory conditions have altered serotonin metabolism. Some patients with pain disorders and inflammatory conditions have a resistance to the use of tryptophan that is similar to the mechanism found in insulin resistance. Patients with pain disorders and inflammatory conditions cannot acquire sufficient tryptophan from the diet to alter the perception of pain and the inflammatory process without ingesting a prohibitively large amount of calories, particularly calories from protein.Flavonoids
Flavonoids are a group of phytochemical compounds found in all vascular plants including fruits and vegetables. They are a part of a larger class of compounds known as polyphenols. Many of the therapeutic or health benefits of colored fruits and vegetables, cocoa, red wine, and green tea are directly related to their flavonoid content. The specially formulated flavonoids found in Theramine cannot be obtained from conventional foods in the necessary proportions to elicit a therapeutic response.Other Ingredients
Theramine contains the following inactive or other ingredients, as fillers, excipients, and colorings: magnesium stearate, microcrystalline cellulose, Maltodextrin NF, gelatin (as the capsule material).
Physical Description
Theramine is a yellow to light brown powder. Theramine contains L-Glutamine, L-Arginine, L-Histidine, and L-Serine, 5-Hydroxytryptophan as Griffonia Seed Extract, GABA, Choline Bitartrate, Cinnamon, Cocoa, Hydrolyzed Whey Protein, and Grape Seed Extract. -
CLINICAL PHARMACOLOGY
CLINICAL PHARMACOLOGY
Mechanism of Action
Theramine acts by restoring and maintaining the balance of the neurotransmitters; GABA, nitric oxide, serotonin, and acetylcholine that are associated with pain disorders and inflammatory conditions. Theramine stimulates the production ACTH to reduce inflammation.Metabolism
The amino acids in Theramine are primarily absorbed by the stomach and small intestines. All cells metabolize the amino acids in Theramine. Circulating tryptophan, arginine and choline blood levels determine the production of serotonin, nitric oxide, and acetylcholine.Excretion
Theramine is not an inhibitor of cytochrome P450 1A2, 2C9, 2C19, 2D6, or 3A4. These isoenzymes are principally responsible for 95% of all detoxification of drugs, with CYP3A4 being responsible for detoxification of roughly 50% of drugs. Amino acids do not appear to have an effect on drug metabolizing enzymes. - INDICATIONS & USAGE
-
CLINICAL STUDIES
CLINICAL EXPERIENCE
Administration of Theramine has demonstrated significant reduction in symptoms of pain and inflammation in patients with acute and chronic pain when used for the dietary management of the metabolic processes associated with pain disorders and inflammatory conditions. Administration of Theramine results in the induction and maintenance of pain relief in patients with pain disorders and inflammatory conditions. - PRECAUTIONS
-
ADVERSE REACTIONS
ADVERSE REACTIONS
Oral supplementation with L-tryptophan, L-arginine or choline at high doses up to 15 grams daily is generally well tolerated. The most common adverse reactions of higher doses — from 15 to 30 grams daily — are nausea, abdominal cramps, and diarrhea. Some patients may experience these symptoms at lower doses. The total combined amount of amino acids in each Theramine capsule does not exceed 400 mg. - DRUG INTERACTIONS
- OVERDOSAGE
-
SPL UNCLASSIFIED SECTION
POST-MARKETING SURVEILLANCE
Post-marketing surveillance has shown no serious adverse reactions. Reported cases of mild rash and itching may have been associated with allergies to Theramine flavonoid ingredients, including cinnamon, cocoa, and chocolate. These reactions were transient in nature and subsided within 24 hours. -
DOSAGE & ADMINISTRATION
DOSAGE AND ADMINISTRATION
Recommended Administration
For the dietary management of the metabolic processes associated with pain disorders and inflammatory conditions. Take (2) capsules one to three times daily or as directed by physician. As with most amino acid formulations Theramine should be taken without food to increase the absorption of key ingredients. - HOW SUPPLIED
- SPL UNCLASSIFIED SECTION
- STORAGE AND HANDLING
- SPL UNCLASSIFIED SECTION
-
SPL UNCLASSIFIED SECTION
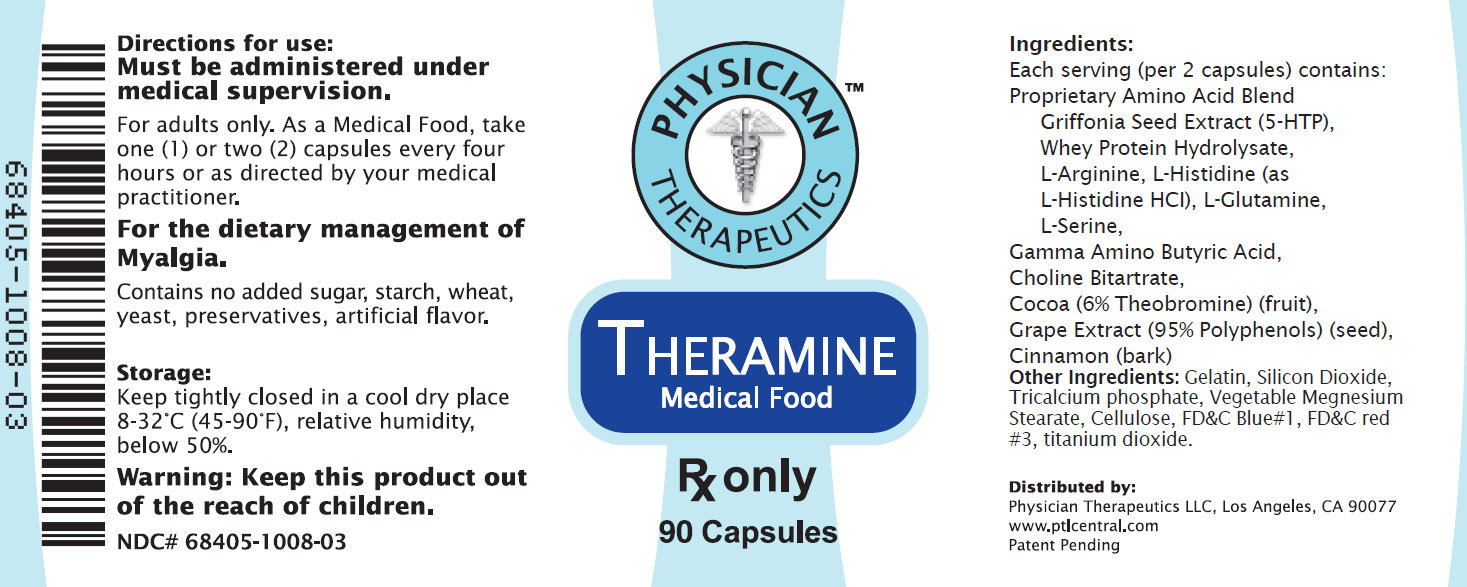
Ingredients:
Each serving (per 2 capsules) contains:
Proprietary Amino Acid Blend Griffonia Seed Extract (5-HTP), Whey Protein Hydrolysate, L-Arginine, L-Histidine (as L-Histidine HCI), L-Glutamine, L-Serine, Gamma Amino Butyric Acid, Choline Bitartrate, Cocoa (6% Theobromine) (fruit), Grape Extract (95% Polyphenols) (seed), Cinnamon (bark)
Other Ingredients: Gelatin, Silicon Dioxide, Tricalcium phosphate, Vegetable Megnesium Stearate, Cellulose, FD C Blue 1, FD C red 3, titanium dioxide.
-
DOSAGE & ADMINISTRATION
Directions for use:
Must be administered under medical supervision.
For adults only. As a Medical Food, take one (1) or two (2) capsules every four hours or as directed by your medical practicioner.
For the dietary management of Myalgia.
Contains no added sugar, starch , wheat, yeast, preservatives, artificial flavor.
- STORAGE AND HANDLING
- WARNINGS
- PRINCIPAL DISPLAY PANEL
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
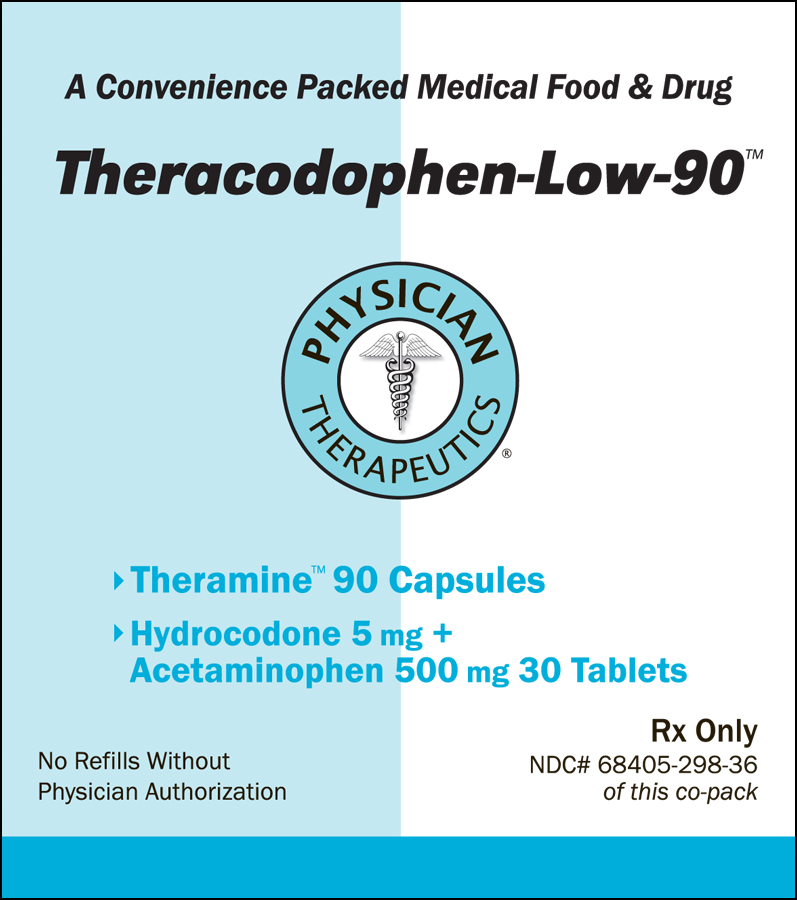
THERACODOPHEN-LOW-90
hydrocodone bitartrate, acetaminophen, .gamma.-aminobutyric acid kitProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:68405-298 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:68405-298-36 1 in 1 KIT Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 BOTTLE 30 Part 2 1 BOTTLE 90 Part 1 of 2 HYDROCODONE BITARTRATE AND ACETAMINOPHEN
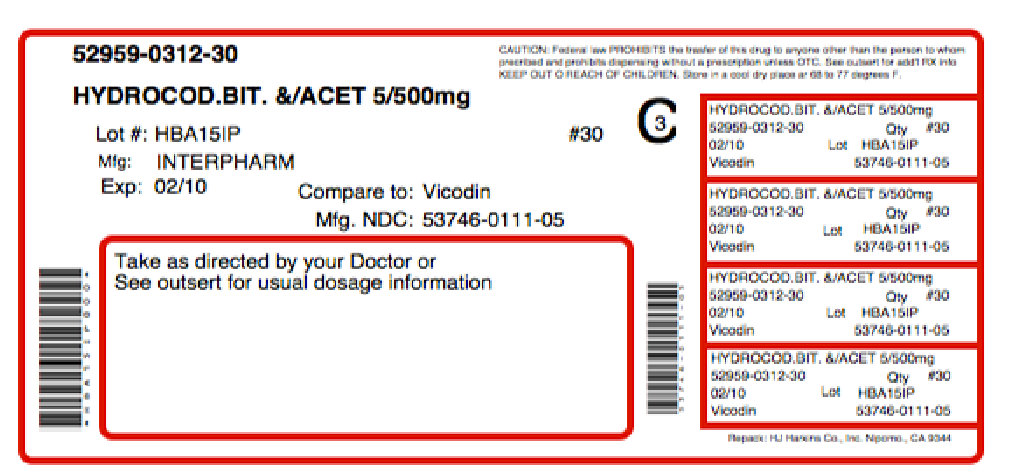
hydrocodone bitartrate, acetaminophen tabletProduct Information Item Code (Source) NDC:52959-312(NDC:53746-111) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength HYDROCODONE BITARTRATE (UNII: NO70W886KK) (HYDROCODONE - UNII:6YKS4Y3WQ7) HYDROCODONE BITARTRATE 5 mg ACETAMINOPHEN (UNII: 362O9ITL9D) (ACETAMINOPHEN - UNII:362O9ITL9D) ACETAMINOPHEN 500 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) Product Characteristics Color white (off-white) Score 2 pieces Shape CAPSULE (bi-convex) Size 17mm Flavor Imprint Code IP;111 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:52959-312-30 30 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA040729 02/02/2011 Part 2 of 2 THERAMINE
.gamma.-aminobutyric acid capsuleProduct Information Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength .GAMMA.-AMINOBUTYRIC ACID (UNII: 2ACZ6IPC6I) (.GAMMA.-AMINOBUTYRIC ACID - UNII:2ACZ6IPC6I) .GAMMA.-AMINOBUTYRIC ACID 100 mg Inactive Ingredients Ingredient Name Strength WHEY (UNII: 8617Z5FMF6) ARGININE (UNII: 94ZLA3W45F) HISTIDINE (UNII: 4QD397987E) GLUTAMINE (UNII: 0RH81L854J) CHOLINE BITARTRATE (UNII: 6K2W7T9V6Y) COCOA (UNII: D9108TZ9KG) THEOBROMINE (UNII: OBD445WZ5P) GRAPE (UNII: 6X543N684K) CINNAMON (UNII: 5S29HWU6QB) GELATIN (UNII: 2G86QN327L) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TRICALCIUM PHOSPHATE (UNII: K4C08XP666) MAGNESIUM STEARATE (UNII: 70097M6I30) POWDERED CELLULOSE (UNII: SMD1X3XO9M) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 3 (UNII: PN2ZH5LOQY) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color purple (PURPLE WHITE) Score no score Shape CAPSULE Size 21mm Flavor Imprint Code ; Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 90 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date Medical Food 02/02/2011 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date unapproved drug other 02/02/2011 Labeler - Physician Therapeutics LLC (931940964) Establishment Name Address ID/FEI Business Operations Amneal Pharmaceuticals, LLC 963900878 manufacture Establishment Name Address ID/FEI Business Operations H.J. Harkins Company, Inc. 147681894 repack Establishment Name Address ID/FEI Business Operations Targeted Medical Pharma Inc. 126962740 manufacture