VALACYCLOVIR HYDROCHLORIDE- valacyclovir tablet, film coated
Mylan Pharmaceuticals Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use VALACYCLOVIR TABLETS safely and effectively. See full prescribing information for VALACYCLOVIR TABLETS.
VALACYCLOVIR tablets, for oral use Initial U.S. Approval: 1995 INDICATIONS AND USAGEValacyclovir tablets are a deoxynucleoside analogue DNA polymerase inhibitor indicated for: Adult Patients (1.1)
Pediatric Patients (1.2)
Limitations of Use (1.3) The efficacy and safety of valacyclovir tablets have not been established in immunocompromised patients other than for the suppression of genital herpes in HIV-1–infected patients. DOSAGE AND ADMINISTRATION
Valacyclovir oral suspension (25 mg/mL or 50 mg/mL) can be prepared from the 500 mg valacyclovir tablets. (2.3) DOSAGE FORMS AND STRENGTHSTablets: 500 mg (unscored), 1 gram (partial break line) (3) CONTRAINDICATIONSHypersensitivity to valacyclovir (e.g., anaphylaxis), acyclovir, or any component of the formulation. (4) WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
To report SUSPECTED ADVERSE REACTIONS, contact Mylan at 1-877-446-3679 (1-877-4-INFO-RX) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling. Revised: 12/2022 |
|||||||||||||||||||||||||||||
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
1.1 Adult Patients
Cold Sores (Herpes Labialis)
Valacyclovir tablets are indicated for treatment of cold sores (herpes labialis). The efficacy of valacyclovir tablets initiated after the development of clinical signs of a cold sore (e.g., papule, vesicle, or ulcer) has not been established.
Genital Herpes
Initial Episode
Valacyclovir tablets are indicated for treatment of the initial episode of genital herpes in immunocompetent adults. The efficacy of treatment with valacyclovir tablets when initiated more than 72 hours after the onset of signs and symptoms has not been established.
Recurrent Episodes
Valacyclovir tablets are indicated for treatment of recurrent episodes of genital herpes in immunocompetent adults. The efficacy of treatment with valacyclovir tablets when initiated more than 24 hours after the onset of signs and symptoms has not been established.
Suppressive Therapy
Valacyclovir tablets are indicated for chronic suppressive therapy of recurrent episodes of genital herpes in immunocompetent and in HIV-1–infected adults. The efficacy and safety of valacyclovir tablets for the suppression of genital herpes beyond 1 year in immunocompetent patients and beyond 6 months in HIV-1–infected patients have not been established.
Reduction of Transmission
Valacyclovir tablets are indicated for the reduction of transmission of genital herpes in immunocompetent adults. The efficacy of valacyclovir tablets for the reduction of transmission of genital herpes beyond 8 months in discordant couples has not been established. The efficacy of valacyclovir tablets for the reduction of transmission of genital herpes in individuals with multiple partners and non-heterosexual couples has not been established. Safer sex practices should be used with suppressive therapy (see current Centers for Disease Control and Prevention [CDC] Sexually Transmitted Diseases Treatment Guidelines).
Herpes Zoster
Valacyclovir tablets are indicated for the treatment of herpes zoster (shingles) in immunocompetent adults. The efficacy of valacyclovir tablets when initiated more than 72 hours after the onset of rash and the efficacy and safety of valacyclovir tablets for treatment of disseminated herpes zoster have not been established.
1.2 Pediatric Patients
Cold Sores (Herpes Labialis)
Valacyclovir tablets are indicated for the treatment of cold sores (herpes labialis) in pediatric patients aged greater than or equal to 12 years. The efficacy of valacyclovir tablets initiated after the development of clinical signs of a cold sore (e.g., papule, vesicle, or ulcer) has not been established.
Chickenpox
Valacyclovir is indicated for the treatment of chickenpox in immunocompetent pediatric patients aged 2 to less than 18 years. Based on efficacy data from clinical trials with oral acyclovir, treatment with valacyclovir should be initiated within 24 hours after the onset of rash [see Clinical Studies (14.4)].
1.3 Limitations of Use
The efficacy and safety of valacyclovir have not been established in:
- •
- Immunocompromised patients other than for the suppression of genital herpes in HIV-1–infected patients with a CD4+ cell count greater than or equal to 100 cells/mm3.
- •
- Patients aged less than 12 years with cold sores (herpes labialis).
- •
- Patients aged less than 2 years or greater than or equal to 18 years with chickenpox.
- •
- Patients aged less than 18 years with genital herpes.
- •
- Patients aged less than 18 years with herpes zoster.
- •
- Neonates and infants as suppressive therapy following neonatal herpes simplex virus (HSV) infection.
2 DOSAGE AND ADMINISTRATION
- •
- Valacyclovir tablets may be given without regard to meals.
- •
- Valacyclovir oral suspension (25 mg/mL or 50 mg/mL) may be prepared extemporaneously from 500-mg valacyclovir tablets for use in pediatric patients for whom a solid dosage form is not appropriate [see Dosage and Administration (2.3)].
2.1 Adult Dosing Recommendations
Cold Sores (Herpes Labialis)
The recommended dosage of valacyclovir tablets for treatment of cold sores is 2 grams twice daily for 1 day taken 12 hours apart. Therapy should be initiated at the earliest symptom of a cold sore (e.g., tingling, itching, or burning).
Genital Herpes
Initial Episode
The recommended dosage of valacyclovir tablets for treatment of initial genital herpes is 1 gram twice daily for 10 days. Therapy was most effective when administered within 48 hours of the onset of signs and symptoms.
Recurrent Episodes
The recommended dosage of valacyclovir tablets for treatment of recurrent genital herpes is 500 mg twice daily for 3 days. Initiate treatment at the first sign or symptom of an episode.
Suppressive Therapy
The recommended dosage of valacyclovir tablets for chronic suppressive therapy of recurrent genital herpes is 1 gram once daily in patients with normal immune function. In patients with a history of 9 or fewer recurrences per year, an alternative dose is 500 mg once daily.
In HIV-1–infected patients with a CD4+ cell count greater than or equal to 100 cells/mm3, the recommended dosage of valacyclovir tablets for chronic suppressive therapy of recurrent genital herpes is 500 mg twice daily.
2.2 Pediatric Dosing Recommendations
Cold Sores (Herpes Labialis)
The recommended dosage of valacyclovir tablets for the treatment of cold sores in pediatric patients aged greater than or equal to 12 years is 2 grams twice daily for 1 day taken 12 hours apart. Therapy should be initiated at the earliest symptom of a cold sore (e.g., tingling, itching, or burning).
Chickenpox
The recommended dosage of valacyclovir for treatment of chickenpox in immunocompetent pediatric patients aged 2 to less than 18 years is 20 mg/kg administered 3 times daily for 5 days. The total dose should not exceed 1 gram 3 times daily. Therapy should be initiated at the earliest sign or symptom [see Use in Specific Populations (8.4), Clinical Pharmacology (12.3), Clinical Studies (14.4)].
2.3 Extemporaneous Preparation of Oral Suspension
Ingredients and Preparation per USP-NF
Valacyclovir tablets 500 mg, cherry flavor, and Suspension Structured Vehicle USP-NF (SSV). Valacyclovir oral suspension (25 mg/mL or 50 mg/mL) should be prepared in lots of 100 mL.
Instructions for Preparing Suspension at Time of Dispensing
- •
- Prepare SSV according to the USP-NF.
- •
- Using a pestle and mortar, grind the required number of valacyclovir 500-mg tablets until a fine powder is produced (5 valacyclovir tablets for 25-mg/mL suspension; 10 valacyclovir tablets for 50-mg/mL suspension).
- •
- Gradually add approximately 5-mL aliquots of SSV to the mortar and triturate the powder until a paste has been produced. Ensure that the powder has been adequately wetted.
- •
- Continue to add approximately 5-mL aliquots of SSV to the mortar, mixing thoroughly between additions, until a concentrated suspension is produced, to a minimum total quantity of 20 mL SSV and a maximum total quantity of 40 mL SSV for both the 25-mg/mL and 50- mg/mL suspensions.
- •
- Transfer the mixture to a suitable 100-mL measuring flask.
- •
- Transfer the cherry flavor* to the mortar and dissolve in approximately 5 mL of SSV. Once dissolved, add to the measuring flask.
- •
- Rinse the mortar at least 3 times with approximately 5-mL aliquots of SSV, transferring the rinsing to the measuring flask between additions.
- •
- Make the suspension to volume (100 mL) with SSV and shake thoroughly to mix.
- •
- Transfer the suspension to an amber glass medicine bottle with a child-resistant closure.
- •
- The prepared suspension should be labeled with the following information “Shake well before using. Store suspension between 2° to 8°C (36° to 46°F) in a refrigerator. Discard after 28 days.”
*The amount of cherry flavor added is as instructed by the suppliers of the cherry flavor.
2.4 Patients with Renal Impairment
Dosage recommendations for adult patients with reduced renal function are provided in Table 1 [see Use in Specific Populations (8.5, 8.6), Clinical Pharmacology (12.3)]. Data are not available for the use of valacyclovir in pediatric patients with a creatinine clearance less than 50 mL/min/1.73 m2.
|
Indications |
Normal Dosage Regimen (Creatinine Clearance ≥ 50 mL/min) |
Creatinine Clearance (mL/min) |
||
|
30-49 |
10-29 |
< 10 |
||
|
Cold sores (Herpes Labialis)
Do not exceed 1 day of treatment. |
Two 2-gram doses taken 12 hours apart |
Two 1-gram doses taken |
Two 500-mg doses taken |
500-mg single dose |
|
Genital herpes: Initial episode |
1 gram every |
no reduction |
1 gram every |
500 mg every |
|
Genital herpes: Recurrent episode |
500 mg every |
no reduction |
500 mg every |
500 mg every |
|
Genital herpes: Suppressive therapy | ||||
|
1 gram every |
no reduction |
500 mg every |
500 mg every |
|
500 mg every |
no reduction |
500 mg every |
500 mg every |
|
500 mg every |
no reduction |
500 mg every |
500 mg every |
|
Herpes zoster |
1 gram every |
1 gram every |
1 gram every |
500 mg every |
Hemodialysis
Patients requiring hemodialysis should receive the recommended dose of valacyclovir tablets after hemodialysis. During hemodialysis, the half-life of acyclovir after administration of valacyclovir tablets is approximately 4 hours. About one-third of acyclovir in the body is removed by dialysis during a 4-hour hemodialysis session.
Peritoneal Dialysis
There is no information specific to administration of valacyclovir tablets in patients receiving peritoneal dialysis. The effect of chronic ambulatory peritoneal dialysis (CAPD) and continuous arteriovenous hemofiltration/dialysis (CAVHD) on acyclovir pharmacokinetics has been studied. The removal of acyclovir after CAPD and CAVHD is less pronounced than with hemodialysis, and the pharmacokinetic parameters closely resemble those observed in patients with end-stage renal disease (ESRD) not receiving hemodialysis. Therefore, supplemental doses of valacyclovir tablets should not be required following CAPD or CAVHD.
3 DOSAGE FORMS AND STRENGTHS
Valacyclovir Tablets, USP are available containing 556.2 mg or 1.112 grams of valacyclovir hydrochloride, USP (hydrous), which are equivalent to 500 mg or 1 gram of valacyclovir, on the anhydrous basis, respectively.
- •
- The 500 mg tablets are white, film-coated, oval, unscored tablets with M122 imprinted with black ink on one side of the tablet and plain on the other side of the tablet.
- •
- The 1 gram tablets are white, film-coated, oval tablets with a partial break line on both sides of the tablet and M123 imprinted with black ink on one side of the tablet.
4 CONTRAINDICATIONS
Valacyclovir tablets are contraindicated in patients who have had a demonstrated clinically significant hypersensitivity reaction (e.g., anaphylaxis) to valacyclovir, acyclovir, or any component of the formulation [see Adverse Reactions (6.3)].
5 WARNINGS AND PRECAUTIONS
5.1 Thrombotic Thrombocytopenic Purpura/Hemolytic Uremic Syndrome (TTP/HUS)
TTP/HUS, in some cases resulting in death, has occurred in patients with advanced HIV-1 disease and also in allogeneic bone marrow transplant and renal transplant recipients participating in clinical trials of valacyclovir tablets at doses of 8 grams per day. Treatment with valacyclovir tablets should be stopped immediately if clinical signs, symptoms, and laboratory abnormalities consistent with TTP/HUS occur.
5.2 Acute Renal Failure
Cases of acute renal failure have been reported in:
- •
- Elderly patients with or without reduced renal function. Caution should be exercised when administering valacyclovir tablets to geriatric patients, and dosage reduction is recommended for those with impaired renal function [see Dosage and Administration (2.4), Use in Specific Populations (8.5)].
- •
- Patients with underlying renal disease who received higher-than-recommended doses of valacyclovir tablets for their level of renal function. Dosage reduction is recommended when administering valacyclovir tablets to patients with renal impairment [see Dosage and Administration (2.4), Use in Specific Populations (8.6)].
- •
- Patients receiving other nephrotoxic drugs. Caution should be exercised when administering valacyclovir tablets to patients receiving potentially nephrotoxic drugs.
- •
- Patients without adequate hydration. Precipitation of acyclovir in renal tubules may occur when the solubility (2.5 mg/mL) is exceeded in the intratubular fluid. Adequate hydration should be maintained for all patients.
In the event of acute renal failure and anuria, the patient may benefit from hemodialysis until renal function is restored [see Dosage and Administration (2.4), Adverse Reactions (6.3)].
5.3 Central Nervous System Effects
Central nervous system adverse reactions, including agitation, hallucinations, confusion, delirium, seizures, and encephalopathy, have been reported in both adult and pediatric patients with or without reduced renal function and in patients with underlying renal disease who received higher-than-recommended doses of valacyclovir tablets for their level of renal function. Elderly patients are more likely to have central nervous system adverse reactions. Valacyclovir tablets should be discontinued if central nervous system adverse reactions occur [see Adverse Reactions (6.3), Use in Specific Populations (8.5, 8.6)].
6 ADVERSE REACTIONS
The following serious adverse reactions are discussed in greater detail in other sections of the labeling:
- •
- Thrombotic Thrombocytopenic Purpura/Hemolytic Uremic Syndrome [see Warnings and Precautions (5.1)].
- •
- Acute Renal Failure [see Warnings and Precautions (5.2)].
- •
- Central Nervous System Effects [see Warnings and Precautions (5.3)].
The most common adverse reactions reported in at least 1 indication by greater than 10% of adult subjects treated with valacyclovir tablets and observed more frequently with valacyclovir tablets compared with placebo are headache, nausea, and abdominal pain. The only adverse reaction reported in greater than 10% of pediatric subjects aged less than 18 years was headache.
6.1 Clinical Trials Experience in Adult Subjects
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Cold Sores (Herpes Labialis)
In clinical trials for the treatment of cold sores, the adverse reactions reported by subjects receiving valacyclovir tablets 2 grams twice daily (n = 609) or placebo (n = 609) for 1 day, respectively, included headache (14%, 10%) and dizziness (2%, 1%). The frequencies of abnormal ALT (greater than 2 x ULN) were 1.8% for subjects receiving valacyclovir tablets compared with 0.8% for placebo. Other laboratory abnormalities (hemoglobin, white blood cells, alkaline phosphatase, and serum creatinine) occurred with similar frequencies in the 2 groups.
Genital Herpes
Initial Episode
In a clinical trial for the treatment of initial episodes of genital herpes, the adverse reactions reported by greater than or equal to 5% of subjects receiving valacyclovir tablets 1 gram twice daily for 10 days (n = 318) or oral acyclovir 200 mg 5 times daily for 10 days (n = 318), respectively, included headache (13%, 10%) and nausea (6%, 6%). For the incidence of laboratory abnormalities see Table 2.
Recurrent Episodes
In 3 clinical trials for the episodic treatment of recurrent genital herpes, the adverse reactions reported by greater than or equal to 5% of subjects receiving valacyclovir tablets 500 mg twice daily for 3 days (n = 402), valacyclovir tablets 500 mg twice daily for 5 days (n = 1,136), or placebo (n = 259), respectively, included headache (16%, 11%, 14%) and nausea (5%, 4%, 5%). For the incidence of laboratory abnormalities see Table 2.
Suppressive Therapy
Suppression of Recurrent Genital Herpes in Immunocompetent Adults
In a clinical trial for the suppression of recurrent genital herpes infections, the adverse reactions reported by subjects receiving valacyclovir tablets 1 gram once daily (n = 269), valacyclovir tablets 500 mg once daily (n = 266), or placebo (n = 134), respectively, included headache (35%, 38%, 34%), nausea (11%, 11%, 8%), abdominal pain (11%, 9%, 6%), dysmenorrhea (8%, 5%, 4%), depression (7%, 5%, 5%), arthralgia (6%, 5%, 4%), vomiting (3%, 3%, 2%), and dizziness (4%, 2%, 1%). For the incidence of laboratory abnormalities see Table 2.
Suppression of Recurrent Genital Herpes in HIV-1–Infected Subjects
In HIV-1–infected subjects, frequently reported adverse reactions for valacyclovir tablets (500 mg twice daily; n = 194, median days on therapy = 172) and placebo (n = 99, median days on therapy = 59), respectively, included headache (13%, 8%), fatigue (8%, 5%), and rash (8%, 1%). Post-randomization laboratory abnormalities that were reported more frequently in valacyclovir subjects versus placebo included elevated alkaline phosphatase (4%, 2%), elevated ALT (14%, 10%), elevated AST (16%, 11%), decreased neutrophil counts (18%, 10%), and decreased platelet counts (3%, 0%), respectively.
Reduction of Transmission
In a clinical trial for the reduction of transmission of genital herpes, the adverse reactions reported by subjects receiving valacyclovir tablets 500 mg once daily (n = 743) or placebo once daily (n = 741), respectively, included headache (29%, 26%), nasopharyngitis (16%, 15%), and upper respiratory tract infection (9%, 10%).
Herpes Zoster
In 2 clinical trials for the treatment of herpes zoster, the adverse reactions reported by subjects receiving valacyclovir tablets 1 gram 3 times daily for 7 to 14 days (n = 967) or placebo (n = 195), respectively, included nausea (15%, 8%), headache (14%, 12%), vomiting (6%, 3%), dizziness (3%, 2%), and abdominal pain (3%, 2%). For the incidence of laboratory abnormalities see Table 2.
| LLN = Lower limit of normal. ULN = Upper limit of normal. |
||||||||
|
||||||||
|
Laboratory Abnormality |
Herpes Zoster |
Genital Herpes Treatment |
Genital Herpes Suppression |
|||||
|
Valacyclovir Tablets 1 gram 3 Times Daily (n = 967) |
Placebo (n = 195) |
Valacyclovir Tablets 1 gram Twice Daily (n = 1,194) |
Valacyclovir Tablets 500 mg Twice Daily (n = 1,159) |
Placebo (n = 439) |
Valacyclovir Tablets 1 gram Once Daily (n = 269) |
Valacyclovir Tablets 500 mg Once Daily (n = 266) |
Placebo (n = 134) |
|
|
Hemoglobin (< 0.8 x LLN) |
0.8% |
0% |
0.3% |
0.2% |
0% |
0% |
0.8% |
0.8% |
|
White blood cells (< 0.75 x LLN) |
1.3% |
0.6% |
0.7% |
0.6% |
0.2% |
0.7% |
0.8% |
1.5% |
|
Platelet count (< 100,000/mm3) |
1.0% |
1.2% |
0.3% |
0.1% |
0.7% |
0.4% |
1.1% |
1.5% |
|
AST (SGOT) (> 2 x ULN) |
1.0% |
0% |
1.0% |
0.5% |
4.1% |
3.8% |
3.0% |
|
|
Serum creatinine (> 1.5 x ULN) |
0.2% |
0% |
0.7% |
0% |
0% |
0% |
0% |
0% |
6.2 Clinical Trials Experience in Pediatric Subjects
The safety profile of valacyclovir tablets has been studied in 177 pediatric subjects aged 1 month to less than 18 years. Sixty-five of these pediatric subjects, aged 12 to less than 18 years, received oral tablets for 1 to 2 days for treatment of cold sores. The remaining 112 pediatric subjects, aged 1 month to less than 12 years, participated in 3 pharmacokinetic and safety trials and received valacyclovir oral suspension. Fifty-one of these 112 pediatric subjects received oral suspension for 3 to 6 days. The frequency, intensity, and nature of clinical adverse reactions and laboratory abnormalities were similar to those seen in adults.
Pediatric Subjects Aged 12 to Less Than 18 Years (Cold Sores)
In clinical trials for the treatment of cold sores, the adverse reactions reported by adolescent subjects receiving valacyclovir tablets 2 grams twice daily for 1 day, or valacyclovir tablets 2 grams twice daily for 1 day followed by 1 gram twice daily for 1 day (n = 65, across both dosing groups), or placebo (n = 30), respectively, included headache (17%, 3%) and nausea (8%, 0%).
Pediatric Subjects Aged 1 Month to Less Than 12 Years
Adverse events reported in more than 1 subject across the 3 pharmacokinetic and safety trials in children aged 1 month to less than 12 years were diarrhea (5%), pyrexia (4%), dehydration (2%), herpes simplex (2%), and rhinorrhea (2%). No clinically meaningful changes in laboratory values were observed.
6.3 Postmarketing Experience
In addition to adverse events reported from clinical trials, the following events have been identified during postmarketing use of valacyclovir tablets. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to valacyclovir tablets.
General: Facial edema, hypertension, tachycardia.
Allergic: Acute hypersensitivity reactions including anaphylaxis, angioedema, dyspnea, pruritus, rash, and urticaria [see Contraindications (4)].
Central Nervous System (CNS) Symptoms: Aggressive behavior; agitation; ataxia; coma; confusion; decreased consciousness; dysarthria; encephalopathy; mania; and psychosis, including auditory and visual hallucinations, seizures, tremors [see Warnings and Precautions (5.3), Use in Specific Populations (8.5, 8.6)].
Eye: Visual abnormalities.
Gastrointestinal: Diarrhea.
Hepatobiliary Tract and Pancreas: Liver enzyme abnormalities, hepatitis.
Renal: Renal failure, renal pain (may be associated with renal failure) [see Warnings and Precautions (5.2), Use in Specific Populations (8.5, 8.6)].
Hematologic: Thrombocytopenia, aplastic anemia, leukocytoclastic vasculitis, TTP/HUS [see Warnings and Precautions (5.1)].
Skin: Erythema multiforme, rashes including photosensitivity, alopecia.
7 DRUG INTERACTIONS
No clinically significant drug-drug or drug-food interactions with valacyclovir tablets are known [see Clinical Pharmacology (12.3)].
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Clinical data over several decades with valacyclovir and its metabolite, acyclovir, in pregnant women, have not identified a drug associated risk of major birth defects. There are insufficient data on the use of valacyclovir regarding miscarriage or adverse maternal or fetal outcomes (see Data). There are risks to the fetus associated with untreated herpes simplex during pregnancy (see Clinical Considerations).
In animal reproduction studies, no evidence of adverse developmental outcomes was observed with valacyclovir when administered to pregnant rats and rabbits at system exposures (AUC) 4 (rats) and 7 (rabbits) times the human exposure at the maximum recommended human dose (MRHD) (see Data).
The estimated background risk of major birth defects and miscarriage for the indicated populations is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
The risk of neonatal HSV infection varies from 30% to 50% for genital HSV acquired in late pregnancy (third trimester), whereas with HSV acquisition in early pregnancy, the risk of neonatal infection is about 1%. A primary herpes occurrence during the first trimester of pregnancy has been associated with neonatal chorioretinitis, microcephaly, and, in rare cases, skin lesions. In very rare cases, transplacental transmission can occur resulting in congenital infection, including microcephaly, hepatosplenomegaly, intrauterine growth restriction, and stillbirth. Co-infection with HSV increases the risk of perinatal HIV transmission in women who had a clinical diagnosis of genital herpes during pregnancy.
Data
Human Data
Clinical data over several decades with valacyclovir and its metabolite, acyclovir, in pregnant women, based on published literature, have not identified a drug-associated risk of major birth defects. There are insufficient data on the use of valacyclovir regarding miscarriage or adverse maternal or fetal outcomes.
The Acyclovir and the Valacyclovir Pregnancy Registries, both population-based international prospective studies, collected pregnancy data through April 1999. The Acyclovir Registry documented outcomes of 1,246 infants and fetuses exposed to acyclovir during pregnancy (756 with earliest exposure during the first trimester, 197 during the second trimester, 291 during the third trimester, and 2 unknown). The occurrence of major birth defects during first-trimester exposure to acyclovir was 3.2% (95% CI: 2.0% to 5.0%) and during any trimester of exposure was 2.6% (95% CI: 1.8% to 3.8%). The Valacyclovir Pregnancy Registry documented outcomes of 111 infants and fetuses exposed to valacyclovir during pregnancy (28 with earliest exposure in the first trimester, 31 during the second trimester, and 52 during the third trimester).The occurrence of major birth defects during first-trimester exposure to valacyclovir was 4.5% (95% CI: 0.24% to 24.9%) and during any trimester of exposure was 3.9% (95% CI: 1.3% to 10.7%).
Available studies have methodological limitations including insufficient sample size to support conclusions about overall malformation risk or for making comparisons of the frequencies of specific birth defects.
Animal Data
Valacyclovir was administered orally to pregnant rats and rabbits (up to 400 mg/kg/day) during organogenesis (Gestation Days 6 through 15, and 6 through 18, respectively). No adverse embryo-fetal effects were observed in rats and rabbits at acyclovir exposures (AUC) of up to approximately 4 (rats) and 7 (rabbits) times the exposure in humans at the MRHD. Early embryo death, fetal growth retardation (weight and length), and variations in fetal skeletal development (primarily extra ribs and delayed ossification of sternebrae) were observed in rats and associated with maternal toxicity (200 mg/kg/day; approximately 6 times higher than human exposure at the MRHD).
In a pre/postnatal development study, valacyclovir was administered orally to pregnant rats (up to 200 mg/kg/day from Gestation Day 15 to Post-Partum Day 20) from late gestation through lactation. No significant adverse effects were observed in offspring exposed daily from before birth through lactation at maternal exposures (AUC) of approximately 6 times higher than human exposures at the MRHD.
8.2 Lactation
Risk Summary
Although there is no information on the presence of valacyclovir in human milk, its metabolite, acyclovir, is present in human milk following oral administration of valacyclovir. Based on published data, a 500-mg maternal dose of valacyclovir tablets twice daily would provide a breastfed child with an oral acyclovir dosage of approximately 0.6 mg/kg/day (see Data). There is no data on the effects of valacyclovir or acyclovir on the breastfed child or on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for valacyclovir tablets and any potential adverse effects on the breastfed child from valacyclovir or from the underlying maternal condition.
Data
Following oral administration of a 500-mg dose of valacyclovir tablets to 5 lactating women, peak acyclovir concentrations (Cmax) in breast milk ranged from 0.5 to 2.3 times (median 1.4) the corresponding maternal acyclovir serum concentrations. The acyclovir breast milk AUC ranged from 1.4 to 2.6 times (median 2.2) maternal serum AUC. A 500-mg maternal dose of valacyclovir tablets twice daily would provide a breastfed child with an oral acyclovir dosage of approximately 0.6 mg/kg/day. Unchanged valacyclovir was not detected in maternal serum, breast milk or infant urine.
8.4 Pediatric Use
Valacyclovir is indicated for treatment of cold sores in pediatric patients aged greater than or equal to 12 years and for treatment of chickenpox in pediatric patients aged 2 to less than 18 years [see Indications and Usage (1.2), Dosage and Administration (2.2)].
The use of valacyclovir tablets for treatment of cold sores is based on 2 double-blind, placebo-controlled clinical trials in healthy adults and adolescents (aged greater than or equal to 12 years) with a history of recurrent cold sores [see Clinical Studies (14.1)].
The use of valacyclovir for treatment of chickenpox in pediatric patients aged 2 to less than 18 years is based on single-dose pharmacokinetic and multiple-dose safety data from an open-label trial with valacyclovir and supported by efficacy and safety data from 3 randomized, double-blind, placebo-controlled trials evaluating oral acyclovir in pediatric subjects with chickenpox [see Dosage and Administration (2.2), Adverse Reactions (6.2), Clinical Pharmacology (12.3), Clinical Studies (14.4)].
The efficacy and safety of valacyclovir have not been established in pediatric patients:
- •
- aged less than 12 years with cold sores
- •
- aged less than 18 years with genital herpes
- •
- aged less than 18 years with herpes zoster
- •
- aged less than 2 years with chickenpox
- •
- for suppressive therapy following neonatal HSV infection.
The pharmacokinetic profile and safety of valacyclovir oral suspension in children aged less than 12 years were studied in 3 open-label trials. No efficacy evaluations were conducted in any of the 3 trials.
Trial 1 was a single-dose pharmacokinetic, multiple-dose safety trial in 27 pediatric subjects aged 1 to less than 12 years with clinically suspected varicella-zoster virus (VZV) infection [see Dosage and Administration (2.2), Adverse Reactions (6.2), Clinical Pharmacology (12.3), Clinical Studies (14.4)].
Trial 2 was a single-dose pharmacokinetic and safety trial in pediatric subjects aged 1 month to less than 6 years who had an active herpes virus infection or who were at risk for herpes virus infection. Fifty-seven subjects were enrolled and received a single dose of 25 mg/kg valacyclovir oral suspension. In infants and children aged 3 months to less than 6 years, this dose provided comparable systemic acyclovir exposures to that from a 1-gram dose of valacyclovir in adults (historical data). In infants aged 1 month to less than 3 months, mean acyclovir exposures resulting from a 25-mg/kg dose were higher (Cmax: ↑ 30%, AUC: ↑ 60%) than acyclovir exposures following a 1-gram dose of valacyclovir in adults. Acyclovir is not approved for suppressive therapy in infants and children following neonatal HSV infections; therefore, valacyclovir is not recommended for this indication because efficacy cannot be extrapolated from acyclovir.
Trial 3 was a single-dose pharmacokinetic, multiple-dose safety trial in 28 pediatric subjects aged 1 to less than 12 years with clinically suspected HSV infection. None of the subjects enrolled in this trial had genital herpes. Each subject was dosed with valacyclovir oral suspension 10 mg/kg twice daily for 3 to 5 days. Acyclovir systemic exposures in pediatric subjects following valacyclovir oral suspension were compared with historical acyclovir systemic exposures in immunocompetent adults receiving the solid oral dosage form of valacyclovir or acyclovir for the treatment of recurrent genital herpes. The mean projected daily acyclovir systemic exposures in pediatric subjects across all age-groups (1 to less than 12 years) were lower (Cmax: ↓ 20%, AUC: ↓ 33%) compared with the acyclovir systemic exposures in adults receiving valacyclovir 500 mg twice daily but were higher (daily AUC: ↑ 16%) than systemic exposures in adults receiving acyclovir 200 mg 5 times daily. Insufficient data are available to support valacyclovir for the treatment of recurrent genital herpes in this age-group because clinical information on recurrent genital herpes in young children is limited; therefore, extrapolating efficacy data from adults to this population is not possible. Moreover, valacyclovir has not been studied in children aged 1 to less than 12 years with recurrent genital herpes.
8.5 Geriatric Use
Of the total number of subjects in clinical trials of valacyclovir tablets, 906 were 65 and over, and 352 were 75 and over. In a clinical trial of herpes zoster, the duration of pain after healing (post-herpetic neuralgia) was longer in subjects 65 and older compared with younger adults. Elderly patients are more likely to have reduced renal function and require dose reduction. Elderly patients are also more likely to have renal or CNS adverse events [see Dosage and Administration (2.4), Warnings and Precautions (5.2, 5.3), Clinical Pharmacology (12.3)].
8.6 Renal Impairment
Dosage reduction is recommended when administering valacyclovir tablets to patients with renal impairment [see Dosage and Administration (2.4), Warnings and Precautions (5.2, 5.3)].
10 OVERDOSAGE
Caution should be exercised to prevent inadvertent overdose [see Use in Specific Populations (8.5, 8.6)]. Precipitation of acyclovir in renal tubules may occur when the solubility (2.5 mg/mL) is exceeded in the intratubular fluid. In the event of acute renal failure and anuria, the patient may benefit from hemodialysis until renal function is restored [see Dosage and Administration (2.4)].
11 DESCRIPTION
Valacyclovir hydrochloride is the hydrochloride salt of the L-valyl ester of the antiviral drug acyclovir.
Valacyclovir tablets, USP are for oral administration. Each tablet contains 556.2 mg or 1.112 grams of valacyclovir hydrochloride, USP (hydrous), which are equivalent to 500 mg or 1 gram of valacyclovir, on the anhydrous basis, respectively, and the inactive ingredients hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol and titanium dioxide. The white, film-coated tablets are printed with edible black ink which contains black iron oxide, propylene glycol and shellac glaze.
The chemical name of valacyclovir hydrochloride is L-valine, 2-[(2-amino-1,6-dihydro-6-oxo-9H-purin-9-yl)methoxy]ethyl ester, monohydrochloride. It has the following structural formula:
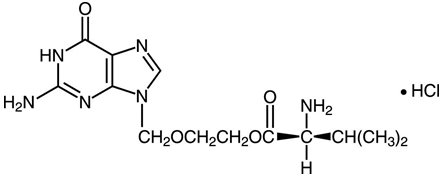
Valacyclovir hydrochloride, USP (hydrous) is a white to off-white powder with the molecular formula C13H20N6O4•HCl and a molecular weight of 360.80. The maximum solubility in water at 25°C is 174 mg/mL. The pkas for valacyclovir hydrochloride are 7.47 and 9.43.
Meets USP Dissolution Test 2.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Valacyclovir is an antiviral drug active against α-herpes viruses [see Microbiology (12.4)].
12.3 Pharmacokinetics
The pharmacokinetics of valacyclovir and acyclovir after oral administration of valacyclovir tablets have been investigated in 14 volunteer trials involving 283 adults and in 3 trials involving 112 pediatric subjects aged 1 month to less than 12 years.
Pharmacokinetics in Adults
Absorption and Bioavailability
After oral administration, valacyclovir hydrochloride is rapidly absorbed from the gastrointestinal tract and nearly completely converted to acyclovir and L-valineby first-pass intestinal and/or hepatic metabolism.
The absolute bioavailability of acyclovir after administration of valacyclovir tablets is 54.5% ± 9.1% as determined following a 1-gram oral dose of valacyclovir tablets and a 350-mg intravenous acyclovir dose to 12 healthy volunteers. Acyclovir bioavailability from the administration of valacyclovir tablets is not altered by administration with food (30 minutes after an 873 Kcal breakfast, which included 51 grams of fat).
Acyclovir pharmacokinetic parameter estimates following administration of valacyclovir tablets to healthy adult volunteers are presented in Table 3. There was a less than dose-proportional increase in acyclovir maximum concentration (Cmax) and area under the acyclovir concentration-time curve (AUC) after single-dose and multiple-dose administration (4 times daily) of valacyclovir tablets from doses between 250 mg to 1 gram.
There is no accumulation of acyclovir after the administration of valacyclovir at the recommended dosage regimens in adults with normal renal function.
| ND = not done. | ||||
|
||||
|
Dose |
Single-Dose Administration (N = 8) |
Multiple-Dose Administration* (N = 24, 8 per treatment arm) |
||
|
Cmax (± SD) (mcg/mL) |
AUC (± SD) |
Cmax (± SD) (mcg/mL) |
AUC (± SD) |
|
|
100 mg |
0.83 (± 0.14) |
2.28 (± 0.40) |
ND |
ND |
|
250 mg |
2.15 (± 0.50) |
5.76 (± 0.60) |
2.11 (± 0.33) |
5.66 (± 1.09) |
|
500 mg |
3.28 (± 0.83) |
11.59 (± 1.79) |
3.69 (± 0.87) |
9.88 (± 2.01) |
|
750 mg |
4.17 (± 1.14) |
14.11 (± 3.54) |
ND |
ND |
|
1,000 mg |
5.65 (± 2.37) |
19.52 (± 6.04) |
4.96 (± 0.64) |
15.70 (± 2.27) |
Distribution
The binding of valacyclovir to human plasma proteins ranges from 13.5% to 17.9%. The binding of acyclovir to human plasma proteins ranges from 9% to 33%.
Metabolism
Valacyclovir is converted to acyclovir and L-valine by first-pass intestinal and/or hepatic metabolism. Acyclovir is converted to a small extent to inactive metabolites by aldehyde oxidase and by alcohol and aldehyde dehydrogenase. Neither valacyclovir nor acyclovir is metabolized by cytochrome P450 enzymes. Plasma concentrations of unconverted valacyclovir are low and transient, generally becoming non-quantifiable by 3 hours after administration. Peak plasma valacyclovir concentrations are generally less than 0.5 mcg/mL at all doses. After single-dose administration of 1 gram of valacyclovir tablets, average plasma valacyclovir concentrations observed were 0.5, 0.4, and 0.8 mcg/mL in subjects with hepatic dysfunction, renal insufficiency, and in healthy subjects who received concomitant cimetidine and probenecid, respectively.
Elimination
The pharmacokinetic disposition of acyclovir delivered by valacyclovir is consistent with previous experience from intravenous and oral acyclovir. Following the oral administration of a single 1-gram dose of radiolabeled valacyclovir to 4 healthy subjects, 46% and 47% of administered radioactivity was recovered in urine and feces, respectively, over 96 hours. Acyclovir accounted for 89% of the radioactivity excreted in the urine. Renal clearance of acyclovir following the administration of a single 1-gram dose of valacyclovir tablets to 12 healthy subjects was approximately 255 ± 86 mL/min which represents 42% of total acyclovir apparent plasma clearance.
The plasma elimination half-life of acyclovir typically averaged 2.5 to 3.3 hours in all trials of valacyclovir tablets in subjects with normal renal function.
Specific Populations
Patients with Renal Impairment
Reduction in dosage is recommended in patients with renal impairment [see Dosage and Administration (2.4), Use in Specific Populations (8.5, 8.6)].
Following administration of valacyclovir tablets to subjects with ESRD, the average acyclovir half-life is approximately 14 hours. During hemodialysis, the acyclovir half-life is approximately 4 hours. Approximately one-third of acyclovir in the body is removed by dialysis during a 4-hour hemodialysis session. Apparent plasma clearance of acyclovir in subjects on dialysis was 86.3 ± 21.3 mL/min/1.73 m2 compared with 679.16 ± 162.76 mL/min/1.73 m2 in healthy subjects.
Patients with Hepatic Impairment
Administration of valacyclovir tablets to subjects with moderate (biopsy-proven cirrhosis) or severe (with and without ascites and biopsy-proven cirrhosis) liver disease indicated that the rate but not the extent of conversion of valacyclovir to acyclovir is reduced, and the acyclovir half-life is not affected. Dosage modification is not recommended for patients with cirrhosis.
Patients with HIV-1 Disease
In 9 subjects with HIV-1 disease and CD4+ cell counts less than 150 cells/mm3 who received valacyclovir tablets at a dosage of 1 gram 4 times daily for 30 days, the pharmacokinetics of valacyclovir and acyclovir were not different from that observed in healthy subjects.
Geriatric Patients
After single-dose administration of 1 gram of valacyclovir tablets in healthy geriatric subjects, the half-life of acyclovir was 3.11 ± 0.51 hours compared with 2.91 ± 0.63 hours in healthy younger adult subjects. The pharmacokinetics of acyclovir following single- and multiple-dose oral administration of valacyclovir tablets in geriatric subjects varied with renal function. Dose reduction may be required in geriatric patients, depending on the underlying renal status of the patient [see Dosage and Administration (2.4), Use in Specific Populations (8.5, 8.6)].
Pediatric Patients
Acyclovir pharmacokinetics have been evaluated in a total of 98 pediatric subjects (aged 1 month to less than 12 years) following administration of the first dose of an extemporaneous oral suspension of valacyclovir [see Adverse Reactions (6.2), Use in Specific Populations (8.4)]. Acyclovir pharmacokinetic parameter estimates following a 20-mg/kg dose are provided in Table 4.
|
||||
|
Parameter |
Pediatric Subjects (20 mg/kg Oral Suspension) |
Adults 1-gram Solid Dose of Valacyclovir Tablets* (N = 15) |
||
|
1 - < 2 year (N = 6) |
2 - < 6 year (N = 12) |
6 - < 12 year (N = 8) |
||
|
AUC (mcg•hr/mL) |
14.4 (± 6.26) |
10.1 (± 3.35) |
13.1 (± 3.43) |
17.2 (± 3.10) |
|
Cmax (mcg/mL) |
4.03 (± 1.37) |
3.75 (± 1.14) |
4.71 (± 1.20) |
4.72 (± 1.37) |
Drug Interaction Studies
When valacyclovir tablets are coadministered with antacids, cimetidine and/or probenecid, digoxin, or thiazide diuretics in patients with normal renal function, the effects are not considered to be of clinical significance (see below). Therefore, when valacyclovir tablets are coadministered with these drugs in patients with normal renal function, no dosage adjustment is recommended.
Antacids
The pharmacokinetics of acyclovir after a single dose of valacyclovir tablets (1 gram) were unchanged by coadministration of a single dose of antacids (Al3+ or Mg++).
Cimetidine
Acyclovir Cmax and AUC following a single dose of valacyclovir tablets (1 gram) increased by 8% and 32%, respectively, after a single dose of cimetidine (800 mg).
Cimetidine Plus Probenecid
Acyclovir Cmax and AUC following a single dose of valacyclovir tablets (1 gram) increased by 30% and 78%, respectively, after a combination of cimetidine and probenecid, primarily due to a reduction in renal clearance of acyclovir.
Digoxin
The pharmacokinetics of digoxin were not affected by coadministration of valacyclovir tablets 1 gram 3 times daily, and the pharmacokinetics of acyclovir after a single dose of valacyclovir tablets (1 gram) was unchanged by coadministration of digoxin (2 doses of 0.75 mg).
12.4 Microbiology
Mechanism of Action
Valacyclovir is a deoxynucleoside analogue DNA polymerase inhibitor. Valacyclovir hydrochloride is rapidly converted to acyclovir, which has demonstrated antiviral activity against HSV types 1 (HSV-1) and 2 (HSV-2) and VZV both in cell culture and in vivo.
Acyclovir is a synthetic purine deoxynucleoside that is phosphorylated intracellularly by the viral encoded thymidine kinase (TK; pUL23) of HSV or VZV into acyclovir monophosphate, a nucleotide analogue. The monophosphate is further converted into diphosphate by cellular guanylate kinase and into triphosphate by a number of cellular enzymes. In biochemical assays, acyclovir triphosphate inhibits replication of α-herpes viral DNA. This is accomplished in 3 ways: 1) competitive inhibition of viral DNA polymerase, 2) incorporation and termination of the growing viral DNA chain, and 3) inactivation of the viral DNA polymerase. The greater antiviral activity of acyclovir against HSV compared with VZV is due to its more efficient phosphorylation by the viral TK.
Antiviral Activity
The quantitative relationship between the cell culture susceptibility of herpes viruses to antivirals and the clinical response to therapy has not been established in humans, and virus sensitivity testing has not been standardized. Sensitivity testing results, expressed as the concentration of drug required to inhibit by 50% the growth of virus in cell culture (EC50), vary greatly depending upon a number of factors. Using plaque-reduction assays, the EC50 values against herpes simplex virus isolates range from 0.09 to 60 microM (0.02 to 13.5 mcg/mL) for HSV-1 and from 0.04 to 44 microM (0.01 to 9.9 mcg/mL) for HSV-2. The EC50 values for acyclovir against most laboratory strains and clinical isolates of VZV range from 0.53 to 48 microM (0.12 to 10.8 mcg/mL). Acyclovir also demonstrates activity against the Oka vaccine strain of VZV with a mean EC50 value of 6 microM (1.35 mcg/mL).
Resistance
In Cell Culture
Acyclovir-resistant HSV-1, HSV-2, and VZV strains were isolated in cell culture. Acyclovir-resistant HSV and VZV resulted from mutations in the viral thymidine kinase (TK, pUL23) and DNA polymerase (POL; pUL30) genes. Frameshifts were commonly isolated and result in premature truncation of the HSV TK product with consequent decreased susceptibility to acyclovir. Mutations in the viral TK gene may lead to complete loss of TK activity (TK negative), reduced levels of TK activity (TK partial), or alteration in the ability of viral TK to phosphorylate the drug without an equivalent loss in the ability to phosphorylate thymidine (TK altered). In cell culture, acyclovir resistance-associated substitutions in TK of HSV-1 and HSV-2 were observed (Table 5).
|
Virus |
Gene |
Substitution |
|
HSV-1 |
TK |
P5A, H7Q, L50V, G56V, G59R/V/W/A, G61A/V, K62I/N, T63A, E83K, P84L/S, R89W, D116N, P131S, P155R, F161I/C, R163H/P, A167V, P173L, R176Q/W, Q185R, A189L/V, G200S, G206R, R216S, R220H, L227F, Y239S, T245M, Q261stop, R281stop, T287M, M322K, C336Y, V348A |
|
HSV-2 |
TK |
L69P, C172R, A175V, T288M |
|
HSV-1 |
POL |
D368A, Y557S, E597D, V621S, L702H, A719V, S742N, N815S, V817M, Y818C, G841C/S |
|
HSV-2 |
POL |
No substitutions detected |
HSV-Infected Patients
Clinical HSV-1 and HSV-2 isolates obtained from patients who failed treatment for their α-herpes virus infections were evaluated for genotypic changes in the TK and POL genes and for phenotypic resistance to acyclovir (Table 6). HSV isolates with frameshift mutations and resistance-associated substitutions in TK and POL were identified. The listing of substitutions in the HSV TK and POL leading to decreased susceptibility to acyclovir is not all inclusive and additional changes will likely be identified in HSV variants isolated from patients who fail acyclovir-containing regimens. The possibility of viral resistance to acyclovir should be considered in patients who fail to respond or experience recurrent viral shedding during therapy.
| Note: Many additional pathways to acyclovir resistance likely exist. | ||
|
Virus |
Gene |
Substitution |
|
HSV-1 |
TK |
G6C, R32H, R41H, R51W, Y53C/D/H, Y53stop, D55N, G56D/E/S, P57H, G58N/R, G59R, G61A/E/W, K62N, T63I, Q67stop, S74stop, Y80N, E83K, P84L, Y87H, E95stop, T103P, Q104H, Q104stop, H105P, M121K/L/R, Q125N, M128L, G129D, I143V, A156V, D162A/H/N, R163G/H, L170P, Y172C, P173L/R, A174P, A175V, R176Q/W, R176stop, L178R, S181N, A186P, V187M, A189V, V192A, G200C/D/S, T201P, T202A, V204G, A207P, L208F/H, R216C/H, R220C/H, R221C/H, R222C/H, E226K, D229H, L242P, T245M/P, L249P, Q250stop, C251G, E257K, Q261R, A265T, R281stop, T287M, L288stop, L291R, L297S, L315S, L327R, C336Y, C336stop, Q342stop, T354P, L364P, A365T |
|
HSV-2 |
TK |
G25A, R34C, G39E, R51W, Y53N/D, G59P, G61A/E/W, S66P, A72S, D78N, P85S, R86P, A94V, L98stop, N100H, I101S, Q103stop, Q105P, A125T, T131P, Y133F, D137stop, F140L, L158P, S169P, R177W, S182N, M183Istop, V192M, G201D, R217H, R221C/H, Q222stop, R223H, D229stop, Y239stop, D231N, L263stop, R271V, P272S, D273R, T287M, C337Y |
|
HSV-1 |
POL |
K532T, S559L, Q570R, L583V, A605V, V621S, A657T, D672N, V715G, A719T/V, S724N, F733C, E771Q, S775N, L778M, E798K, V813M, N815S, G841S, R842S, I890M, V958L, H1228D |
|
HSV-2 |
POL |
E250Q, D307N, K533E, A606V, C625R, R628C, E678G, A724V, S725G, S729N, I731F, Q732R, D785N, M789K/T, V818A, N820S, Y823C, Q829R, T843A, M910T, D912N/V, A915V, F923L, T934A, R964H |
Cross Resistance
Cross-resistance has been observed among HSV isolates carrying frameshift mutations and resistance-associated substitutions, which confer reduced susceptibility to penciclovir (PCV), famciclovir (FCV), and foscarnet (FOS) (Table 7).
|
Cross-Resistant Drug |
Virus/Gene |
Substitution |
|
PCV/FCV |
HSV-1 TK |
G6C, R32H, R51W, Y53C/H/N, H58N, G61A, S74stop, E83K, P84L, T103P, Q104stop, D116N, M121R, I143V, P155R, R163G/H, A167V, L170P, Y172C, P173L, A174P, R176Q/W, Q185R, A186P, A189L/V, G200D/S, G206R, L208H, R216C, R220H, R222C/H, Y239S, T245M, Q250stop, Q261stop, R281stop, T287M, L315S, M322K, C336Y, V348A |
|
HSV-1 POL |
A657T, D672N, V715G, A719V, S724N, E798K, N815S, G841C/S |
|
|
HSV-2 TK |
G39E, R51W, Y53N, R86P, Y133F, R177W, R221H, T288M |
|
|
HSV-2 POL |
K533E, A606V, C625R, R628C, S729N, Q732R, M789K/T, V818A, N820S, F923L, T934A |
|
|
FOS |
HSV-1 POL |
D368A, A605V, D672N, L702H, V715G, A719T/V, S724N, L778M, E798K, V813M, N815S, V817M, G841C/S, I890M |
|
HSV-2 POL |
K533E, A606V, C625R, R628C, A724V, S725G, S729N, I731F, Q732R, M789K/T, V818A, Y823C, D912V, F923L, T934A, R964H |
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
The data presented below include references to the steady-state acyclovir AUC observed in humans treated with 1 gram of valacyclovir tablets given orally 3 times a day to treat herpes zoster. Plasma drug concentrations in animal studies are expressed as multiples of human exposure to acyclovir [see Clinical Pharmacology (12.3)].
Carcinogenesis
Valacyclovir was noncarcinogenic in lifetime carcinogenicity bioassays at single daily doses (gavage) of valacyclovir giving plasma acyclovir concentrations equivalent to human levels in the mouse bioassay and 1.4 to 2.3 times human levels in the rat bioassay. There was no significant difference in the incidence of tumors between treated and control animals, nor did valacyclovir shorten the latency of tumors.
Mutagenesis
Valacyclovir was tested in 5 genetic toxicity assays. An Ames assay was negative in the absence or presence of metabolic activation. Also negative were an in vitro cytogenetic study with human lymphocytes and a rat cytogenetic study.
In the mouse lymphoma assay, valacyclovir was not mutagenic in the absence of metabolic activation. In the presence of metabolic activation (76% to 88% conversion to acyclovir), valacyclovir was mutagenic.
Valacyclovir was mutagenic in a mouse micronucleus assay.
14 CLINICAL STUDIES
14.1 Cold Sores (Herpes Labialis)
Two double-blind, placebo-controlled clinical trials were conducted in 1,856 healthy adults and adolescents (aged greater than or equal to 12 years) with a history of recurrent cold sores. Subjects self-initiated therapy at the earliest symptoms and prior to any signs of a cold sore. The majority of subjects initiated treatment within 2 hours of onset of symptoms. Subjects were randomized to valacyclovir tablets 2 grams twice daily on Day 1 followed by placebo on Day 2, valacyclovir tablets 2 grams twice daily on Day 1 followed by 1 gram twice daily on Day 2, or placebo on Days 1 and 2.
The mean duration of cold sore episodes was about 1 day shorter in treated subjects as compared with placebo. The 2-day regimen did not offer additional benefit over the 1-day regimen.
No significant difference was observed between subjects receiving valacyclovir tablets or placebo in the prevention of progression of cold sore lesions beyond the papular stage.
14.2 Genital Herpes Infections
Initial Episode
Six hundred forty-three immunocompetent adults with first-episode genital herpes who presented within 72 hours of symptom onset were randomized in a double-blind trial to receive 10 days of valacyclovir tablets 1 gram twice daily (n = 323) or oral acyclovir 200 mg 5 times a day (n = 320). For both treatment groups the median time to lesion healing was 9 days, the median time to cessation of pain was 5 days, and the median time to cessation of viral shedding was 3 days.
Recurrent Episodes
Three double-blind trials (2 of them placebo-controlled) in immunocompetent adults with recurrent genital herpes were conducted. Subjects self-initiated therapy within 24 hours of the first sign or symptom of a recurrent genital herpes episode.
In 1 trial, subjects were randomized to receive 5 days of treatment with either valacyclovir tablets 500 mg twice daily (n = 360) or placebo (n = 259). The median time to lesion healing was 4 days in the group receiving valacyclovir tablets 500 mg versus 6 days in the placebo group, and the median time to cessation of viral shedding in subjects with at least 1 positive culture (42% of the overall trial population) was 2 days in the group receiving valacyclovir tablets 500 mg versus 4 days in the placebo group. The median time to cessation of pain was 3 days in the group receiving valacyclovir tablets 500 mg versus 4 days in the placebo group. Results supporting efficacy were replicated in a second trial.
In a third trial, subjects were randomized to receive valacyclovir tablets 500 mg twice daily for 5 days (n = 398) or valacyclovir tablets 500 mg twice daily for 3 days (and matching placebo twice daily for 2 additional days) (n = 402). The median time to lesion healing was about 4½ days in both treatment groups. The median time to cessation of pain was about 3 days in both treatment groups.
Suppressive Therapy
Two clinical trials were conducted, one in immunocompetent adults and one in HIV-1–infected adults.
A double-blind, 12-month, placebo- and active-controlled trial enrolled immunocompetent adults with a history of 6 or more recurrences per year. Outcomes for the overall trial population are shown in Table 8.
|
||||||
|
Outcome |
6 Months |
12 Months |
||||
|
Valacyclovir Tablets 1 gram Once Daily (n = 269) |
Oral Acyclovir 400 mg Twice Daily (n = 267) |
Placebo (n = 134) |
Valacyclovir Tablets 1 gram Once Daily (n = 269) |
Oral Acyclovir 400 mg Twice Daily (n = 267) |
Placebo (n = 134) |
|
|
Recurrence free |
55% |
54% |
7% |
34% |
34% |
4% |
|
Recurrences |
35% |
36% |
83% |
46% |
46% |
85% |
|
Unknown* |
10% |
10% |
10% |
19% |
19% |
10% |
Subjects with 9 or fewer recurrences per year showed comparable results with valacyclovir tablets 500 mg once daily.
In a second trial, 293 HIV-1–infected adults on stable antiretroviral therapy with a history of 4 or more recurrences of ano-genital herpes per year were randomized to receive either valacyclovir tablets 500 mg twice daily (n = 194) or matching placebo (n = 99) for 6 months. The median duration of recurrent genital herpes in enrolled subjects was 8 years, and the median number of recurrences in the year prior to enrollment was 5. Overall, the median pretrial HIV-1 RNA was 2.6 log10 copies/mL. Among subjects who received valacyclovir tablets, the pretrial median CD4+ cell count was 336 cells/mm3; 11% had less than 100 cells/mm3, 16% had 100 to 199 cells/mm3, 42% had 200 to 499 cells/mm3, and 31% had greater than or equal to 500 cells/mm3. Outcomes for the overall trial population are shown in Table 9.
|
||
|
Outcome |
Valacyclovir Tablets 500 mg Twice Daily (n = 194) |
Placebo (n = 99) |
|
Recurrence free |
65% |
26% |
|
Recurrences |
17% |
57% |
|
Unknown* |
18% |
17% |
Reduction of Transmission of Genital Herpes
A double-blind, placebo-controlled trial to assess transmission of genital herpes was conducted in 1,484 monogamous, heterosexual, immunocompetent adult couples. The couples were discordant for HSV-2 infection. The source partner had a history of 9 or fewer genital herpes episodes per year. Both partners were counseled on safer sex practices and were advised to use condoms throughout the trial period. Source partners were randomized to treatment with either valacyclovir tablets 500 mg once daily or placebo once daily for 8 months. The primary efficacy endpoint was symptomatic acquisition of HSV-2 in susceptible partners. Overall HSV-2 acquisition was defined as symptomatic HSV-2 acquisition and/or HSV-2 seroconversion in susceptible partners. The efficacy results are summarized in Table 10.
|
||
|
Endpoint |
Valacyclovir Tablets* (n = 743) |
Placebo (n = 741) |
|
Symptomatic HSV-2 acquisition |
4 (0.5%) |
16 (2.2%) |
|
HSV-2 seroconversion |
12 (1.6%) |
24 (3.2%) |
|
Overall HSV-2 acquisition |
14 (1.9%) |
27 (3.6%) |
14.3 Herpes Zoster
Two randomized, double-blind clinical trials in immunocompetent adults with localized herpes zoster were conducted. Valacyclovir tablets were compared with placebo in subjects aged less than 50 years and with oral acyclovir in subjects aged greater than 50 years. All subjects were treated within 72 hours of appearance of zoster rash. In subjects aged less than 50 years, the median time to cessation of new lesion formation was 2 days for those treated with valacyclovir tablets compared with 3 days for those treated with placebo. In subjects aged greater than 50 years, the median time to cessation of new lesions was 3 days in subjects treated with either valacyclovir tablets or oral acyclovir. In subjects aged less than 50 years, no difference was found with respect to the duration of pain after healing (post-herpetic neuralgia) between the recipients of valacyclovir tablets and placebo. In subjects aged greater than 50 years, among the 83% who reported pain after healing (post-herpetic neuralgia), the median duration of pain after healing (95% CI) in days was: 40 (31, 51), 43 (36, 55), and 59 (41, 77) for 7-day valacyclovir tablets, 14-day valacyclovir tablets, and 7-day oral acyclovir, respectively.
14.4 Chickenpox
The use of valacyclovir for treatment of chickenpox in pediatric subjects aged 2 to less than 18 years is based on single-dose pharmacokinetic and multiple-dose safety data from an open-label trial with valacyclovir and supported by safety and extrapolated efficacy data from 3 randomized, double-blind, placebo-controlled trials evaluating oral acyclovir in pediatric subjects.
The single-dose pharmacokinetic and multiple-dose safety trial enrolled 27 pediatric subjects aged 1 to less than 12 years with clinically suspected VZV infection. Each subject was dosed with valacyclovir oral suspension, 20 mg/kg 3 times daily for 5 days. Acyclovir systemic exposures in pediatric subjects following valacyclovir oral suspension were compared with historical acyclovir systemic exposures in immunocompetent adults receiving the solid oral dosage form of valacyclovir or acyclovir for the treatment of herpes zoster. The mean projected daily acyclovir exposures in pediatric subjects across all age-groups (1 to less than 12 years) were lower (Cmax: ↓ 13%, AUC: ↓ 30%) than the mean daily historical exposures in adults receiving valacyclovir 1 gram 3 times daily, but were higher (daily AUC: ↑ 50%) than the mean daily historical exposures in adults receiving acyclovir 800 mg 5 times daily. The projected daily exposures in pediatric subjects were greater (daily AUC approximately 100% greater) than the exposures seen in immunocompetent pediatric subjects receiving acyclovir 20 mg/kg 4 times daily for the treatment of chickenpox. Based on the pharmacokinetic and safety data from this trial and the safety and extrapolated efficacy data from the acyclovir trials, oral valacyclovir 20 mg/kg 3 times a day for 5 days (not to exceed 1 gram 3 times daily) is recommended for the treatment of chickenpox in pediatric patients aged 2 to less than 18 years. Because the efficacy and safety of acyclovir for the treatment of chickenpox in children aged less than 2 years have not been established, efficacy data cannot be extrapolated to support valacyclovir treatment in children aged less than 2 years with chickenpox. Valacyclovir is also not recommended for the treatment of herpes zoster in children because safety data up to 7 days’ duration are not available [see Use in Specific Populations (8.4)].
16 HOW SUPPLIED/STORAGE AND HANDLING
Valacyclovir Tablets, USP are available containing 556.2 mg or 1.112 grams of valacyclovir hydrochloride, USP (hydrous), which are equivalent to 500 mg or 1 gram of valacyclovir, on the anhydrous basis, respectively.
The 500 mg tablets are white, film-coated, oval, unscored tablets with M122 imprinted with black ink on one side of the tablet and plain on the other side of the tablet. They are available as follows:
NDC 0378-4275-93
bottles of 30 tablets
NDC 0378-4275-77
bottles of 90 tablets
The 1 gram tablets are white, film-coated, oval tablets with a partial break line on both sides of the tablet and M123 imprinted with black ink on one side of the tablet. They are available as follows:
NDC 0378-4276-93
bottles of 30 tablets
NDC 0378-4276-77
bottles of 90 tablets
Storage: Store at 20º to 25ºC (68º to 77ºF). [See USP Controlled Room Temperature.] Dispense in a tight, light-resistant container as defined in the USP using a child-resistant closure.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Importance of Adequate Hydration: Patients should be advised to maintain adequate hydration.
Missed Dose: Instruct patients that if they miss a dose of valacyclovir tablets, to take it as soon as they remember. Advise patients not to double their next dose or take more than the prescribed dose.
Cold Sores (Herpes Labialis): Patients should be advised to initiate treatment at the earliest symptom of a cold sore (e.g., tingling, itching, or burning). There are no data on the effectiveness of treatment initiated after the development of clinical signs of a cold sore (e.g., papule, vesicle, or ulcer). Patients should be instructed that treatment for cold sores should not exceed 1 day (2 doses) and that their doses should be taken about 12 hours apart. Patients should be informed that valacyclovir tablets are not a cure for cold sores.
Genital Herpes: Patients should be informed that valacyclovir tablets are not a cure for genital herpes. Because genital herpes is a sexually transmitted disease, patients should avoid contact with lesions or intercourse when lesions and/or symptoms are present to avoid infecting partners. Genital herpes is frequently transmitted in the absence of symptoms through asymptomatic viral shedding. Therefore, patients should be counseled to use safer sex practices in combination with suppressive therapy with valacyclovir tablets. Sex partners of infected persons should be advised that they might be infected even if they have no symptoms. Type-specific serologic testing of asymptomatic partners of persons with genital herpes can determine whether risk for HSV-2 acquisition exists.
Valacyclovir tablets have not been shown to reduce transmission of sexually transmitted infections other than HSV-2.
If medical management of a genital herpes recurrence is indicated, patients should be advised to initiate therapy at the first sign or symptom of an episode.
There are no data on the effectiveness of treatment initiated more than 72 hours after the onset of signs and symptoms of a first episode of genital herpes or more than 24 hours after the onset of signs and symptoms of a recurrent episode.
There are no data on the safety or effectiveness of chronic suppressive therapy of more than 1 year’s duration in otherwise healthy patients. There are no data on the safety or effectiveness of chronic suppressive therapy of more than 6 months’ duration in HIV-1–infected patients.
Herpes Zoster: There are no data on treatment initiated more than 72 hours after onset of the zoster rash. Patients should be advised to initiate treatment as soon as possible after a diagnosis of herpes zoster.
Chickenpox: Patients should be advised to initiate treatment at the earliest sign or symptom of chickenpox.
Patient Information
|
Valacyclovir Tablets, USP |
|
|
What are valacyclovir tablets? Valacyclovir tablets are a prescription medicine used in adults:
Valacyclovir tablets are used in children to treat:
Valacyclovir tablets do not cure cold sores, chickenpox, shingles, or genital herpes.
|
|
|
Do not take valacyclovir tablets if you are allergic to valacyclovir, acyclovir, or any of the ingredients in valacyclovir tablets. See the end of this leaflet for a complete list of ingredients in valacyclovir tablets. |
|
|
Before you take valacyclovir tablets, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. |
|
|
How should I take valacyclovir tablets?
|
|
|
What are the possible side effects of valacyclovir tablets? Valacyclovir tablets can cause serious side effects including:
|
|
|
|
|
Elderly people are more likely to get certain side effects. Talk to your healthcare provider if this is a concern for you.
The most common side effects of valacyclovir tablets in adults include: |
|
|
|
|
The most common side effect of valacyclovir tablets in children less than 18 years of age is headache.
These are not all the possible side effects of valacyclovir tablets.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
How should I store valacyclovir tablets?
Keep valacyclovir tablets and all medicines out of the reach of children. |
|
|
General information about the safe and effective use of valacyclovir tablets. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use valacyclovir tablets for a condition for which they were not prescribed. Do not give valacyclovir tablets to other people, even if they have the same symptoms that you have. They may harm them. You can ask your healthcare provider or pharmacist for information about valacyclovir tablets that is written for health professionals. |
|
|
What are the ingredients in valacyclovir tablets? Active Ingredient: valacyclovir hydrochloride Inactive Ingredients: hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol and titanium dioxide. The white, film-coated tablets are printed with edible black ink which contains black iron oxide, propylene glycol and shellac glaze.
Manufactured for: Mylan Pharmaceuticals Inc., Morgantown, WV 26505 U.S.A. Manufactured by: Mylan Laboratories Limited, Hyderabad — 500 096, India |
|
This Patient Information has been approved by the U.S. Food and Drug Administration.
For more information, call Mylan at 1-877-446-3679 (1-877-INFO-RX).
Manufactured for:
Mylan Pharmaceuticals Inc.
Morgantown, WV 26505 U.S.A.
Manufactured by:
Mylan Laboratories Limited
Hyderabad — 500 096, India
75095095
Revised: 12/2022
MX:VLCY:R11pt/MX:PL:VLCY:R7pt
PRINCIPAL DISPLAY PANEL – 500 mg
NDC 0378-4275-93
Valacyclovir
Tablets, USP
500 mg
Rx only 30 Tablets
Each film-coated tablet contains 500 mg
of valacyclovir, on the anhydrous basis,
equivalent to 556.2 mg of valacyclovir
hydrochloride, USP (hydrous) per tablet.
Usual Dosage: See accompanying
prescribing information.
Keep this and all medication out of
the reach of children.
Store at 20° to 25°C (68° to 77°F). [See
USP Controlled Room Temperature.]
Do not use if safety seal under cap is
broken or missing.
Manufactured for:
Mylan Pharmaceuticals Inc.
Morgantown, WV 26505 U.S.A.
Made in India
Mylan.com
RMX4275H8
Dispense in a tight, light-resistant
container as defined in the USP
using a child-resistant closure.
Keep container tightly closed.
Code No.: MH/DRUGS/25/NKD/89

PRINCIPAL DISPLAY PANEL – 1 g
NDC 0378-4276-93
Valacyclovir
Tablets, USP
1 gram
Rx only 30 Tablets
Each film-coated tablet contains 1 gram
of valacyclovir, on the anhydrous basis,
equivalent to 1.112 grams of valacyclovir
hydrochloride, USP (hydrous) per tablet.
Usual Dosage: See accompanying
prescribing information.
Keep this and all medication out of
the reach of children.
Store at 20° to 25°C (68° to 77°F). [See
USP Controlled Room Temperature.]
Do not use if safety seal under cap is
broken or missing.
Manufactured for:
Mylan Pharmaceuticals Inc.
Morgantown, WV 26505 U.S.A.
Made in India
Mylan.com
RMX4276H8
Dispense in a tight, light-resistant
container as defined in the USP
using a child-resistant closure.
Keep container tightly closed.
Code No.: MH/DRUGS/25/NKD/89
| VALACYCLOVIR HYDROCHLORIDE
valacyclovir tablet, film coated |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| VALACYCLOVIR HYDROCHLORIDE
valacyclovir tablet, film coated |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Mylan Pharmaceuticals Inc. (059295980) |