HEPATASOL- leucine, isoleucine, valine, lysine acetate, threonine, methionine, phenylalanine, tryptophan, glycine, proline, alanine, arginine, serine, histidine and cysteine hydrochloride injection
Baxter Healthcare Corporation
----------
8% HEPATASOL - sulfite-free (Amino Acid) Injection
in VIAFLEX Plastic Container
Protect from light until use.
Rx Only
DESCRIPTION
8% HEPATASOL - sulfite-free (Amino Acid) Injection is a sterile, nonpyrogenic, hypertonic solution containing crystalline amino acids.
The VIAFLEX plastic container is fabricated from a specially formulated polyvinyl chloride (PL 146 Plastic). Exposure to temperatures above 25ºC/77ºF during transport and storage will lead to minor losses in moisture content. Higher temperatures lead to greater losses. It is unlikely that these minor losses will lead to clinically significant changes within the expiration period. The amount of water that can permeate from inside the container into the overwrap is insufficient to affect the solution significantly. Solutions in contact with the plastic container can leach out certain of its chemical components in very small amounts within the expiration period (e.g., di-2-ethylhexyl phthalate, DEHP, at not more than 0.2 part per million); however, the safety of the plastic has been confirmed in tests in animals according to USP biological tests for plastic containers as well as by tissue culture toxicity studies.
Intravenous fat emulsion should not be administered in polyvinyl chloride (PVC) containers that use di-2-ethylhexyl phthalate (DEHP) as a plasticizer, because the fat emulsion facilitates the leaching of DEHP from these containers.
| Each 100 mL contains: | |
| Amino Acids | 8 g |
| Total Nitrogen | 1.22 g |
| Essential Amino Acids | |
| Leucine - (CH3)2 CHCH2CH (NH2) COOH | 1.10 g |
| Isoleucine - CH3CH2CH (CH3) CH (NH2) COOH | 0.90 g |
| Valine - (CH3)2 CHCH (NH2) COOH | 0.84 g |
| Lysine - (added as lysine acetate) H2N (CH2)4 CH (NH2) COOH | 0.61 g |
| Threonine - CH3CH (OH) CH (NH2) COOH | 0.45 g |
| Methionine - CH3S (CH2)2 CH (NH2) COOH | 0.10 g |
| Phenylalanine - (C6H5) CH2 CH (NH2) COOH | 0.10 g |
| Tryptophan - (C8H6N) CH2 CH (NH2) COOH | 0.066 g |
| Nonessential Amino Acids | |
| Glycine - H2NCH2COOH | 0.90 g |
| Proline - [(CH2)3 NH CH] COOH | 0.80 g |
| Alanine – CH3CH (NH2) COOH | 0.77 g |
| Arginine - H2NC (NH) NH (CH2)3 CH (NH2) COOH | 0.60 g |
| Serine - HOCH2CH (NH2) COOH | 0.50 g |
| Histidine - (C3H3N2) CH2CH (NH2) COOH | 0.24 g |
| Cysteine Hydrochloride Monohydrate - [SHCH2 CHNH2 COOH]•HCl•H2O | less than 0.020 g |
| Phosphoric Acid NF | 0.115 g |
| pH (pH adjusted with glacial acetic acid) | 6.5 (6.0 to 6.8) |
| Electrolyte profile mEq per liter* | |
| Chloride less than 3, Phosphate (as HPO4=) 20 (10 mmoles/Liter), Acetate 68 (provided as glacial acetic acid and lysine acetate). | |
| *Balanced by ions from amino acids. | |
| Osmolarity (Calc.) | 775 mOsmol/L |
CLINICAL PHARMACOLOGY
8% HEPATASOL - sulfite-free (Amino Acid) Injection provides a mixture of essential and nonessential amino acids with high concentrations of the branched chain amino acids isoleucine, leucine, and valine, and low concentrations of methionine and the aromatic amino acids phenylalanine and tryptophan, relative to general purpose amino acid injections. This amino acid composition has been specifically formulated to provide a well tolerated nitrogen source for nutritional support and therapy of patients with liver disease who have hepatic encephalopathy.
The precise mechanisms which produce the therapeutic effects of this amino acid formulation are not known, The etiopathology of hepatic encephalopathy is also unknown and is thought to be of multifactorial origin. The rationale for this amino acid formulation is based on observations of plasma amino acid imbalances in patients with liver disease and on theories which postulate that these abnormal patterns are causally related to the development of hepatic encephalopathy.
Clinical studies in patients with hepatic encephalopathy showed that the infusion of this amino acid formulation reversed the abnormal plasma amino acid pattern characterized by decreased levels of branched chain amino acids and elevated levels of aromatic amino acids and methionine. The trend toward normalization of these amino acids was generally associated with an improvement in mental status and EEG patterns. This clinical response was observed in the majority of patients studied. Nitrogen balance was significantly improved and mortality reduced in these typically protein-intolerant patients who received substantial amounts of protein equivalent as this amino acid injection.
When infused with hypertonic dextrose as a calorie source, supplemented with electrolytes, vitamins, and minerals, this amino acid formulation provides total parenteral nutrition in patients with liver disease, with the exception of essential fatty acids.
Phosphate is a major intracellular anion which participates in providing energy for metabolism of substrates and contributes to significant metabolic and enzymatic reactions in all organs and tissues. It exerts a modifying influence on calcium levels, a buffering effect on acid-base equilibrium, and has a primary role in the renal excretion of hydrogen ions.
It is thought that the acetate from lysine acetate and acetic acid, under the conditions of parenteral nutrition, does not impact net acid-base balance when renal and respiratory functions are normal. Clinical evidence seems to support this thinking; however, confirmatory experimental evidence is not available.
The amount of chloride present is not of clinical significance.
INDICATIONS AND USAGE
8% HEPATASOL - sulfite-free (Amino Acid) Injection is indicated for the treatment of hepatic encephalopathy in patients with cirrhosis or hepatitis. 8% HEPATASOL - sulfite-free (Amino Acid) Injection provides nutritional support for patients with these diseases of the liver who require parenteral nutrition and are intolerant of general purpose amino acid injections, which are contraindicated in patients with hepatic coma.
CONTRAINDICATIONS
8% HEPATASOL - sulfite-free (Amino Acid) Injection is contraindicated in patients with anuria, inborn errors of amino acid metabolism, especially those involving branched chain amino acid metabolism such as Maple Syrup Urine Disease and Isovaleric Acidemia, or hypersensitivity to one or more amino acids present in the solution.
WARNINGS
Additives may be incompatible. Consult with pharmacist, if available. When introducing additives, use aseptic techniques. Mix thoroughly. Do not store.
Because of the potential for life-threatening events, caution should be taken to ensure that precipitates have not formed in any parenteral nutrient admixture.
Safe, effective use of parenteral nutrition requires a knowledge of nutrition as well as clinical expertise in recognition and treatment of the complications which can occur. Frequent evaluations and laboratory determinations are necessary for proper monitoring of parenteral nutrition. Studies should include blood sugar, serum proteins, kidney and liver function tests, electrolytes, hemogram, carbon dioxide content, serum osmolarities, blood cultures, and blood ammonia levels.
Administration of amino acids in the presence of impaired renal function or gastrointestinal bleeding may augment an already elevated blood urea nitrogen. Patients with azotemia from any cause should not be infused with amino acids without regard to total nitrogen intake.
Administration of intravenous solutions can cause fluid and/or solute overload resulting in dilution of serum electrolyte concentrations, over-hydration, congested states, or pulmonary edema. The risk of dilutional states is inversely proportional to the electrolyte concentrations of the solutions. The risk of solute overload causing congested states with peripheral and pulmonary edema is directly proportional to the electrolyte concentrations of the solutions.
WARNING: This product contains aluminum that may be toxic. Aluminum may reach toxic levels with prolonged parenteral administration if kidney function is impaired. Premature neonates are particularly at risk because their kidneys are immature, and they require large amounts of calcium and phosphate solutions, which contain aluminum.
Research indicates that patients with impaired kidney function, including premature neonates, who receive parenteral levels of aluminum at greater than 4 to 5 μg/kg/day accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration.
PRECAUTIONS
General
Clinical evaluation and periodic laboratory determinations are necessary to monitor changes in fluid balance, electrolyte concentrations, and acid-base balance during prolonged parenteral therapy or whenever the condition of the patient warrants such evaluation. Significant deviations from normal concentrations may require the use of additional electrolyte supplements.
Strongly hypertonic nutrient solutions should be administered through an indwelling intravenous catheter with the tip located in the superior vena cava.
Special care must be taken when giving hypertonic dextrose to a diabetic or prediabetic patient. To prevent severe hyperglycemia in such patients, insulin may be required.
Peripheral intravenous administration of 8% HEPATASOL - sulfite-free (Amino Acid) Injection requires appropriate dilution and provision of adequate calories. Care should be taken to assure proper placement of the needle within the lumen of the vein. The venipuncture site should be inspected frequently for signs of infiltration. If venous thrombosis or phlebitis occurs, discontinue infusions or change infusion site and initiate appropriate treatment.
Care should be taken to avoid circulatory overload, particularly in patients with cardiac insufficiency.
In patients with myocardial infarct, infusion of amino acids should always be accompanied by dextrose since in anoxia, free fatty acids cannot be utilized by the myocardium and energy must be produced anaerobically from glycogen or glucose.
Infusion of this amino acid formulation may not affect the clinical course of patients with fulminant hepatitis who have a poor prognosis and are generally unresponsive to treatment. It has been shown that the abnormal plasma amino acid pattern in fulminant hepatitis differs from that in chronic liver disease.
Extraordinary electrolyte losses such as may occur during protracted nasogastric suction, vomiting, diarrhea, or gastrointestinal fistula drainage may necessitate additional electrolyte supplementation.
Administration of glucose at a rate exceeding the patient's utilization rate may lead to hyperglycemia, coma, and death.
Metabolic acidosis can be prevented or readily controlled by adding a portion of the cations in the electrolyte mixture as acetate salts and in the case of hyperchloremic acidosis, by keeping the total chloride content of the infusate to a minimum.
8% HEPATASOL - sulfite-free (Amino Acid) Injection contains less than 3 mEq chloride per liter.
8% HEPATASOL - sulfite-free (Amino Acid) Injection contains 10 mmoles/Liter of phosphate. Some patients, especially those with hypophosphatemia, may require additional phosphate. To prevent hypocalcemia, calcium supplementation should always accompany phosphate administration. To assure adequate intake, serum levels should be monitored frequently.
8% HEPATASOL - sulfite-free (Amino Acid) Injection has not been adequately studied in pregnant women and children therefore, its safe use in such patients has not been demonstrated.
To minimize the risk of possible incompatibilities arising from mixing this solution with other additives that may be prescribed, the final infusate should be inspected for cloudiness or precipitation immediately after mixing, prior to administration, and periodically during administration.
Use 8% HEPATASOL - sulfite-free (Amino Acid) Injection only if solution is clear, and the seal is intact.
Drug product contains no more than 25 μg/L of aluminum.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies with 8% HEPATASOL - sulfite-free (Amino Acid) have not been performed to evaluate carcinogenic potential, mutagenic potential, or effects on fertility.
Pregnancy:
Teratogenic Effects
Pregnancy Category C.
Animal reproduction studies have not been conducted with 8% HEPATASOL - sulfite-free (Amino Acid) Injection. It is also not known whether 8% HEPATASOL - sulfite-free (Amino Acid) Injection can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. 8% HEPATASOL - sulfite-free (Amino Acid) Injection should be given to a pregnant woman only if clearly needed.
Nursing Mothers:
Caution should be exercised when 8% HEPATASOL - sulfite-free (Amino Acid) Injection is administered to a nursing woman.
Pediatric Use:
Safety and effectiveness of 8% HEPATASOL - sulfite-free (Amino Acid) Injection in pediatric patients have not been established by adequate and well-controlled studies. However, the use of amino acid injections in pediatric patients as an adjunct in the offsetting of nitrogen loss or in the treatment of negative nitrogen balance is referenced in the medical literature. See DOSAGE AND ADMINISTRATION.
Special Precautions for Central Venous Nutrition
Administration by central venous catheter should be used only by those familiar with this technique and its complications.
Central venous nutrition may be associated with complications which can be prevented or minimized by careful attention to all aspects of the procedure, including solution preparation, administration, and patient monitoring. It is essential that a carefully prepared protocol, based on current medical practices, be followed, preferably by an experienced team.
Although a detailed discussion of the complications is beyond the scope of this insert, the following summary lists those based on current literature.
Technical.
The placement of a central venous catheter should be regarded as a surgical procedure. One should be fully acquainted with various techniques of catheter insertion as well as recognition and treatment of complications. For details of techniques and placement sites, consult the medical literature. X-ray is the best means of verifying catheter placement. Complications known to occur from the placement of central venous catheters are pneumothorax, hemothorax, hydrothorax, artery puncture and transection, injury to the brachial plexus, malposition of the catheter, formation of arterio-venous fistula, phlebitis, thrombosis, pericardial tamponade, and air and catheter embolus.
Septic.
The constant risk of sepsis is present during total parenteral nutrition. Since contaminated solutions and infusion catheters are potential sources of infection, it is imperative that the preparation of solutions and the placement and care of catheters be accomplished under controlled aseptic conditions.
Solutions should ideally be prepared in the hospital pharmacy in a laminar flow hood. The key factor in their preparation is careful aseptic technique to avoid inadvertent touch contamination during mixing of solutions and subsequent admixtures.
Solutions should be used promptly after mixing. Any storage should be under refrigeration for as brief a time as possible. Administration time for a single container and set should never exceed 24 hours.
Consult the medical literature for a discussion of the management of sepsis. In brief, typical management includes replacing the solution being administered with a fresh container and set, and culturing the contents for bacterial or fungal contamination. It sepsis persists and another source of infection is not identified, the catheter is removed, the proximal tip cultured, and a new catheter reinserted when the fever has subsided. Non-specific, prophylactic antibiotic treatment is not recommended.
Clinical experience indicates that the catheter is likely to be the prime source of infection as opposed to aseptically prepared and properly stored solutions.
Metabolic.
The following metabolic complications have been reported during the use of central venous nutrition: metabolic acidosis, hypophosphatemia, alkalosis, hyperglycemia and glycosuria, osmotic diuresis and dehydration, rebound hypoglycemia, elevated liver enzymes, hypo- and hyper- vitaminosis, electrolyte imbalances and hyperammonemia in children. Frequent clinical evaluation and laboratory determinations are necessary, especially during the first few days of therapy to prevent or minimize these complications.
ADVERSE REACTIONS
See WARNINGS, and Special Precautions for Central Venous Nutrition.
Reactions reported in clinical studies as a result of infusion of the parenteral fluid were water weight gain, edema, increase in BUN, and dilutional hyponatremia. Asterixis was reported to have worsened in one patient during infusion of this amino acid formulation.
Reactions which may occur because of the solution or the technique of administration include febrile response, infection at the site of injection, venous thrombosis or phlebitis extending from the site of injection, extravasation and hypervolemia.
Symptoms may result from an excess or deficit of one or more of the ions present in the solution; therefore, frequent monitoring of electrolyte levels is essential.
Phosphorus deficiency may lead to impaired tissue oxygenation and acute hemolytic anemia. Relative to calcium, excessive phosphorus intake can precipitate hypocalcemia with cramps, tetany and muscular hyperexcitability.
If an adverse reaction does occur, discontinue the infusion, evaluate the patient, institute appropriate therapeutic countermeasures and save the remainder of the fluid for examination if deemed necessary.
OVERDOSAGE
In the event of a fluid or solute overload during parenteral therapy, re-evaluate the patient’s condition, and institute appropriate corrective treatment.
DOSAGE AND ADMINISTRATION
The objective of nutritional management of patients with liver disease is the provision of sufficient amino acid and caloric support for protein synthesis without exacerbating hepatic encephalopathy.
The total daily dose of 8% HEPATASOL - sulfite-free (Amino Acid) Injection depends on daily protein requirements and on the patient’s metabolic and clinical response. The determination of nitrogen balance and accurate daily body weights, corrected for fluid balance, are probably the best means of assessing individual protein requirements. Dosage should also be guided by the patient’s fluid intake limits and glucose and nitrogen tolerances, as well as by metabolic and clinical response.
The recommended dosage is 80-120 grams of amino acids (12-18 grams of nitrogen) as 8% HEPATASOL - sulfite-free (Amino Acid) Injection per day. Typically, 500 mL of 8% HEPATASOL - sulfite-free (Amino Acid) Injection appropriately mixed with 500 mL of 50% dextrose supplemented with electrolytes and vitamins is administered over an 8-12 hour period. This results in a total daily fluid intake of approximately 2-3 liters. Patients with fluid restrictions may only tolerate 1-2 liters. Although nitrogen requirements may be higher in severely hypercatabolic or depleted patients, provision of additional nitrogen may not be possible due to fluid intake limits, nitrogen, or glucose intolerance.
Pediatric Use:
Use of 8% HEPATASOL - sulfite-free (Amino Acid) Injection in pediatric patients is governed by the same considerations that affect the use of any amino acid solution in pediatrics. The amount administered is dosed on the basis of grams of amino acids/kg of body weight/day. Two to three g/kg of body weight for infants with adequate calories are generally sufficient to satisfy protein needs and promote positive nitrogen balance. Solutions administered by peripheral vein should not exceed twice normal serum osmolarity (718 mOsmol/L).
In many patients, provision of adequate calories in the form of hypertonic dextrose may require the administration of exogenous insulin to prevent hyperglycemia and glycosuria. To prevent rebound hypoglycemia, a solution containing 5% dextrose should be administered when hypertonic dextrose solutions are abruptly discontinued.
Fat emulsion coadministration should be considered when prolonged (more than 5 days) parenteral nutrition is required in order to prevent essential fatty acid deficiency (E.F.A.D.). Serum lipids should be monitored for evidence of E.F.A.D. in patients maintained on fat free TPN. Caution should be exercised in administering fat emulsions to patients with severe liver damage.
Fat emulsion may obscure the presence of precipitate formation.
The provision of sufficient intracellular electrolytes, principally potassium, magnesium, and phosphate, is required for optimum utilization of amino acids. Approximately 60-180 mEq of potassium, 10-30 mEq of magnesium, and 10-40 mmoles of phosphate per day appear necessary to achieve optimum metabolic response. In addition, sufficient quantities of the major extracellular electrolytes sodium, calcium, and chloride, must be given. In patients with hyperchloremic or other metabolic acidoses, sodium and potassium may be added as the acetate salts to provide bicarbonate precursor. The electrolyte content of 8% HEPATASOL - sulfite-free (Amino Acid) Injection must be considered when calculating daily electrolyte intake. Serum electrolytes, including magnesium and phosphorus, should be monitored frequently.
Hypertonic mixtures of amino acids and dextrose may be safely administered by continuous infusion through a central venous catheter with the tip located in the superior vena cava. Initial infusion rates should be slow, and gradually increased to the recommended 60-125 mL/hr. If administration rate should fall behind schedule, no attempt to “catch up" to planned intake should be made. In addition to meeting protein needs, the rate of administration, particularly during the first few days of therapy, is governed by the patient’s glucose tolerance. Daily intake of amino acids and dextrose should be increased gradually to the maximum required dose as indicated by frequent determinations of glucose levels in blood and urine.
For patients in whom the central venous route is not indicated and who can consume adequate calories enterally, 8% HEPATASOL - sulfite-free (Amino Acid) Injection may be administered by peripheral vein with or without parenteral carbohydrate calories. Such infusates can be prepared by dilution of 8% HEPATASOL - sulfite-free (Amino Acid) Injection with Sterile Water for injection or 5%-10% dextrose to prepare isotonic or slightly hypertonic solutions for peripheral infusion. It is essential that peripheral infusion be accompanied by adequate caloric supplementation. In pediatric patients, the final solution should not exceed twice normal serum osmolarity (718 mOsmol/L).
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
A slight yellow color does not alter the quality and efficacy of the product.
Care must be taken to avoid incompatible admixtures. Consult with pharmacist.
Intravenous fat emulsion should not be administered in polyvinyl chloride (PVC) containers that use di-2-ethylhexyl phthalate (DEHP) as a plasticizer, because the fat emulsion facilitates the leaching of DEHP from these containers.
HOW SUPPLIED
8% HEPATASOL - sulfite-free (Amino Acid) Injection is supplied sterile and nonpyrogenic in single dose VIAFLEX plastic containers packaged as follows:
| 2B6173 | 500 mL | NDC 0338-0504-03 |
Exposure of pharmaceutical products to heat should be minimized. Avoid excessive heat. Protect from freezing. It is recommended the product be stored at room temperature (25ºC/77ºF): brief exposure up to 40ºC/104ºF does not adversely affect the product.
Protect from light until use.
Do not remove container from overpouch until ready to use.
Do not use if overpouch has been previously opened or damaged.
PACKAGE LABEL - PRINCIPAL DISPLAY PANEL
Container Label
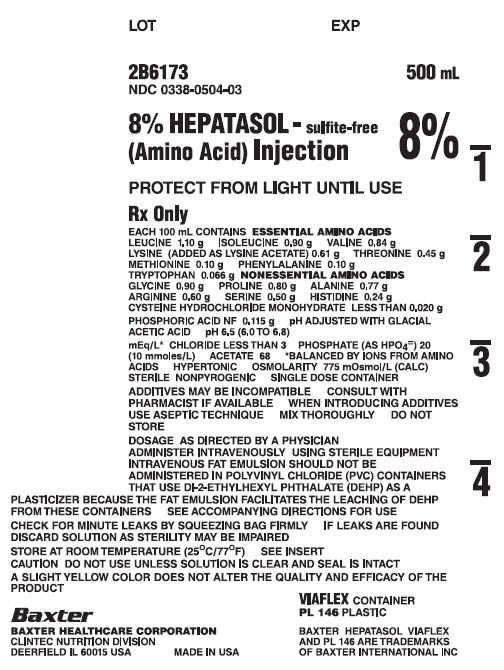
LOT
EXP
2B6173
NDC 0338-0504-03
500 mL
8% HEPATASOL - sulfite-free
(Amino Acid) Injection
PROTECT FROM LIGHT UNTIL USE
Rx Only
EACH 100 mL CONTAINS ESSENTIAL AMINO ACIDS
LEUCINE 1.10 g ISOLEUCINE 0.90 g VALINE 0.84 g
LYSINE (ADDED AS LYSINE ACETATE) 0.61 g THREONINE 0.45 g
METHIONINE 0.10 g PHENYLALANINE 0.10 g
TRYPTOPHAN 0.066 g NONESSENTIAL AMINO ACIDS
GLYCINE 0.90 g PROLINE 0.80 g ALANINE 0.77 g
ARGININE 0.60 g SERINE 0.50 G HISTIDINE 0.24 g
CYSTEINE HYDROCHLORIDE MONOHYDRATE LESS THAN 0.020 g
PHOSPHORIC ACID NF 0.115 g pH ADJUSTED WITH GLACIAL
ACETIC ACID pH 6.5 (6.0 TO 6.8)
mEq/L* CHLORIDE LES THAN 3 PHOSPHATE (AS HPO4=) 20
(10 mmoles/L) ACETATE 68 *BALANCED BY IONS FROM AMINO
ACIDS HYPERTONIC OSMOLARITY 775 mOsmol/L (CALC)
STERILE NONPYROGENIC SINGLE DOSE CONTAINER
ADDITIVES MAY BE IMCOMPATIBLE CONSULT WITH
PHARMACIST IF AVAILABLE WHEN INTRODUCING ADDITIVES
USE ASEPTIC TECHNIQUE MIX THOROUGHLY DO NOT
STORE
DOSAGE AS DIRECTED BY A PHYSICIAN
ADMINISTER INTRAVENOUSLY USING STERILE EQUIPMENT
INTRAVENOUS FAT EMULSION SHOULD NOT BE
ADMINISTERED IN POLYVINYL CHLORIDE (PVC) CONTAINERS
THAT USE DI-2-ETHYLHEXYL PHTHALATE (DEHP) AS A
PLASTICIZER BECAUSE THE FAT EMULSION FACILITATES THE LEACHING OF DEHP
FROM THESE CONTAINERS SEE ACCOMPANYING DIRECTIONS FOR USE
CHECK FOR MINUTE LEAKS BY SQUEEZING BAG FIRMLY IF LEAKS ARE FOUND
DISCARD SOLUTION AS STERILITY MAY BE IMPAIRED
STORE AT ROOM TEMPERATURE (25ºC/77ºF) SEE INSERT
CAUTION DO NOT USE UNLESS SOLUTION IS CLEAR AND SEAL IS INTACT
A SLIGHT YELLOW COLOR DOES NOT ALTER THE QUALITY AND EFFICACY OF THE PRODUCT
VIAFLEX CONTAINER
PL 146 PLASTIC
BAXTER HEPATASOL VIAFLEX
AND PL 146 ARE TRADEMARKS
OF BAXTER INTERNATIONAL INC
Baxter
BAXTER HEALTHCARE CORPORATION
CLINTEC NUTRITION DIVISION
DEERFIELD IL 60015 USA
MADE IN USA
Carton Label
Lot: x
QTY: 24-500 mL
Exp: x x
Code: 2B6173
NDC: 0338-0504-03
8% Hepatasol Sulfite-Free (Amino Acid) INJ
Viaflex Container
(17) XX00 (10) x
(01) 50303380504034
| HEPATASOL
leucine, isoleucine, valine, lysine acetate, threonine, methionine, phenylalanine, tryptophan, glycine, proline, alanine, arginine, serine, histidine and cysteine hydrochloride injection |
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
| Labeler - Baxter Healthcare Corporation (005083209) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Baxter Healthcare Corporation | 189326168 | ANALYSIS(0338-0504), MANUFACTURE(0338-0504), LABEL(0338-0504), PACK(0338-0504), STERILIZE(0338-0504) | |