ASPIRIN AND DIPYRIDAMOLE- aspirin and dipyridamole capsule, extended release
Impax Generics
----------
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ASPIRIN and EXTENDED-RELEASE DIPYRIDAMOLE CAPSULES safely and effectively. See full prescribing information for ASPIRIN and EXTENDED-RELEASE DIPYRIDAMOLE CAPSULES.
ASPIRIN and extended-release DIPYRIDAMOLE capsules, for oral use Initial U.S. Approval: 1999 INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONSWARNINGS AND PRECAUTIONSADVERSE REACTIONS
To report SUSPECTED ADVERSE REACTIONS, contact Impax Laboratories, Inc. at 1-800-934-6729 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. DRUG INTERACTIONSUSE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling. Revised: 3/2019 |
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
Aspirin and extended-release dipyridamole capsules are indicated to reduce the risk of stroke in patients who have had transient ischemia of the brain or completed ischemic stroke due to thrombosis.
2 DOSAGE AND ADMINISTRATION
Aspirin and extended-release dipyridamole capsules are not interchangeable with the individual components of aspirin and dipyridamole tablets.
The recommended dose of aspirin and extended-release dipyridamole capsules is one capsule given orally twice daily, one in the morning and one in the evening. Swallow capsules whole without chewing. Aspirin and extended-release dipyridamole capsules can be administered with or without food.
2.1 Alternative Regimen in Case of Intolerable Headaches
In the event of intolerable headaches during initial treatment, switch to one capsule at bedtime and low-dose aspirin in the morning. Because there are no outcome data with this regimen and headaches become less of a problem as treatment continues, patients should return to the usual regimen as soon as possible, usually within one week.
3 DOSAGE FORMS AND STRENGTHS
25 mg/200 mg capsules with a white cap and body, containing yellow extended-release pellets incorporating dipyridamole, USP and a round, white, film-coated tablet incorporating immediate-release aspirin, USP. The capsule is imprinted with  and 2510 on both cap and body in black ink.
and 2510 on both cap and body in black ink.
4 CONTRAINDICATIONS
4.1 Hypersensitivity
Aspirin and extended-release dipyridamole capsules are contraindicated in patients with known hypersensitivity to any of the product components.
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Bleeding
Aspirin and extended-release dipyridamole capsules increase the risk of bleeding. Risk factors for bleeding include the use of other drugs that increase the risk of bleeding (e.g., anticoagulants, antiplatelet agents, heparin, anagrelide, fibrinolytic therapy, and chronic use of NSAIDs) [see Drug Interactions (7.1)].
Intracranial Hemorrhage
In European Stroke Prevention Study-2 (ESPS2), the incidence of intracranial hemorrhage was 0.6% in the aspirin and extended-release dipyridamole capsule group, 0.5% in the extended-release dipyridamole (ER-DP) group, 0.4% in the aspirin (ASA) group and 0.4% in the placebo groups.
Gastrointestinal (GI) Side Effects
GI side effects include stomach pain, heartburn, nausea, vomiting, and gross GI bleeding. Although minor upper GI symptoms, such as dyspepsia, are common and can occur anytime during therapy, physicians should remain alert for signs of ulceration and bleeding, even in the absence of previous GI symptoms. Inform patients about the signs and symptoms of GI side effects and what steps to take if they occur.
In ESPS2, the incidence of gastrointestinal bleeding was 4.1% in the aspirin and extended-release dipyridamole capsule group, 2.2% in the extended-release dipyridamole group, 3.2% in the aspirin group, and 2.1% in the placebo groups.
Peptic Ulcer Disease
Avoid using aspirin in patients with a history of active peptic ulcer disease, which can cause gastric mucosal irritation and bleeding.
Alcohol Warning
Because aspirin and extended-release dipyridamole capsules contain aspirin, counsel patients who consume three or more alcoholic drinks every day about the bleeding risks involved with chronic, heavy alcohol use while taking aspirin.
5.2 Renal Failure
Avoid aspirin in patients with severe renal failure (glomerular filtration rate less than 10 mL/minute) [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].
5.3 Hepatic Insufficiency
Elevations of hepatic enzymes and hepatic failure have been reported in association with dipyridamole administration [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].
5.4 Pregnancy
Because aspirin and extended-release dipyridamole capsules contain aspirin, aspirin and extended-release dipyridamole capsules can cause fetal harm when administered to a pregnant woman. Maternal aspirin use during later stages of pregnancy may cause low birth weight, increased incidence for intracranial hemorrhage in premature infants, stillbirths and neonatal death. Because of the above and because of the known effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on the fetal cardiovascular system (closure of the ductus arteriosus), avoid aspirin and extended-release dipyridamole capsules in the third trimester of pregnancy [see Use in Specific Populations (8.1)].
Aspirin has been shown to be teratogenic in rats (spina bifida, exencephaly, microphthalmia and coelosomia) and rabbits (congested fetuses, agenesis of skull and upper jaw, generalized edema with malformation of the head, and diaphanous skin) at oral doses of 330 mg/kg/day and 110 mg/kg/day, respectively. These doses, which also resulted in a high resorption rate in rats (63% of implantations versus 5% in controls), are, on a mg/m2 basis, about 66 and 44 times, respectively, the dose of aspirin contained in the maximum recommended daily human dose of aspirin and extended-release dipyridamole capsules. Reproduction studies with dipyridamole have been performed in mice, rabbits and rats at oral doses of up to 125 mg/kg, 40 mg/kg and 1000 mg/kg, respectively (about 1½, 2 and 25 times the maximum recommended daily human oral dose, respectively, on a mg/m2 basis) and have revealed no evidence of harm to the fetus due to dipyridamole. When 330 mg aspirin/kg/day was combined with 75 mg dipyridamole/kg/day in the rat, the resorption rate approached 100%, indicating potentiation of aspirin-related fetal toxicity. There are no adequate and well-controlled studies of the use of aspirin and extended-release dipyridamole capsules in pregnant women. If aspirin and extended-release dipyridamole capsules are used during pregnancy, or if the patient becomes pregnant while taking aspirin and extended-release dipyridamole capsules, inform the patient of the potential hazard to the fetus.
5.5 Coronary Artery Disease
Dipyridamole has a vasodilatory effect. Chest pain may be precipitated or aggravated in patients with underlying coronary artery disease who are receiving dipyridamole.
For stroke or TIA patients for whom aspirin is indicated to prevent recurrent myocardial infarction (MI) or angina pectoris, the aspirin in this product may not provide adequate treatment for the cardiac indications.
6 ADVERSE REACTIONS
The following adverse reactions are discussed elsewhere in the labeling:
- Hypersensitivity [seeContraindications (4.1)]
- Allergy [see Contraindications (4.2)]
- Risk of Bleeding [see Warnings and Precautions (5.1)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The efficacy and safety of aspirin and extended-release dipyridamole capsules were established in the European Stroke Prevention Study-2 (ESPS2). ESPS2 was a double-blind, placebo-controlled study that evaluated 6602 patients over the age of 18 years who had a previous ischemic stroke or transient ischemic attack within ninety days prior to entry. Patients were randomized to either aspirin and extended-release dipyridamole capsules, aspirin, ER-DP, or placebo [see Clinical Studies (14)]; primary endpoints included stroke (fatal or nonfatal) and death from all causes.
This 24-month, multicenter, double-blind, randomized study (ESPS2) was conducted to compare the efficacy and safety of aspirin and extended-release dipyridamole capsules with placebo, extended-release dipyridamole alone and aspirin alone. The study was conducted in a total of 6602 male and female patients who had experienced a previous ischemic stroke or transient ischemia of the brain within three months prior to randomization.
Table 1 presents the incidence of adverse events that occurred in 1% or more of patients treated with aspirin and extended-release dipyridamole capsules where the incidence was also greater than in those patients treated with placebo. There is no clear benefit of the dipyridamole/aspirin combination over aspirin with respect to safety.
|
||||||||
| Individual Treatment Group | ||||||||
|
Body System/Preferred Term |
Aspirin and extended-release dipyridamole capsules | ER-DP Alone | ASA Alone |
Placebo |
||||
| Total Number of Patients | 1650 | 1654 | 1649 | 1649 |
||||
| Total Number (%) of Patients With at Least One On-Treatment Adverse Event
| 1319 | (80%) | 1305 | (79%) | 1323 | (80%) | 1304 | (79%) |
| Central and Peripheral Nervous System Disorders |
||||||||
| Headache | 647 | (39%) | 634 | (38%) | 558 | (34%) | 543 | (33%) |
| Convulsions | 28 | (2%) | 15 | (1%) | 28 | (2%) | 26 | (2%) |
| Gastrointestinal System Disorders |
||||||||
| Dyspepsia | 303 | (18%) | 288 | (17%) | 299 | (18%) | 275 | (17%) |
| Abdominal Pain | 289 | (18%) | 255 | (15%) | 262 | (16%) | 239 | (14%) |
| Nausea | 264 | (16%) | 254 | (15%) | 210 | (13%) | 232 | (14%) |
| Diarrhea | 210 | (13%) | 257 | (16%) | 112 | (7%) | 161 | (10%) |
| Vomiting | 138 | (8%) | 129 | (8%) | 101 | (6%) | 118 | (7%) |
| Hemorrhage Rectum | 26 | (2%) | 22 | (1%) | 16 | (1%) | 13 | (1%) |
| Melena | 31 | (2%) | 10 | (1%) | 20 | (1%) | 13 | (1%) |
| Hemorrhoids | 16 | (1%) | 13 | (1%) | 10 | (1%) | 10 | (1%) |
| GI Hemorrhage | 20 | (1%) | 5 | (0%) | 15 | (1%) | 7 | (0%) |
| Body as a Whole - General Disorders |
||||||||
| Pain | 105 | (6%) | 88 | (5%) | 103 | (6%) | 99 | (6%) |
| Fatigue | 95 | (6%) | 93 | (6%) | 97 | (6%) | 90 | (5%) |
| Back Pain | 76 | (5%) | 77 | (5%) | 74 | (4%) | 65 | (4%) |
| Accidental Injury | 42 | (3%) | 24 | (1%) | 51 | (3%) | 37 | (2%) |
| Malaise | 27 | (2%) | 23 | (1%) | 26 | (2%) | 22 | (1%) |
| Asthenia | 29 | (2%) | 19 | (1%) | 17 | (1%) | 18 | (1%) |
| Syncope | 17 | (1%) | 13 | (1%) | 16 | (1%) | 8 | (0%) |
| Psychiatric Disorders |
||||||||
| Amnesia | 39 | (2%) | 40 | (2%) | 57 | (3%) | 34 | (2%) |
| Confusion | 18 | (1%) | 9 | (1%) | 22 | (1%) | 15 | (1%) |
| Anorexia | 19 | (1%) | 17 | (1%) | 10 | (1%) | 15 | (1%) |
| Somnolence | 20 | (1%) | 13 | (1%) | 18 | (1%) | 9 | (1%) |
| Musculoskeletal System Disorders |
||||||||
| Arthralgia | 91 | (6%) | 75 | (5%) | 91 | (6%) | 76 | (5%) |
| Arthritis | 34 | (2%) | 25 | (2%) | 17 | (1%) | 19 | (1%) |
| Arthrosis | 18 | (1%) | 22 | (1%) | 13 | (1%) | 14 | (1%) |
| Vomiting | 138 | (8%) | 129 | (8%) | 101 | (6%) | 118 | (7%) |
| Myalgia | 20 | (1%) | 16 | (1%) | 11 | (1%) | 11 | (1%) |
| Respiratory System Disorders |
||||||||
| Coughing | 25 | (2%) | 18 | (1%) | 32 | (2%) | 21 | (1%) |
| Upper Respiratory Tract Infection | 16 | (1%) | 9 | (1%) | 16 | (1%) | 14 | (1%) |
| Cardiovascular Disorders, General |
||||||||
| Cardiac Failure | 26 | (2%) | 17 | (1%) | 30 | (2%) | 25 | (2%) |
| Platelet, Bleeding and Clotting Disorders |
||||||||
| Hemorrhage NOS | 52 | (3%) | 24 | (1%) | 46 | (3%) | 24 | (1%) |
| Epistaxis | 39 | (2%) | 16 | (1%) | 45 | (3%) | 25 | (2%) |
| Purpura | 23 | (1%) | 8 | (0%) | 9 | (1%) | 7 | (0%) |
| Neoplasm |
||||||||
| Neoplasm NOS | 28 | (2%) | 16 | (1%) | 23 | (1%) | 20 | (1%) |
| Red Blood Cell Disorders |
||||||||
| Anemia | 27 | (2%) | 16 | (1%) | 19 | (1%) | 9 | (1%) |
| Note: ER-DP = extended-release dipyridamole 200 mg; ASA = aspirin 25 mg. The dosage regimen for all treatment groups is BID. NOS = not otherwise specified. |
||||||||
Discontinuation due to adverse events in ESPS2 was 25% for aspirin and extended-release dipyridamole capsules, 25% for extended-release dipyridamole, 19% for aspirin, and 21% for placebo (refer to Table 2)
| Treatment Groups |
||||||||
| Aspirin and extended-release dipyridamole capsules | ER-DP | ASA | Placebo |
|||||
| Total Number of Patients | 1650 | 1654 | 1649 | 1649 |
||||
| Patients with at least one Adverse Event that led to treatment discontinuation | 417 | (25%) | 419 | (25%) | 318 | (19%) | 352 | (21%) |
| Headache | 165 | (10%) | 166 | (10%) | 57 | (3%) | 69 | (4%) |
| Dizziness | 85 | (5%) | 97 | (6%) | 69 | (4%) | 68 | (4%) |
| Nausea | 91 | (6%) | 95 | (6%) | 51 | (3%) | 53 | (3%) |
| Abdominal Pain | 74 | (4%) | 64 | (4%) | 56 | (3%) | 52 | (3%) |
| Dyspepsia | 59 | (4%) | 61 | (4%) | 49 | (3%) | 46 | (3%) |
| Vomiting | 53 | (3%) | 52 | (3%) | 28 | (2%) | 24 | (1%) |
| Diarrhea | 35 | (2%) | 41 | (2%) | 9 | (<1%) | 16 | (<1%) |
| Stroke | 39 | (2%) | 48 | (3%) | 57 | (3%) | 73 | (4%) |
| Transient Ischemic Attack | 35 | (2%) | 40 | (2%) | 26 | (2%) | 48 | (3%) |
| Angina Pectoris | 23 | (1%) | 20 | (1%) | 16 | (<1%) | 26 | (2%) |
| Note: ER-DP = extended-release dipyridamole 200 mg; ASA = aspirin 25 mg. The dosage regimen for all treatment groups is BID. |
||||||||
Headache was most notable in the first month of treatment.
Other Adverse Events
Adverse reactions that occurred in less than 1% of patients treated with aspirin and extended-release dipyridamole capsules in the ESPS2 study and that were medically judged to be possibly related to either dipyridamole or aspirin are listed below.
Body as a Whole: Allergic reaction, fever
Cardiovascular: Hypotension
Central Nervous System: Coma, dizziness, paresthesia, cerebral hemorrhage, intracranial hemorrhage, subarachnoid hemorrhage
Gastrointestinal: Gastritis, ulceration and perforation
Hearing and Vestibular Disorders: Tinnitus, and deafness. Patients with high frequency hearing loss may have difficulty perceiving tinnitus. In these patients, tinnitus cannot be used as a clinical indicator of salicylism
Heart Rate and Rhythm Disorders: Tachycardia, palpitation, arrhythmia, supraventricular tachycardia
Liver and Biliary System Disorders: Cholelithiasis, jaundice, hepatic function abnormal
Metabolic and Nutritional Disorders: Hyperglycemia, thirst
Platelet, Bleeding and Clotting Disorders: Hematoma, gingival bleeding
Psychiatric Disorders: Agitation
Reproductive: Uterine hemorrhage
Respiratory: Hyperpnea, asthma, bronchospasm, hemoptysis, pulmonary edema
Special Senses Other Disorders: Taste loss
Skin and Appendages Disorders: Pruritus, urticaria
Urogenital: Renal insufficiency and failure, hematuria
Vascular (Extracardiac) Disorders: Flushing
Laboratory Changes
Over the course of the 24-month study (ESPS2), patients treated with aspirin and extended-release dipyridamole capsules showed a decline (mean change from baseline) in hemoglobin of 0.25 g/dL, hematocrit of 0.75%, and erythrocyte count of 0.13x106/mm3.
6.2 Post-Marketing Experience
The following is a list of additional adverse reactions that have been reported either in the literature or are from postmarketing spontaneous reports for either dipyridamole or aspirin. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to estimate reliably their frequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labeling are typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency of reporting, or (3) strength of causal connection to aspirin and extended-release dipyridamole capsules.
Body as a Whole: Hypothermia, chest pain
Cardiovascular: Angina pectoris
Central Nervous System: Cerebral edema
Fluid and Electrolyte: Hyperkalemia, metabolic acidosis, respiratory alkalosis, hypokalemia
Gastrointestinal: Pancreatitis, Reye syndrome, hematemesis
Hearing and Vestibular Disorders: Hearing loss
Immune System Disorders: Hypersensitivity, acute anaphylaxis, laryngeal edema
Liver and Biliary System Disorders: Hepatitis, hepatic failure
Musculoskeletal: Rhabdomyolysis
Metabolic and Nutritional Disorders: Hypoglycemia, dehydration
Platelet, Bleeding and Clotting Disorders: Prolongation of the prothrombin time, disseminated intravascular coagulation, coagulopathy, thrombocytopenia
Reproductive: Prolonged pregnancy and labor, stillbirths, lower birth weight infants, antepartum and postpartum bleeding
Respiratory: Tachypnea, dyspnea
Skin and Appendages Disorders: Rash, alopecia, angioedema, Stevens-Johnson syndrome, skin hemorrhages such as bruising, ecchymosis, and hematoma
Urogenital: Interstitial nephritis, papillary necrosis, proteinuria
Vascular (Extracardiac) Disorders: Allergic vasculitis
Other Adverse Events: anorexia, aplastic anemia, migraine, pancytopenia, thrombocytosis.
7 DRUG INTERACTIONS
7.1 Drug Interaction Study Information Obtained From Literature
Adenosine
Dipyridamole has been reported to increase the plasma levels and cardiovascular effects of adenosine. Adjustment of adenosine dosage may be necessary.
Angiotensin Converting Enzyme (ACE) Inhibitors
Due to the indirect effect of aspirin on the renin-angiotensin conversion pathway, the hyponatremic and hypotensive effects of ACE inhibitors may be diminished by concomitant administration of aspirin.
Acetazolamide
Concurrent use of aspirin and acetazolamide can lead to high serum concentrations of acetazolamide (and toxicity) due to competition at the renal tubule for secretion.
Anticoagulants and Antiplatelets
Patients taking aspirin and extended-release dipyridamole capsules in combination with anticoagulants, antiplatelets, or any substance impacting coagulation are at increased risk for bleeding. Aspirin can displace warfarin from protein binding sites, leading to prolongation of both the prothrombin time and the bleeding time. Aspirin can increase the anticoagulant activity of heparin, increasing bleeding risk.
Anagrelide
Patients taking aspirin in combination with anagrelide are at an increased risk of bleeding.
Anticonvulsants
Salicylic acid can displace protein-bound phenytoin and valproic acid, leading to a decrease in the total concentration of phenytoin and an increase in serum valproic acid levels.
Beta Blockers
The hypotensive effects of beta blockers may be diminished by the concomitant administration of aspirin due to inhibition of renal prostaglandins, leading to decreased renal blood flow and salt and fluid retention.
Cholinesterase Inhibitors
Dipyridamole may counteract the anticholinesterase effect of cholinesterase inhibitors, thereby potentially aggravating myasthenia gravis.
Diuretics
The effectiveness of diuretics in patients with underlying renal or cardiovascular disease may be diminished by the concomitant administration of aspirin due to inhibition of renal prostaglandins, leading to decreased renal blood flow and salt and fluid retention.
Methotrexate
Salicylate can inhibit renal clearance of methotrexate, leading to bone marrow toxicity, especially in the elderly or renal impaired.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
The concurrent use of aspirin with other NSAIDs may increase bleeding or lead to decreased renal function.
Oral Hypoglycemics
Moderate doses of aspirin may increase the effectiveness of oral hypoglycemic drugs, leading to hypoglycemia.
Uricosuric Agents (probenecid and sulfinpyrazone)
Salicylates antagonize the uricosuric action of uricosuric agents.
8 USE IN SPECIFIC POPULATIONS
8.2 Labor and Delivery
Aspirin can result in excessive blood loss at delivery as well as prolonged gestation and prolonged labor. Because of these effects on the mother and because of adverse fetal effects seen with aspirin during the later stages of pregnancy [see Warnings and Precautions (5.4) ], avoid aspirin and extended-release dipyridamole capsules in the third trimester of pregnancy and during labor and delivery.
8.3 Nursing Mothers
Both dipyridamole and aspirin are excreted in human milk. Exercise caution when aspirin and extended-release dipyridamole capsules are administered to a nursing woman.
8.4 Pediatric Use
Safety and effectiveness of aspirin and extended-release dipyridamole capsules in pediatric patients have not been studied. Due to the aspirin component, use of this product in the pediatric population is not recommended [see Contraindications (4.3)].
8.5 Geriatric Use
Of the total number of subjects in ESPS2, 61 percent were 65 and over, while 27 percent were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out [see Clinical Pharmacology (12.3)].
8.6 Patients with Severe Hepatic or Severe Renal Dysfunction
Aspirin and extended-release dipyridamole capsules have not been studied in patients with hepatic or renal impairment. Avoid using aspirin containing products, such as aspirin and extended-release dipyridamole capsules in patients with severe hepatic or severe renal (glomerular filtration rate less than 10 mL/min) dysfunction [see Warnings and Precautions (5.2, 5.3) and Clinical Pharmacology (12.3)].
10 OVERDOSAGE
Because of the dose ratio of dipyridamole to aspirin, overdosage of aspirin and extended-release dipyridamole capsules are likely to be dominated by signs and symptoms of dipyridamole overdose. In case of real or suspected overdose, seek medical attention or contact a Poison Control Center immediately. Careful medical management is essential.
Based upon the known hemodynamic effects of dipyridamole, symptoms such as warm feeling, flushes, sweating, restlessness, feeling of weakness and dizziness may occur. A drop in blood pressure and tachycardia might also be observed.
Salicylate toxicity may result from acute ingestion (overdose) or chronic intoxication. Severity of aspirin intoxication is determined by measuring the blood salicylate level. The early signs of salicylic overdose (salicylism), including tinnitus (ringing in the ears), occur at plasma concentrations approaching 200 mcg/mL. In severe cases, hyperthermia and hypovolemia are the major immediate threats to life. Plasma concentrations of aspirin above 300 mcg/mL are clearly toxic. Severe toxic effects are associated with levels above 400 mcg/mL. A single lethal dose of aspirin in adults is not known with certainty but death may be expected at 30 g.
Treatment of overdose consists primarily of supporting vital functions, increasing drug elimination, and correcting acid-base disturbances. Consider gastric emptying and/or lavage as soon as possible after ingestion, even if the patient has vomited spontaneously. After lavage and/or emesis, administration of activated charcoal as a slurry may be beneficial if less than 3 hours have passed since ingestion. Charcoal absorption should not be employed prior to emesis and lavage. Follow acid-base status closely with serial blood gas and serum pH measurements. Maintain fluid and electrolyte balance. Administer replacement fluid intravenously and augment with correction of acidosis. Treatment may require the use of a vasopressor. Infusion of glucose may be required to control hypoglycemia.
Administration of xanthine derivatives (e.g., aminophylline) may reverse the hemodynamic effects of dipyridamole overdose. Plasma electrolytes and pH should be monitored serially to promote alkaline diuresis of salicylate if renal function is normal. In patients with renal insufficiency or in cases of life-threatening intoxication, dialysis is usually required to treat salicylic overdose; however, since dipyridamole is highly protein bound, dialysis is not likely to remove dipyridamole. Exchange transfusion may be indicated in infants and young children.
11 DESCRIPTION
Aspirin and extended-release dipyridamole capsules are a combination antiplatelet agent intended for oral administration. Each hard gelatin capsule contains 200 mg dipyridamole, USP in an extended-release form and 25 mg aspirin, USP, as an immediate-release film-coated tablet. In addition, each capsule contains the following inactive ingredients: colloidal silicon dioxide, corn starch, hydrolyzed methacrylic acid copolymer type C, gelatin, hydroxypropyl cellulose, hypromellose 2910, methacrylic acid copolymer type B, microcrystalline cellulose, polyethylene glycol 3350, polyvinyl alcohol, sodium bicarbonate, sodium lauryl sulfate, sodium starch glycolate type A, stearic acid, talc, tartaric acid, titanium dioxide, triacetin and triethyl citrate. The capsules are imprinted with black Tek-Print ink SW-9008 or black opacode S-1-17823 which contain black iron oxide, potassium hydroxide, propylene glycol and shellac.
Dipyridamole, USP
Dipyridamole, USP is an antiplatelet agent chemically described as 2,2',2'',2'''-[(4,8-Dipiperidinopyrimido[5,4-d]pyrimidine-2,6-diyl)dinitrilo]-tetraethanol. It has the following structural formula:
Dipyridamole, USP is an odorless yellow crystalline substance, having a bitter taste. It is soluble in dilute acids, methanol and chloroform, and is practically insoluble in water.
Aspirin, USP
The antiplatelet agent aspirin (acetylsalicylic acid) is chemically known as benzoic acid, 2- (acetyloxy)-, and has the following structural formula:
Aspirin, USP is an odorless white needle-like crystalline or powdery substance. When exposed to moisture, aspirin, USP hydrolyzes into salicylic and acetic acids, and gives off a vinegary odor. It is highly lipid soluble and slightly soluble in water.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The antithrombotic action of aspirin and extended-release dipyridamole capsules is the result of the additive antiplatelet effects of dipyridamole and aspirin.
Dipyridamole
Dipyridamole inhibits the uptake of adenosine into platelets, endothelial cells and erythrocytes in vitro and in vivo; the inhibition occurs in a dose-dependent manner at therapeutic concentrations (0.5 to 1.9 mcg/mL). This inhibition results in an increase in local concentrations of adenosine which acts on the platelet A2-receptor thereby stimulating platelet adenylate cyclase and increasing platelet cyclic-3',5'-adenosine monophosphate (cAMP) levels. Via this mechanism, platelet aggregation is inhibited in response to various stimuli such as platelet activating factor (PAF), collagen and adenosine diphosphate (ADP).
Dipyridamole inhibits phosphodiesterase (PDE) in various tissues. While the inhibition of cAMP-PDE is weak, therapeutic levels of dipyridamole inhibit cyclic-3',5'-guanosine monophosphate-PDE (cGMP-PDE), thereby augmenting the increase in cGMP produced by EDRF (endothelium-derived relaxing factor, now identified as nitric oxide).
Aspirin
Aspirin inhibits platelet aggregation by irreversible inhibition of platelet cyclooxygenase and thus inhibits the generation of thromboxane A2, a powerful inducer of platelet aggregation and vasoconstriction.
12.2 Pharmacodynamics
The effect of either agent on the other's inhibition of platelet reactivity has not been evaluated.
12.3 Pharmacokinetics
There are no significant interactions between aspirin and dipyridamole. The kinetics of the components are unchanged by their co-administration as aspirin and extended-release dipyridamole capsules.
Dipyridamole
Absorption
Peak plasma levels of dipyridamole are achieved 2 hours (range 1 to 6 hours) after administration of a daily dose of 400 mg aspirin and extended-release dipyridamole capsules (given as 200 mg BID). The peak plasma concentration at steady-state is 1.98 mcg/mL (1.01 to 3.99 mcg/mL) and the steady-state trough concentration is 0.53 mcg/mL (0.18 to 1.01 mcg/mL).
Effect of Food
When aspirin and extended-release dipyridamole capsules were taken with a high fat meal, dipyridamole peak plasma levels (Cmax) and total absorption (AUC) were decreased at steady-state by 20 to 30% compared to fasting. Due to the similar degree of inhibition of adenosine uptake at these plasma concentrations, this food effect is not considered clinically relevant.
Distribution
Dipyridamole is highly lipophilic (log P=3.71, pH=7); however, it has been shown that the drug does not cross the blood-brain barrier to any significant extent in animals. The steady-state volume of distribution of dipyridamole is about 92 L. Approximately 99% of dipyridamole is bound to plasma proteins, predominantly to alpha 1-acid glycoprotein and albumin.
Metabolism and Elimination
Dipyridamole is metabolized in the liver, primarily by conjugation with glucuronic acid, of which monoglucuronide which has low pharmacodynamic activity is the primary metabolite. In plasma, about 80% of the total amount is present as parent compound and 20% as monoglucuronide. Most of the glucuronide metabolite (about 95%) is excreted via bile into the feces, with some evidence of enterohepatic circulation. Renal excretion of parent compound is negligible and urinary excretion of the glucuronide metabolite is low (about 5%). With intravenous (i.v.) treatment of dipyridamole, a triphasic profile is obtained: a rapid alpha phase, with a half-life of about 3.4 minutes, a beta phase, with a half-life of about 39 minutes, (which, together with the alpha phase accounts for about 70% of the total area under the curve, AUC) and a prolonged elimination phase λz with a half-life of about 15.5 hours. Due to the extended absorption phase of the dipyridamole component, only the terminal phase is apparent from oral treatment with aspirin and extended-release dipyridamole capsules which, in Trial 9.123 was 13.6 hours.
Special Populations
Geriatric Patients: In ESPS2 [see Clinical Studies (14)], plasma concentrations (determined as AUC) of dipyridamole in healthy elderly subjects (greater than 65 years) were about 40% higher than in subjects younger than 55 years receiving treatment with aspirin and extended-release dipyridamole capsules.
Hepatic Dysfunction: No study has been conducted with aspirin and extended-release dipyridamole capsules in patients with hepatic dysfunction.
In a study conducted with an intravenous formulation of dipyridamole, patients with mild to severe hepatic insufficiency showed no change in plasma concentrations of dipyridamole but showed an increase in the pharmacologically inactive monoglucuronide metabolite. Dipyridamole can be dosed without restriction as long as there is no evidence of hepatic failure.
Renal Dysfunction: No study has been conducted with aspirin and extended-release dipyridamole capsules in patients with renal dysfunction.
In ESPS2 patients [see Clinical Studies (14)], with creatinine clearances ranging from about 15 mL/min to greater than 100 mL/min, no changes were observed in the pharmacokinetics of dipyridamole or its glucuronide metabolite if data were corrected for differences in age.
Aspirin
Absorption
Peak plasma levels of aspirin are achieved 0.63 hours (0.5 to 1 hour) after administration of a 50 mg aspirin daily dose from aspirin and extended-release dipyridamole capsules (given as 25 mg BID). The peak plasma concentration at steady-state is 319 ng/mL (175 to 463 ng/mL). Aspirin undergoes moderate hydrolysis to salicylic acid in the liver and the gastrointestinal wall, with 50% to 75% of an administered dose reaching the systemic circulation as intact aspirin.
Effect of Food
When aspirin and extended-release dipyridamole capsules were taken with a high fat meal, there was no difference for aspirin in AUC at steady-state, and the approximately 50% decrease in Cmax was not considered clinically relevant based on a similar degree of cyclooxygenase inhibition comparing the fed and fasted state.
Distribution
Aspirin is poorly bound to plasma proteins and its apparent volume of distribution is low (10 L). Its metabolite, salicylic acid, is highly bound to plasma proteins, but its binding is concentration-dependent (nonlinear). At low concentrations (less than 100 mcg/mL), approximately 90% of salicylic acid is bound to albumin. Salicylic acid is widely distributed to all tissues and fluids in the body, including the central nervous system, breast milk, and fetal tissues. Early signs of salicylate overdose (salicylism), including tinnitus (ringing in the ears), occur at plasma concentrations approximating 200 mcg/mL [see Adverse Reactions (6) and Overdosage (10)].
Metabolism and Elimination
Aspirin is rapidly hydrolyzed in plasma to salicylic acid, with a half-life of 20 minutes. Plasma levels of aspirin are essentially undetectable 2 to 2.5 hours after dosing and peak salicylic acid concentrations occur 1 hour (range: 0.5 to 2 hours) after administration of aspirin. Salicylic acid is primarily conjugated in the liver to form salicyluric acid, a phenolic glucuronide, an acyl glucuronide, and a number of minor metabolites. Salicylate metabolism is saturable and total body clearance decreases at higher serum concentrations due to the limited ability of the liver to form both salicyluric acid and phenolic glucuronide. Following toxic doses (10 to 20 g), the plasma half-life may be increased to over 20 hours.
The elimination of acetylsalicylic acid follows first-order kinetics with aspirin and extended-release dipyridamole capsules and has a half-life of 0.33 hours. The half-life of salicylic acid is 1.71 hours. Both values correspond well with data from the literature at lower doses which state a resultant half-life of approximately 2 to 3 hours. At higher doses, the elimination of salicylic acid follows zero-order kinetics (i.e., the rate of elimination is constant in relation to plasma concentration), with an apparent half-life of 6 hours or higher. Renal excretion of unchanged drug depends upon urinary pH. As urinary pH rises above 6.5, the renal clearance of free salicylate increases from less than 5% to greater than 80%. Alkalinization of the urine is a key concept in the management of salicylate overdose [see Overdosage (10)]. Following therapeutic doses, about 10% is excreted as salicylic acid and 75% as salicyluric acid, as the phenolic and acyl glucuronides, in urine.
Special Populations
Hepatic Dysfunction: Avoid aspirin in patients with severe hepatic insufficiency.
Renal Dysfunction: Avoid aspirin in patients with severe renal failure (glomerular filtration rate less than 10 mL/min).
Aspirin and extended-release dipyridamole capsules
Drug Interaction
A dedicated drug interaction study was conducted in 60 healthy volunteers to evaluate the effects of omeprazole 80 mg administered once daily on the pharmacokinetics (PK) of dipyridamole and the pharmacodynamics (PD) of acetylsalicylic acid when co-administered with aspirin and extended-release dipyridamole capsules twice daily. Dipyridamole exposure (Cmax and AUC) at steady-state were similar with or without omeprazole co-administration. The pharmacokinetics of acetylsalicylic acid was not characterized. However, the antiplatelet activity as measured by arachidonic acid induced platelet aggregation was similar between the treatment arms at steady-state.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In studies in which dipyridamole was administered in the feed to mice (up to 111 weeks in males and females) and rats (up to 128 weeks in males and up to 142 weeks in females), there was no evidence of drug-related carcinogenesis. The highest dose administered in these studies (75 mg/kg/day) was, on a mg/m2 basis, about equivalent to the maximum recommended daily human oral dose (MRHD) in mice and about twice the MRHD in rats.
Combinations of dipyridamole and aspirin (1:5 ratio) tested negative in the Ames test, in vivo chromosome aberration tests (in mice and hamsters), oral micronucleus tests (in mice and hamsters) and oral dominant lethal test (in mice). Aspirin, alone, induced chromosome aberrations in cultured human fibroblasts. Mutagenicity tests of dipyridamole alone with bacterial and mammalian cell systems were negative.
Combinations of dipyridamole and aspirin have not been evaluated for effects on fertility and reproductive performance. There was no evidence of impaired fertility when dipyridamole was administered to male and female rats at oral doses up to 500 mg/kg/day (about 12 times the MRHD on a mg/m2 basis). A significant reduction in number of corpora lutea with consequent reduction in implantations and live fetuses was, however, observed at 1250 mg/kg (more than 30 times the MRHD on a mg/m2 basis). Aspirin inhibits ovulation in rats.
14 CLINICAL STUDIES
ESPS2 (European Stroke Prevention Study-2) was a double-blind, placebo-controlled, 24-month study in which 6602 patients over the age of 18 years had an ischemic stroke (76%) or transient ischemic attack (TIA, 24%) within three months prior to entry. Patients were enrolled in 13 European countries between February 1989 and May 1995 and were randomized to one of four treatment groups: Aspirin and extended-release dipyridamole capsules 25 mg/200 mg; extended-release dipyridamole (ER-DP) 200 mg alone; aspirin (ASA) 25 mg alone; or placebo. The mean age in this population was 66.7 years with 58% of them being males. Patients received one capsule twice daily (morning and evening). Efficacy assessments included analyses of stroke (fatal or nonfatal) and death (from all causes) as confirmed by a blinded morbidity and mortality assessment group. There were no differences with regard to efficacy based on age or gender; patients who were older had a trend towards more events.
Stroke Endpoint
Aspirin and extended-release dipyridamole capsules reduced the risk of stroke by 22.1% compared to aspirin 50 mg/day alone (p = 0.008) and reduced the risk of stroke by 24.4% compared to extended-release dipyridamole 400 mg/day alone (p = 0.002) (Table 3). Aspirin and extended-release dipyridamole capsules reduced the risk of stroke by 36.8% compared to placebo (p <0.001).
| Total Number of Patients n | Number of Patients with Stroke within 2 years n (%) | Kaplan-Meier Estimate of Survival at 2 Years (95% C.I.) | Gehan-Wilcoxon TestP-value | Risk Reduction at 2 Years | Odds Ratio(95% C.I.) | |
| Individual Treatment Group |
||||||
| Aspirin and extended-release dipyridamole | 1650 | 157 (9.5%) | 89.9% (88.4%, 91.4%) | - | - | - |
| ER-DP | 1654 | 211 (12.8%) | 86.7% (85.0%, 88.4%) | - | - | - |
| ASA | 1649 | 206 (12.5%) | 87.1% (85.4%, 88.7%) | - | - | - |
| Placebo | 1649 | 250 (15.2%) | 84.1% (82.2%, 85.9%) | - | - | - |
| Pairwise Treatment Group Comparisons |
||||||
| Aspirin and extended-release dipyridamole vs. | - | - | - | 0.002* | 24.4% | 0.72 (0.58, 0.90) |
| ER-DP | ||||||
| Aspirin and extended-release dipyridamole vs. ASA | - | - | - | 0.008* | 22.1% | 0.74 (0.59, 0.92) |
| Aspirin and extended-release dipyridamole vs. Placebo | - | - | - | <0.001* | 36.8% | 0.59 (0.48, 0.73) |
| ER-DP vs. Placebo | - | - | - | 0.036† | 16.5% | 0.82 (0.67, 1.00) |
| ASA vs. Placebo | - | - | - | 0.009* | 18.9% | 0.80 (0.66, 0.97) |
| Note: ER-DP = extended-release dipyridamole 200 mg; ASA = aspirin 25 mg. The dosage regimen for all treatment groups is BID. |
||||||
ESPS2: Cumulative Stroke Rate (Fatal or Nonfatal) Over 24 months of Follow-Up
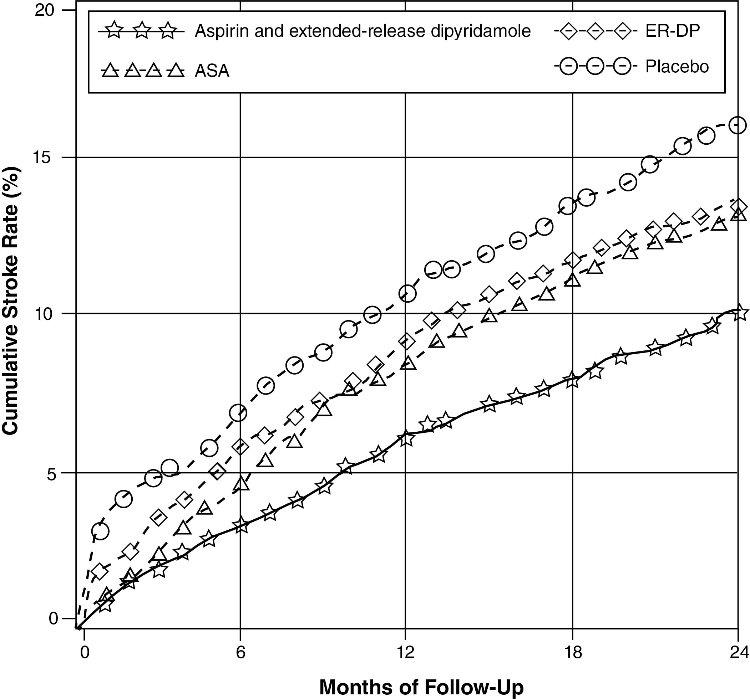
Note: ER-DP = extended-release dipyridamole 200mg; ASA = aspirin 25 mg. the dosage regimen for all treatment groups is b.i.d.
Combined Stroke or Death Endpoint
In ESPS2, aspirin and extended-release dipyridamole capsules reduced the risk of stroke or death by 12.1% compared to aspirin alone and by 10.3% compared to extended-release dipyridamole alone. These results were not statistically significant. Aspirin and extended-release dipyridamole capsules reduced the risk of stroke or death by 24.2% compared to placebo.
Death Endpoint
The incidence rate of all-cause mortality was 11.3% for aspirin and extended-release dipyridamole capsules, 11.0% for aspirin alone, 11.4% for extended-release dipyridamole alone and 12.3% for placebo alone. The differences between the aspirin and extended-release dipyridamole capsules, aspirin alone and extended-release dipyridamole alone treatment groups were not statistically significant. These incidence rates for aspirin and extended-release dipyridamole capsules and aspirin alone are consistent with previous aspirin studies in stroke and TIA patients.
16 HOW SUPPLIED/STORAGE AND HANDLING
Aspirin and extended-release dipyridamole capsules are available as:
25 mg/200 mg - Capsule, with a white cap and body, containing 200 mg of yellow extended-release pellets incorporating dipyridamole, USP and a round, white, film-coated tablet incorporating 25 mg of immediate-release aspirin, USP. The capsule is imprinted with  and 2510 on both cap and body in black ink. Aspirin and extended-release dipyridamole capsules are supplied in unit-of-use bottles of 60 capsules (NDC 0115-1711-13).
and 2510 on both cap and body in black ink. Aspirin and extended-release dipyridamole capsules are supplied in unit-of-use bottles of 60 capsules (NDC 0115-1711-13).
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Protect from excessive moisture.
Dispense in tight, light-resistant containers as defined in the USP.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information)
-
Risk of Bleeding
Inform patients that as with other antiplatelet agents, there is a general risk of bleeding including intracranial and gastrointestinal bleeding. Inform patients about the signs and symptoms of bleeding, including occult bleeding. Tell patients to notify their physician if they are prescribed any drug which may increase risk of bleeding.
Counsel patients who consume three or more alcoholic drinks daily about the bleeding risks involved with chronic, heavy alcohol use while taking aspirin.
-
Pregnancy
Inform patients that aspirin is known to be harmful to fetuses and ask the patient to notify them if they are or become pregnant.
-
Headaches
Some patients may experience headaches upon treatment initiation; these are usually transient. In case of intolerable headaches, tell patients to contact their physician.
-
Dosage and Administration
Tell patients that aspirin and extended-release dipyridamole capsules should be swallowed whole, and not chewed or crushed. If you miss a dose, continue with your next dose on your regular schedule. Do not take a double dose.
-
Storage
Inform patients to protect aspirin and extended-release dipyridamole capsules from moisture.
Manufactured by:
Actavis Elizabeth LLC
Elizabeth, NJ 07207 USA
Distributed by:
Impax Generics
Hayward, CA 94544
1930-01
Issued: August 2016
PATIENT INFORMATION
Aspirin (AS-pir-in) and Extended-Release Dipyridamole (dye-pir-ID-a-mole)
Capsules
Rx Only
Read this Patient Information before you start taking aspirin and extended-release dipyridamole capsules and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
What are aspirin and extended-release dipyridamole capsules?
Aspirin and extended-release dipyridamole capsules are a prescription medicine that contains aspirin and a medicine that is slowly released in your body, called dipyridamole. Aspirin and extended-release dipyridamole capsules are used to lower the risk of stroke in people who have had a “mini-stroke” (transient ischemic attack or TIA) or stroke due to a blood clot.
It is not known if aspirin and extended-release dipyridamole capsules are safe and effective in children. See “Who should not take aspirin and extended-release dipyridamole capsules?”
Who should not take aspirin and extended-release dipyridamole capsules?
Do not take aspirin and extended-release dipyridamole capsules if you:
- are allergic to any of the ingredients in aspirin and extended-release dipyridamole capsules. See the end of this leaflet for a list of ingredients in aspirin and extended-release dipyridamole capsules.
- are allergic to non-steroidal anti-inflammatory drugs (NSAIDs)
- have asthma in combination with runny nose and nasal polyps
Do not give aspirin and extended-release dipyridamole capsules to a child or teenager with a viral illness. Reye syndrome, a life-threatening condition, can happen when aspirin (an ingredient in aspirin and extended-release dipyridamole capsules) is used in children and teenagers who have certain viral illnesses.
What should I tell my doctor before using aspirin and extended-release dipyridamole capsules?
Before taking aspirin and extended-release dipyridamole capsules, tell your healthcare provider if you:
- have stomach ulcers
- have a history of bleeding problems
- have heart problems
- have kidney or liver problems
- have low blood pressure
- have myasthenia gravis
- have any other medical conditions
- are pregnant or plan to become pregnant. Aspirin and extended-release dipyridamole capsules can harm your unborn baby, especially if you take it in the last (third) trimester of pregnancy. You should not take aspirin and extended-release dipyridamole capsules during pregnancy without first talking to your healthcare provider. Tell your healthcare provider right away if you become pregnant while taking aspirin and extended-release dipyridamole capsules.
- are breast-feeding or plan to breast-feed. Aspirin and extended-release dipyridamole can pass into your milk and may harm your baby. Talk to your healthcare provider about the best way to feed your baby if you take aspirin and extended-release dipyridamole capsules.
Tell your doctor about all the medicines you take, including prescription and non-prescription medicines, vitamins and herbal supplements. Aspirin and extended-release dipyridamole capsules and other medicines may affect each other causing side effects. Aspirin and extended-release dipyridamole capsules may affect the way other medicines work, and other medicines may affect how aspirin and extended-release dipyridamole capsules work.
Especially tell your healthcare provider if you take:
- a medicine for high blood pressure, irregular heart beat, or heart failure
- acetazolamide [Diamox®]
- any blood thinner medicines
- warfarin sodium [Coumadin®, Jantoven®]
- a heparin medicine
- anagrelide [Agrylin®]
- a seizure medicine
- a medicine for Alzheimer’s disease
- a water pill
- methotrexate sodium [Trexall®]
- aspirin or a non-steroidal anti-inflammatory drug (NSAIDs). You should not take NSAIDs during treatment with aspirin and extended-release dipyridamole capsules. Using these medicines with aspirin and extended-release dipyridamole capsules can increase your risk of bleeding.
- a medicine for diabetes
- probenecid [Probalan®, Col-Probenecid®]
Ask your healthcare provider or pharmacist if you are not sure if your medicine is one that is listed above.
Know the medicines you take. Keep a list of them and show your healthcare provider and pharmacist when you get a new medicine.
How should I take aspirin and extended-release dipyridamole capsules?
- Take aspirin and extended-release dipyridamole capsules exactly as prescribed. Your healthcare provider will tell you how many aspirin and extended-release dipyridamole capsules to take and when to take them.
- Headaches are not uncommon when you first start taking aspirin and extended-release dipyridamole capsules, but often lessen as treatment continues. Tell your healthcare provider if you have a severe headache. Your healthcare provider may change the instructions for taking aspirin and extended-release dipyridamole capsules.
- Swallow aspirin and extended-release dipyridamole capsules whole. Do not crush or chew the capsules.
- You can take aspirin and extended-release dipyridamole capsules with or without food.
- If you miss a dose, take your next dose at the usual time. Do not take two doses at one time.
- If you take more aspirin and extended-release dipyridamole capsules (overdose) than prescribed, call your healthcare provider or Poison Control Center, or get emergency help right away.
Symptoms of an overdose of aspirin and extended-release dipyridamole capsules include:
- a warm feeling or flushing
- sweating
- restlessness
- weakness or dizziness
- a fast heart rate
- ringing in the ears
What should I avoid while using aspirin and extended-release dipyridamole capsules?
- heavy alcohol use. People who drink three or more alcoholic drinks every day have a higher risk of bleeding during treatment with aspirin and extended-release dipyridamole capsules, because it contains aspirin.
What are the possible side effects of aspirin and extended-release dipyridamole capsules?
Aspirin and extended-release dipyridamole capsules may cause serious side effects, including:
-
increased risk of bleeding. You may bleed more easily during aspirin and extended-release dipyridamole capsules treatment, and it may take longer than usual for bleeding to stop. This can include:
-
bleeding into your brain (intracranial hemorrhage). This can be a medical emergency. Get medical help right away if you have any of these symptoms while taking aspirin and extended-release dipyridamole capsules:
- severe headache with drowsiness
- confusion or memory change
- pass out (become unconscious)
-
bleeding in your stomach or intestine.
- stomach pain
- heartburn or nausea
- vomiting blood or vomit looks like “coffee grounds”
- red or bloody stools
- black stools that look like tar
-
bleeding into your brain (intracranial hemorrhage). This can be a medical emergency. Get medical help right away if you have any of these symptoms while taking aspirin and extended-release dipyridamole capsules:
- new or worsening chest pain in some people with heart disease. Tell your healthcare provider if you have new chest pain or have any change in your chest pain during treatment with aspirin and extended-release dipyridamole capsules.
-
liver problems, including increased liver function tests and liver failure. Tell your healthcare provider if you have any of these symptoms of a liver problem while taking aspirin and extended-release dipyridamole capsules:
- loss of appetite
- pale colored stool
- stomach area (abdomen) pain
- yellowing of your skin or whites of your eyes
- dark urine
- itching
Call your healthcare provider right away if you have any of the symptoms listed above.
The most common side effects of aspirin and extended-release dipyridamole capsules include:
- headache
- upset stomach
- diarrhea
These are not all the possible side effects of aspirin and extended-release dipyridamole capsules. Tell your healthcare provider or pharmacist if you have any side effect that bothers you or that does not go away.
Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store aspirin and extended-release dipyridamole capsules?
- Store aspirin and extended-release dipyridamole capsules at 59°F to 86°F (15°C to 30°C).
- Keep aspirin and extended-release dipyridamole capsules dry.
- Safely throw away medicine that is out of date or no longer needed.
Keep aspirin and extended-release dipyridamole capsules and all medicines out of the reach of children.
General information about aspirin and extended-release dipyridamole capsules
Medicines are sometimes prescribed for purposes other than those listed in the Patient Information. Do not use aspirin and extended-release dipyridamole capsules for a condition for which it was not prescribed. Do not give aspirin and extended-release dipyridamole capsules to other people, even if they have the same symptoms that you have. It may harm them.
This Patient Information summarizes the most important information about aspirin and extended-release dipyridamole capsules. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about aspirin and extended-release dipyridamole capsules that is written for health professionals.
For more information, call Impax Laboratories, Inc. at 1-800-934-6729.
What are the ingredients in aspirin and extended-release dipyridamole capsules?
Active Ingredients: dipyridamole, USP in an extended-release form and aspirin, USP
Inactive Ingredients: colloidal silicon dioxide, corn starch, hydrolyzed methacrylic acid copolymer type C, gelatin, hydroxypropyl cellulose, hypromellose 2910, methacrylic acid copolymer type B, microcrystalline cellulose, polyethylene glycol 3350, polyvinyl alcohol, sodium bicarbonate, sodium lauryl sulfate, sodium starch glycolate type A, stearic acid, talc, tartaric acid, titanium dioxide, triacetin and triethyl citrate. The capsules are imprinted with black Tek-Print ink SW-9008 or black opacode S-1-17823 which contain black iron oxide, potassium hydroxide, propylene glycol and shellac.
Brands listed are the trademarks of their respective owners.
Manufactured by:
Actavis Elizabeth LLC
Elizabeth, NJ 07207 USA
Distributed by:
Impax Generics
Hayward, CA 94544
1930-01
Issued: August 2016
| ASPIRIN AND DIPYRIDAMOLE
aspirin and dipyridamole capsule, extended release |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
| Labeler - Impax Generics (079832487) |