FULL PRESCRIBING INFORMATION
WARNING: SERIOUS PULMONARY OIL MICROEMBOLISM (POME) REACTIONS AND ANAPHYLAXIS
- Serious POME reactions, involving urge to cough, dyspnea, throat tightening, chest pain, dizziness, and syncope; and episodes of anaphylaxis, including life-threatening reactions, have been reported to occur during or immediately after the administration of testosterone undecanoate injection. These reactions can occur after any injection of testosterone undecanoate during the course of therapy, including after the first dose [see Warnings and Precautions (5.1)].
- Following each injection of AVEED, observe patients in the healthcare setting for 30 minutes in order to provide appropriate medical treatment in the event of serious POME reactions or anaphylaxis [see Warnings and Precautions (5.1)].
- Because of the risks of serious POME reactions and anaphylaxis, AVEED is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the AVEED REMS Program [see Warnings and Precautions (5.2)].
1 INDICATIONS AND USAGE
AVEED is indicated for testosterone replacement therapy in adult males for conditions associated with a deficiency or absence of endogenous testosterone.
- Primary hypogonadism (congenital or acquired): testicular failure due to cryptorchidism, bilateral torsion, orchitis, vanishing testis syndrome, orchiectomy, Klinefelter's syndrome, chemotherapy, or toxic damage from alcohol or heavy metals. These men usually have low serum testosterone concentrations and gonadotropins (follicle-stimulating hormone [FSH], luteinizing hormone [LH]) above the normal range.
- Hypogonadotropic hypogonadism (congenital or acquired): gonadotropin or luteinizing hormone-releasing hormone (LHRH) deficiency or pituitary-hypothalamic injury from tumors, trauma, or radiation. These men have low testosterone serum concentrations but have gonadotropins in the normal or low range.
AVEED should only be used in patients who require testosterone replacement therapy and in whom the benefits of the product outweigh the serious risks of POME and anaphylaxis.
Limitations of Use
- Safety and efficacy of AVEED in men with “age-related hypogonadism” (also referred to as “late-onset hypogonadism”) have not been established.
- Safety and efficacy of AVEED in males less than 18 years old have not been established [see Use in Specific Populations (8.4)].
2 DOSAGE AND ADMINISTRATION
Prior to initiating AVEED, confirm the diagnosis of hypogonadism by ensuring that serum testosterone concentrations have been measured in the morning on at least 2 separate days and that these serum testosterone concentrations are below the normal range.
2.1 Dosage
AVEED is for intramuscular use only. Dosage titration is not necessary.
Inject AVEED deeply into the gluteal muscle following the usual precautions for intramuscular administration; care must be taken to avoid intravascular injection [see Dosage and Administration (2.3)]. Intravascular injection of AVEED may lead to POME [see Warnings and Precautions (5.1)].
The recommended dose of AVEED is 3 mL (750 mg) injected intramuscularly, followed by 3 mL (750 mg) injected after 4 weeks, then 3 mL (750 mg) injected every 10 weeks thereafter.
2.2 Preparation Instructions
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Carefully remove the gray plastic cap from the top of the vial by lifting it up from the edges with your fingers or by pushing the bottom edge of the cap upward using the top of your thumb. Remove only the gray plastic cap while leaving the aluminum metal ring and crimp seal around the gray rubber stopper in place. To facilitate the removal of medication from the vial, attach an 18-gauge needle and draw 3 mL of air into the syringe. Hold the needle at a 45° angle to the stopper with the bevel in the up orientation. Inject through the gray rubber stopper into the vial to create positive pressure within the vial chamber.
Withdraw 3 mL (750 mg) of AVEED solution from the vial. Expel excess air bubbles from the syringe. Replace the syringe needle used to draw up the solution from the vial with a new intramuscular needle and inject. Discard any unused portion in the vial.
2.3 Administration Instructions
The site for injection for AVEED is the gluteus medius muscle site located in the upper outer quadrant of the buttock. Care must be taken to avoid the needle hitting the superior gluteal arteries and sciatic nerve. Between consecutive injections, alternate the injection site between left and right buttock.
Figure 1: Identifying the Injection Site
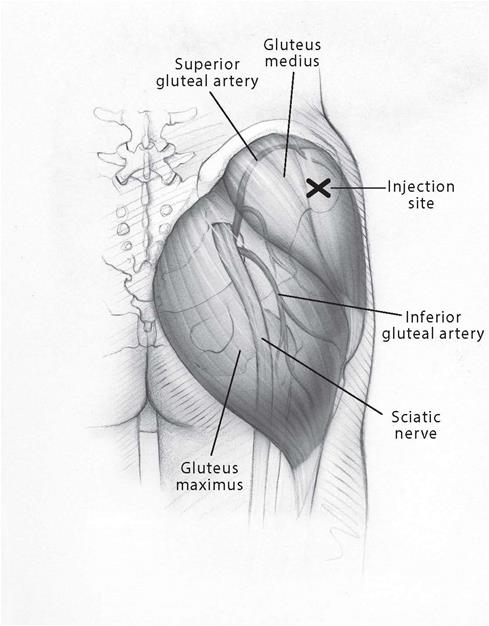
Following antiseptic skin preparation, enter the muscle and maintain the syringe at a 90° angle with the needle in its deeply imbedded position. Grasp the barrel of the syringe firmly with one hand. With the other hand, pull back on the plunger and aspirate for several seconds to ensure that no blood appears. If any blood is drawn into the syringe, immediately withdraw and discard the syringe and prepare another dose.
If no blood is aspirated, reinforce the current needle position to avoid any movement of the needle and slowly (over 60 to 90 seconds) depress the plunger carefully and at a constant rate, until all the medication has been delivered. Be sure to depress the plunger completely with sufficient controlled force. Withdraw the needle.
Immediately upon removal of the needle from the muscle, apply gentle pressure with a sterile pad to the injection site. If there is bleeding at the site of injection, apply a bandage.
Following each injection of AVEED, observe patients in the healthcare setting for 30 minutes in order to provide appropriate medical treatment in the event of serious POME reactions or anaphylaxis [see Warnings and Precautions (5.1)].
3 DOSAGE FORMS AND STRENGTHS
750 mg/3 mL (250 mg/mL) testosterone undecanoate sterile injectable solution is provided in an amber glass, single use vial with silver-colored crimp seal and gray plastic cap.
4 CONTRAINDICATIONS
AVEED should not be used in any of the following patients:
- Men with carcinoma of the breast or known or suspected carcinoma of the prostate [see Warnings and Precautions (5.3)].
- Women who are pregnant. Testosterone can cause virilization of the female fetus when administered to a pregnant woman [see Use in Specific Populations (8.1, 8.2)].
- Men with known hypersensitivity to AVEED or any of its ingredients (testosterone undecanoate, refined castor oil, benzyl benzoate).
5 WARNINGS AND PRECAUTIONS
5.1 Serious Pulmonary Oil Microembolism (POME) Reactions and Anaphylaxis
Serious POME reactions, involving cough, urge to cough, dyspnea, hyperhidrosis, throat tightening, chest pain, dizziness, and syncope, have been reported to occur during or immediately after the injection of intramuscular testosterone undecanoate 1000 mg (4 mL). The majority of these events lasted a few minutes and resolved with supportive measures; however, some lasted up to several hours and some required emergency care and/or hospitalization. To minimize the risk of intravascular injection of AVEED, care should be taken to inject the preparation deeply into the gluteal muscle, being sure to follow the recommended procedure for intramuscular administration [see Dosage and Administration (2.2, 2.3) and Adverse Reactions (6.2)].
In addition to serious POME reactions, episodes of anaphylaxis, including life-threatening reactions, have also been reported to occur following the injection of intramuscular testosterone undecanoate.
Both serious POME reactions and anaphylaxis can occur after any injection of testosterone undecanoate during the course of therapy, including after the first dose. Patients with suspected hypersensitivity reactions to AVEED should not be re-treated with AVEED.
Following each injection of AVEED, observe patients in the healthcare setting for 30 minutes in order to provide appropriate medical treatment in the event of serious POME reactions and anaphylaxis.
5.2 AVEED Risk Evaluation and Mitigation Strategy (REMS) Program
AVEED is available only through a restricted program called the AVEED REMS Program because of the risk of serious POME and anaphylaxis.
Notable requirements of the AVEED REMS Program include the following:
- Healthcare providers who prescribe AVEED must be certified with the REMS Program before ordering or dispensing AVEED.
- Healthcare settings must be certified with the REMS Program and have healthcare providers who are certified before ordering or dispensing AVEED. Healthcare settings must have on-site access to equipment and personnel trained to manage serious POME and anaphylaxis.
Further information is available at www.aveedrems.com or call 1-855-755-0494.
5.3 Worsening of Benign Prostatic Hyperplasia (BPH) and Potential Risk of Prostate Cancer
Patients with BPH treated with androgens are at an increased risk of worsening of signs and symptoms of BPH. Monitor patients with BPH for worsening signs and symptoms.
Patients treated with androgens may be at an increased risk for prostate cancer. Evaluate patients for prostate cancer prior to initiating and during treatment with androgens [see Contraindications (4)].
5.4 Polycythemia
Increases in hematocrit, reflective of increases in red blood cell mass, may require discontinuation of testosterone.
Check hematocrit prior to initiating testosterone treatment. It would be appropriate to re-evaluate the hematocrit 3 to 6 months after starting testosterone treatment, and then annually. If hematocrit becomes elevated, stop therapy until hematocrit decreases to an acceptable level. An increase in red blood cell mass may increase the risk of thromboembolic events.
5.5 Venous Thromboembolism (VTE)
There have been postmarketing reports of venous thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), in patients using testosterone products, such as AVEED. Evaluate patients who report symptoms of pain, edema, warmth and erythema in the lower extremity for DVT and those who present with acute shortness of breath for PE. If a venous thromboembolic event is suspected, discontinue treatment with AVEED and initiate appropriate workup and management.
5.6 Cardiovascular Risk
Long-term clinical safety trials have not been conducted to assess the cardiovascular outcomes of testosterone replacement therapy in men. To date, epidemiologic studies and randomized controlled trials have been inconclusive for determining the risk of major adverse cardiovascular events (MACE), such as non-fatal myocardial infarction, non-fatal stroke, and cardiovascular death, with the use of testosterone compared to non-use. Some studies, but not all, have reported an increased risk of MACE in association with use of testosterone replacement therapy in men. Patients should be informed of this possible risk when deciding whether to use or to continue to use AVEED.
5.7 Abuse of Testosterone and Monitoring of Serum Testosterone Concentrations
Testosterone has been subject to abuse, typically at doses higher than recommended for the approved indication and in combination with other anabolic androgenic steroids. Anabolic androgenic steroid abuse can lead to serious cardiovascular and psychiatric adverse reactions [see Drug Abuse and Dependence (9)].
If testosterone abuse is suspected, check serum testosterone concentrations to ensure they are within therapeutic range. However, testosterone levels may be in the normal or subnormal range in men abusing synthetic testosterone derivatives. Counsel patients concerning the serious adverse reactions associated with abuse of testosterone and anabolic androgenic steroids. Conversely, consider the possibility of testosterone and anabolic androgenic steroid abuse in suspected patients who present with serious cardiovascular or psychiatric adverse events.
5.8 Use in Women
Due to lack of controlled evaluations in women and potential virilizing effects, AVEED is not indicated for use in women [see Contraindications (4) and Use in Specific Populations (8.1, 8.2)].
5.9 Potential for Adverse Effects on Spermatogenesis
With large doses of exogenous androgens, including AVEED, spermatogenesis may be suppressed through feedback inhibition of pituitary FSH which could possibly lead to adverse effects on semen parameters including sperm count.
5.10 Hepatic Adverse Effects
Prolonged use of high doses of orally active 17-alpha-alkyl androgens (eg, methyltestosterone) has been associated with serious hepatic adverse effects (peliosis hepatis, hepatic neoplasms, cholestatic hepatitis, and jaundice). Peliosis hepatis can be a life threatening or fatal complication. Long-term therapy with intramuscular testosterone enanthate, which elevates blood levels for prolonged periods, has produced multiple hepatic adenomas. AVEED is not known to produce these adverse effects. Nonetheless, patients should be instructed to report any signs or symptoms of hepatic dysfunction (eg, jaundice). If these occur, promptly discontinue AVEED while the cause is evaluated.
5.11 Edema
Androgens, including AVEED, may promote retention of sodium and water. Edema with or without congestive heart failure may be a serious complication in patients with preexisting cardiac, renal, or hepatic disease. In addition to discontinuation of the drug, diuretic therapy may be required.
5.12 Gynecomastia
Gynecomastia occasionally develops and occasionally persists in patients being treated for hypogonadism [see Adverse Reactions (6.1)].
5.13 Sleep Apnea
The treatment of hypogonadal men with testosterone products may potentiate sleep apnea in some patients, especially those with risk factors such as obesity or chronic lung diseases.
5.14 Lipids
Changes in serum lipid profile may require dose adjustment of lipid lowering drugs or discontinuation of testosterone therapy.
5.15 Hypercalcemia
Androgens, including AVEED, should be used with caution in cancer patients at risk of hypercalcemia (and associated hypercalciuria). Regular monitoring of serum calcium concentrations is recommended in these patients.
5.16 Decreased Thyroxine-binding Globulin
Androgens, including AVEED, may decrease concentrations of thyroxine-binding globulin, resulting in decreased total T4 serum concentrations and increased resin uptake of T3 and T4. Free thyroid hormone concentrations remain unchanged, however, and there is no clinical evidence of thyroid dysfunction.
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
AVEED was evaluated in an 84-week clinical study using a dose regimen of 750 mg (3 mL) at initiation, at 4 weeks, and every 10 weeks thereafter in 153 hypogonadal men. The most commonly reported adverse reactions (>2%) were: acne (5.2%), injection site pain (4.6%), prostate specific antigen increased (4.6%), hypogonadism (2.6%) and estradiol increased (2.6%).
Table 1 presents adverse reactions reported by ≥1% of patients in the 84-week clinical study.
Table 1: Adverse Reactions Reported in at Least 1% of Patients in the 84-Week Clinical Study of AVEED
|
MedDRA Preferred Term |
Number of Patients (%) |
|
AVEED 750 mg |
|
|
Acne |
8 (5.2%) |
|
Injection site pain |
7 (4.6%) |
|
Prostatic specific antigen increased* |
7 (4.6%) |
|
Estradiol increased |
4 (2.6%) |
|
Hypogonadism |
4 (2.6%) |
|
Fatigue |
3 (2%) |
|
Irritability |
3 (2%) |
|
Hemoglobin increased |
3 (2%) |
|
Insomnia |
3 (2%) |
|
Mood swings |
3 (2%) |
|
Aggression |
2 (1.3%) |
|
Ejaculation disorder |
2 (1.3%) |
|
Injection site erythema |
2 (1.3%) |
|
Hematocrit increased |
2 (1.3%) |
|
Hyperhidrosis |
2 (1.3%) |
|
Prostate Cancer |
2 (1.3%) |
|
Prostate induration |
2 (1.3%) |
|
Weight increased |
2 (1.3%) |
*Prostate-specific antigen increased defined as a serum PSA concentration >4 ng/mL.
In the 84-week clinical trial, 7 patients (4.6%) discontinued treatment because of adverse reactions. Adverse reactions leading to discontinuation included: hematocrit increased, estradiol increased, prostatic specific antigen increased, prostate cancer, mood swings, prostatic dysplasia, acne, and deep vein thrombosis.
During the 84-week clinical trial, the average serum PSA increased from 1.0 ± 0.8 ng/mL at baseline to 1.5 ± 1.3 ng/mL at the end of study. Fourteen (14) patients (10.9%) in whom the baseline PSA was < 4 ng/mL had a post-baseline serum PSA of > 4 ng/mL during the 84-week treatment period.
A total of 725 hypogonadal men received intramuscular testosterone undecanoate in a total of 7 controlled clinical trials. In these clinical trials, the dose and dose frequency of intramuscular testosterone undecanoate varied from 750 mg to 1000 mg, and from every 9 weeks to every 14 weeks. Several of these clinical trials incorporated additional doses upon initiation of therapy (eg, loading doses). In addition to those adverse reactions noted in Table 1, the following adverse events were reported by at least 3% of patients in these trials, irrespective of the investigator’s assessment of relationship to study medication: sinusitis, prostatitis, arthralgia, nasopharyngitis, upper respiratory tract infection, bronchitis, back pain, hypertension, diarrhea and headache.
Pulmonary Oil Microembolism (POME) and Anaphylaxis in Controlled Clinical Studies
Adverse events attributable to POME and anaphylaxis were reported in a small number of patients in controlled clinical trials. In the 84-week clinical trial of AVEED, 1 patient experienced a mild coughing fit lasting 10 minutes after his third injection, which was retrospectively attributed to POME. In another clinical trial of intramuscular testosterone undecanoate (1000 mg), a hypogonadal male patient experienced the urge to cough and respiratory distress at 1 minute after his tenth injection, which was also retrospectively attributed to POME.
During a review that involved adjudication of all cases meeting specific criteria, 9 POME events in 8 patients and 2 events of anaphylaxis among 3,556 patients treated with intramuscular testosterone undecanoate in 18 clinical trials were judged to have occurred.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of AVEED. Because the reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Pulmonary Oil Microembolism (POME) and Anaphylaxis
Serious POME reactions, involving cough, urge to cough, dyspnea, hyperhidrosis, throat tightening, chest pain, dizziness, and syncope, have been reported to occur during or immediately after the injection of intramuscular testosterone undecanoate 1000 mg (4 mL) in post-approval use outside the United States. The majority of these events lasted a few minutes and resolved with supportive measures; however, some lasted up to several hours and some required emergency care and/or hospitalization.
In addition to serious POME reactions, episodes of anaphylaxis, including life-threatening reactions, have also been reported to occur following the injection of intramuscular testosterone undecanoate in post-approval use outside of the United States.
Both serious POME reactions and anaphylaxis have been reported to occur after any injection of testosterone undecanoate during the course of therapy, including after the first dose.
Other Events
The following treatment emergent adverse events or adverse reactions have been identified during post-marketing clinical trials and during post-approval use of intramuscular testosterone undecanoate. In most cases, the dose being used was 1000 mg.
Blood and Lymphatic System Disorders: polycythemia, thrombocytopenia
Cardiac Disorders: angina pectoris, cardiac arrest, cardiac failure, coronary artery disease, coronary artery occlusion, myocardial infarction, tachycardia
Ear and Labyrinth Disorders: sudden hearing loss, tinnitus
Endocrine Disorders: hyperparathyroidism, hypoglycemia
Gastrointestinal Disorders: abdominal pain upper, diarrhea, vomiting
General Disorders and Administrative Site Conditions: chest pain, edema peripheral, injection site discomfort, injection site hematoma, injection site irritation, injection site pain, injection site reaction, malaise, paresthesia, procedural pain
Immune System Disorders: anaphylactic reaction, anaphylactic shock, asthma, dermatitis allergic, hypersensitivity, leukocytoclastic vasculitis
Infections and Infestations: injection site abscess, prostate infection
Investigations: alanine aminotransferase increased, aspartate aminotransferase increased, blood bilirubin increased, blood glucose increased, blood pressure increased, blood prolactin increased, blood testosterone decreased, blood testosterone increased, blood triglycerides increased, gamma-glutamyltransferase increased, hematocrit increased, intraocular pressure increased, liver function test abnormal, prostate examination abnormal, prostatic specific antigen increased, transaminases increased
Metabolism and Nutrition Disorders: diabetes mellitus, fluid retention, hyperlipidemia, hypertriglyceridemia
Musculoskeletal and Connective Tissue Disorders: musculoskeletal chest pain, musculoskeletal pain, myalgia, osteopenia, osteoporosis, systemic lupus erythematosus
Neoplasms Benign, Malignant and Unspecified (including cysts and polyps): prostate cancer, prostatic intraepithelial neoplasia
Nervous System Disorders: stroke, cerebrovascular insufficiency, reversible ischemic neurological deficiency, transient ischemic attack
Psychiatric Disorders: aggression, anxiety, depression, insomnia, irritability, Korsakoff’s psychosis non-alcoholic, male orgasmic disorder, nervousness, restlessness, sleep disorder
Renal and Urinary Disorders: calculus urinary, dysuria, hematuria, nephrolithiasis, pollakiuria, renal colic, renal pain, urinary tract disorder
Reproductive System and Breast Disorders: azoospermia, benign prostatic hyperplasia, breast induration, breast pain, erectile dysfunction, gynecomastia, libido decreased, libido increased, prostate induration, prostatitis, spermatocele, testicular pain
Respiratory, Thoracic and Mediastinal Disorders: asthma, chronic obstructive pulmonary disease, cough, dysphonia, dyspnea, hyperventilation, obstructive airway disorder, pharyngeal edema, pharyngolaryngeal pain, pulmonary microemboli, pulmonary embolism, respiratory distress, rhinitis, sleep apnea syndrome, snoring
Skin and Subcutaneous Tissue Disorders: acne, alopecia, angioedema, angioneurotic edema, dermatitis allergic, erythema, hyperhidrosis, pruritus, rash
Vascular Disorders: cerebral infarction, cerebrovascular accident, circulatory collapse, deep venous thrombosis, hot flush, hypertension, syncope, thromboembolism, thrombosis, venous insufficiency
7 DRUG INTERACTIONS
7.1 Insulin
Changes in insulin sensitivity or glycemic control may occur in patients treated with androgens. In diabetic patients, the metabolic effects of androgens may decrease blood glucose and, therefore, may necessitate a decrease in the dose of anti-diabetic medication.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
AVEED is contraindicated in pregnant women. Testosterone is teratogenic and may cause fetal harm based on data from animal studies and its mechanism of action [see Contraindications (4) and Clinical Pharmacology (12.1)]. Exposure of a female fetus to androgens may result in varying degrees of virilization. In animal development studies, exposure to testosterone in utero resulted in hormonal and behavioral changes in offspring and structural impairments of reproductive tissues in female and male offspring. These studies did not meet current standards for nonclinical development toxicity studies.
Data
Animal Data
In developmental studies conducted in rats, rabbits, pigs, sheep and rhesus monkeys, pregnant animals received intramuscular injection of testosterone during the period of organogenesis. Testosterone treatment at doses that were comparable to those used for testosterone replacement therapy resulted in structural impairments in both female and male offspring. Structural impairments observed in females included increased anogenital distance, phallus development, empty scrotum, no external vagina, intrauterine growth retardation, reduced ovarian reserve, and increased ovarian follicular recruitment. Structural impairments seen in male offspring included increased testicular weight, larger seminal tubular lumen diameter, and higher frequency of occluded tubule lumen. Increased pituitary weight was seen in both sexes.
Testosterone exposure in utero also resulted in hormonal and behavioral changes in offspring. Hypertension was observed in pregnant female rats and their offspring exposed to doses approximately twice those used for testosterone replacement therapy.
8.3 Females and Males of Reproductive Potential
Infertility
During treatment with large doses of exogenous androgens, including AVEED, spermatogenesis may be suppressed through feedback inhibition of the hypothalamic-pituitary-testicular axis [see Warnings and Precautions (5.9)], possibly leading to adverse effects on semen parameters including sperm count. Reduced fertility is observed in some men taking testosterone replacement therapy. Testicular atrophy, subfertility, and infertility have also been reported in men who abuse anabolic androgenic steroids [see Drug Abuse and Dependence (9.2)]. With either type of use, the impact on fertility may be irreversible.
8.4 Pediatric Use
Safety and effectiveness of AVEED in pediatric patients less than 18 years old have not been established. Improper use may result in acceleration of bone age and premature closure of epiphyses.
8.5 Geriatric Use
There have not been sufficient numbers of geriatric patients in controlled clinical studies with AVEED to determine whether efficacy or safety in those over 65 years of age differs from younger subjects. Of the 153 patients enrolled in the pivotal clinical study utilizing AVEED, 26 (17.0%) were over 65 years of age. Additionally, there are insufficient long-term safety data in geriatric patients to assess the potentially increased risk of cardiovascular disease and prostate cancer.
Geriatric patients treated with androgens may also be at risk for worsening of signs and symptoms of BPH [see Warnings and Precautions (5.3)].
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
AVEED contains testosterone, a Schedule III controlled substance in the Controlled Substances Act.
9.2 Abuse
Drug abuse is intentional non-therapeutic use of a drug, even once, for its rewarding psychological and physiological effects. Abuse and misuse of testosterone are seen in male and female adults and adolescents. Testosterone, often in combination with other anabolic androgenic steroids (AAS), and not obtained by prescription through a pharmacy, may be abused by athletes and bodybuilders. There have been reports of misuse of men taking higher doses of legally obtained testosterone than prescribed and continuing testosterone despite adverse events or against medical advice.
Abuse-Related Adverse Reactions
Serious adverse reactions have been reported in individuals who abuse anabolic androgenic steroids, and include cardiac arrest, myocardial infarction, hypertrophic cardiomyopathy, congestive heart failure, cerebrovascular accident, hepatotoxicity, and serious psychiatric manifestations, including major depression, mania, paranoia, psychosis, delusions, hallucinations, hostility, and aggression.
The following adverse reactions have also been reported in men: transient ischemic attacks, convulsions, hypomania, irritability, dyslipidemias, testicular atrophy, subfertility, and infertility.
The following additional adverse reactions have been reported in women: hirsutism, virilization, deepening of voice, clitoral enlargement, breast atrophy, male-pattern baldness, and menstrual irregularities.
The following adverse reactions have been reported in male and female adolescents: premature closure of bony epiphyses with termination of growth, and precocious puberty.
Because these reactions are reported voluntarily from a population of uncertain size and may include abuse of other agents, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
9.3 Dependence
Behaviors Associated with Addiction
Continued abuse of testosterone and other anabolic steroids, leading to addiction is characterized by the following behaviors:
- Taking greater dosages than prescribed
- Continued drug use despite medical and social problems due to drug use
- Spending significant time to obtain the drug when supplies of the drug are interrupted
- Giving a higher priority to drug use than other obligations
- Having difficulty in discontinuing the drug despite desires and attempts to do so
- Experiencing withdrawal symptoms upon abrupt discontinuation of use
Physical dependence is characterized by withdrawal symptoms after abrupt drug discontinuation or a significant dose reduction of a drug. Individuals taking supratherapeutic doses of testosterone may experience withdrawal symptoms lasting for weeks or months which include depressed mood, major depression, fatigue, craving, restlessness, irritability, anorexia, insomnia, decreased libido, and hypogonadotropic hypogonadism.
Drug dependence in individuals using approved doses of testosterone for approved indications has not been documented.
10 OVERDOSAGE
There have been no reports of overdosage in the AVEED clinical trials. There is 1 report of acute overdosage with use of an approved injectable testosterone product: this subject had serum testosterone levels of up to 11,400 ng/dL with a cerebrovascular accident.
Treatment of overdosage would consist of discontinuation of AVEED together with appropriate symptomatic and supportive care.
11 DESCRIPTION
AVEED (testosterone undecanoate) injection contains testosterone undecanoate (17β-undecanoyloxy-4-androsten-3-one) which is an ester of the androgen, testosterone. Testosterone is formed by cleavage of the ester side chain of testosterone undecanoate.
Testosterone undecanoate is a white to off-white crystalline substance. The empirical formula of testosterone undecanoate is C30H48O3 and a molecular weight of 456.7. The structural formula is:
Figure 2: Testosterone Undecanoate
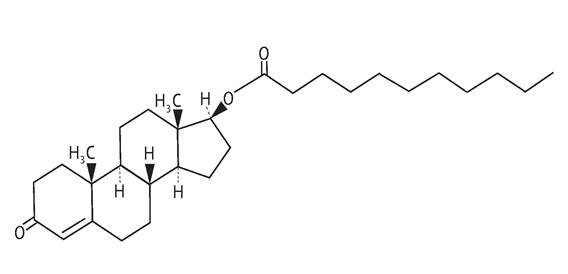
C30H48O3 MW: 456.7
AVEED is a clear, yellowish, sterile oily solution containing testosterone undecanoate, a testosterone ester, for intramuscular injection. Each single use vial contains 3 mL of 250 mg/mL testosterone undecanoate solution in a mixture of 1500 mg of benzyl benzoate and 885 mg of refined castor oil.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Endogenous androgens, including testosterone and dihydrotestosterone (DHT) are responsible for the normal growth and development of the male sex organs and for maintenance of secondary sex characteristics. These effects include the growth and maturation of prostate, seminal vesicles, penis, and scrotum; the development of male hair distribution, such as facial, pubic, chest, and axillary hair; laryngeal enlargement; vocal cord thickening; and alterations in body musculature and fat distribution.
Male hypogonadism, a clinical syndrome resulting from insufficient secretion of testosterone, has 2 main etiologies. Primary hypogonadism is caused by defects of the gonads, such as Klinefelter’s syndrome or Leydig cell aplasia, whereas secondary hypogonadism is the failure of the hypothalamus (or pituitary) to produce sufficient gonadotropins (FSH, LH).
12.3 Pharmacokinetics
Absorption
AVEED 750 mg delivers physiologic amounts of testosterone, producing circulation testosterone concentrations that approximate normal concentrations (300-1000 ng/dL) seen in healthy men.
Testosterone esters in oil injected intramuscularly are absorbed from the lipid phase. Cleavage of the undecanoic acid side chain of AVEED by tissue esterases releases testosterone.
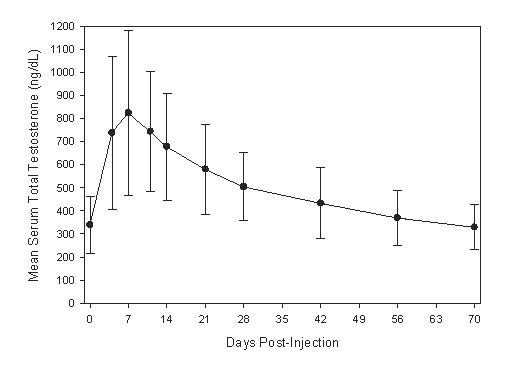
Following intramuscular injection of 750 mg of AVEED, serum testosterone concentrations reach a maximum after a median of 7 days (range 4 to 42 days) then slowly decline (Figure 3). Steady-state serum testosterone concentration was achieved with the third injection of AVEED at 14 weeks.
Figure 3 shows the mean serum total testosterone concentration-time profile during the third injection interval (at steady state, 14 to 24 weeks) for hypogonadal men (less than 300 ng/dL) given 750 mg AVEED at initiation, at 4 weeks, and every 10 weeks thereafter. Intramuscular injection of 750 mg of AVEED generates mean steady-state serum total testosterone concentrations in the normal range for 10 weeks.
Figure 3: Mean (SD) Serum Total Testosterone
Concentrations (ng/dL) at 14 to 24 Weeks
Distribution
Circulating testosterone is chiefly bound in the serum to sex hormone-binding globulin (SHBG) and albumin.
Approximately 40% of testosterone in plasma is bound to SHBG, 2% remains unbound (free), and the rest is loosely bound to albumin and other proteins.
Metabolism
Testosterone undecanoate is metabolized to testosterone via ester cleavage of the undecanoate group. The mean (SD) maximum concentration of testosterone undecanoate was 90.9 (68.8) ng/dL on Day 4 following injection of AVEED. Testosterone undecanoate was nearly undetectable 42 days following injection of AVEED.
Testosterone is metabolized to various 17-keto steroids through 2 different pathways. The major active metabolites of testosterone are estradiol and DHT.
DHT concentrations increased in parallel with testosterone concentrations during AVEED treatment. Average DHT concentrations during a dosing interval ranged from 244 to 451 ng/dL. The mean DHT to testosterone ratios ranged from 0.05 to 0.07.
Excretion
There is considerable variation in the half-life of testosterone as reported in the literature, ranging from 10 to 100 minutes. About 90% of a testosterone dose given intramuscularly is excreted in the urine as glucuronic and sulfuric acid-conjugates of testosterone or as metabolites. About 6% of a dose is excreted in the feces, mostly in the unconjugated form. Inactivation of testosterone occurs primarily in the liver.
Effect of Body Weight and Body Mass Index (BMI)
Analysis of serum testosterone concentrations from 117 hypogonadal men in the 84-week clinical study of AVEED indicated that serum testosterone concentrations achieved were inversely correlated with the patient’s body weight. In 60 patients with pretreatment body weight of ≥100 kg, the mean (±SD) serum testosterone average concentration was 426 ± 104 ng/dL. A higher serum testosterone average concentration (568 ± 139 ng/dL) was observed in 57 patients weighing 65 to 100 kg. A similar trend was also observed for maximum serum testosterone concentrations.
In 70 patients with pretreatment BMIs of >30 kg/m2, the mean (±SD) serum testosterone average concentration was 445 ± 116 ng/dL. Higher serum testosterone average concentrations (579 ± 101 ng/dL and 567± 155ng/dL) were observed in patients with BMIs <26 kg/m2 and 26 to 30 kg/m2, respectively. A similar trend was also observed for maximum serum testosterone concentrations.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Testosterone has been tested by subcutaneous injection and implantation in mice and rats. In mice, the implant induced cervical-uterine tumors, which metastasized in some cases. There is suggestive evidence that injection of testosterone into some strains of female mice increases their susceptibility to hepatoma. Testosterone is also known to increase the number of tumors and decrease the degree of differentiation of chemically induced carcinomas of the liver in rats.
Mutagenesis
AVEED was negative in the in vitro Ames assays, the chromosomal aberration assay in human lymphocytes, and in the in vivo mouse micronucleus assay.
Impairment of Fertility
The administration of exogenous testosterone has been reported to suppress spermatogenesis in the rat, dog, and non-human primates, which was reversible on cessation of the treatment.
14 CLINICAL STUDIES
14.1 Testosterone Replacement Therapy
AVEED was evaluated for efficacy in an 84-week, single-arm, open-label, multicenter study of 130 hypogonadal men. Eligible patients weighed at least 65 kg, were 18 years of age and older (mean age 54.2 years), and had a morning serum total testosterone concentration <300 ng/dL (mean screening testosterone concentration 215 ng/dL). Patients were caucasian (74.6%), black (12.3%), Hispanic (10.8%), and of other ethnicities (2.3%). The mean BMI was 32 kg/m2.
All patients received injections of AVEED 750 mg at baseline, at 4 weeks, and then every 10 weeks thereafter.
The primary endpoint was the percentage of patients with average serum total testosterone concentration (Cavg) within the normal range (300-1000 ng/dL) after the third injection, at steady state.
The secondary endpoint was the percentage of patients with maximum total testosterone concentration (Cmax) above 3 pre-determined limits: greater than 1500 ng/dL, between 1800 and 2499 ng/dL, and greater than 2500 ng/dL.
A total of 117 out of 130 hypogonadal men completed study procedures through Week 24 and were included in the evaluation of testosterone pharmacokinetics after the third AVEED injection. Ninety-four percent (94%) of patients maintained a Cavg within the normal range (300 to 1000 ng/dL). The percentages of patients with Cavg below the normal range (less than 300 ng/dL) and above the normal range (greater than 1000 ng/dL) were 5.1% and 0.9%, respectively.
Table 2 summarizes the mean (SD) serum total testosterone pharmacokinetic parameters at steady state for these 117 patients.
Table 2: Mean (SD) Serum Total Testosterone Concentrations at Steady State
|
AVEED 750 mg (N=117) |
|
|
Cavg (0 to 10 weeks) (ng/dL) |
495 (142) |
|
Cmax (ng/dL) |
891 (345) |
|
Cmin (ng/dL) |
324 (99) |
Cavg = average concentration; Cmax = maximum concentration; Cmin = minimum concentration
The percentage of patients with Cmax >1500 ng/dL was 7.7%. No patient had a Cmax >1800 ng/dL.
16 HOW SUPPLIED/STORAGE AND HANDLING
AVEED, NDC 67979-511-43: 750 mg/3 mL (250 mg/mL) testosterone undecanoate sterile injectable solution is provided in an amber glass vial with silver-colored crimp seal and gray plastic cap. Each vial is individually packaged in a carton box.
Store at controlled room temperature 25ºC (77ºF); excursions permitted to 15ºC - 30ºC (59ºF - 86ºF) [See USP controlled room temperature] in its original carton until the date indicated.
Before use, each vial should be visually inspected. Only vials free from particles should be used.
Single Use Vial. Discard unused portion.
17 PATIENT COUNSELING INFORMATION
See FDA-Approved Medication Guide.
Advise patients of the following:
17.1 Risks of Serious Pulmonary Oil Microembolism (POME) and Anaphylaxis
- Serious POME reactions, involving cough, urge to cough, shortness of breath, sweating, throat tightening, chest pain, dizziness, and syncope, have been reported to occur during or immediately after the injection of intramuscular testosterone undecanoate. The majority of these events lasted a few minutes and resolved with supportive measures; however, some lasted up to several hours and some required emergency care and/or hospitalization.
- Episodes of anaphylaxis, including life-threatening reactions, have also been reported to occur following the injection of intramuscular testosterone undecanoate.
- Both serious POME reactions and anaphylaxis can occur after any injection of testosterone undecanoate during the course of therapy, including after the first dose.
- Advise the patient to read the AVEED REMS information sheet titled "What You Need to Know About AVEED® Treatment: A Patient Guide".
- Instruct patients to remain at the healthcare setting for 30 minutes after each AVEED injection.
17.2 Men with Known or Suspected Carcinoma of the Prostate or Breast
Men with known or suspected prostate or breast cancer should not use AVEED [see Contraindications (4)].
17.3 Potential Adverse Reactions to Androgens
Patients should be informed that treatment with androgens may lead to adverse reactions which include:
- Changes in urinary habits, such as increased urination at night, trouble starting the urine stream, passing urine many times during the day, having an urge to go the bathroom right away, having a urine accident, or being unable to pass urine or weak urine flow
- Breathing disturbances, including those associated with sleep or excessive daytime sleepiness
- Too frequent or persistent erections of the penis
- Nausea, vomiting, changes in skin color, or ankle swelling
17.4 Patients Should Be Advised of the Following Instructions for Use
- Read the Medication Guide before starting AVEED therapy and reread the Guide before each injection.
- Adhere to all recommended monitoring.
- Report any changes in their state of health, such as changes in urinary habits, breathing, sleep, and mood.
MEDICATION GUIDE
AVEED® (Uh-Veed)
(testosterone undecanoate)
injection
Read this Medication Guide before you receive AVEED and before each injection. There may be new information. This Medication Guide does not take the place of talking with your doctor about your medical condition or your treatment.
What is the most important information I should know about AVEED?
AVEED may cause serious side effects, including:
- A serious lung problem. AVEED can cause a serious lung problem called a pulmonary oil microembolism (POME) reaction. POME is caused by tiny droplets of oil that have traveled to the lungs. Symptoms of a POME reaction may include:
o cough or urge to cough
o difficulty breathing
o sweating
o tightening of your throat
o chest pain
o dizziness
o fainting
- Serious allergic reactions (anaphylaxis). AVEED can cause a serious allergic reaction right after receiving the injection. Some of these allergic reactions may be life threatening.
These reactions can happen after you receive your first dose of AVEED or may happen after receiving more than 1 dose.
You may need emergency treatment in a hospital, especially if these symptoms get worse over the 24 hours after
your AVEED injection.
These side effects may happen during or right after each injection. To be sure that you are not having one
of these reactions:
o You need to stay in the doctor’s office, clinic, or hospital for 30 minutes after having your AVEED injection so
that your doctor can watch you for symptoms of POME or a serious allergic reaction.
o You can only get AVEED at your doctor’s office, clinic, or hospital.
AVEED is only available through a restricted program called the AVEED Risk Evaluation and Mitigation Strategy (REMS) Program. For more information about the AVEED REMS Program go to www.AveedREMS.com or call 1-855-755-0494.
What is AVEED?
AVEED is a prescription medicine that contains testosterone. AVEED is used to treat adult males who have low or no testosterone due to certain medical conditions.
AVEED is only for adult males who need testosterone replacement therapy and when the benefit of receiving AVEED is more than the risk of POME and anaphylaxis.
Your healthcare provider will test your blood before you start and while you are taking AVEED.
It is not known if AVEED is safe or effective to treat men who have low testosterone due to aging.
It is not known if AVEED is safe and effective for use in children younger than 18 years old. Improper use of AVEED may affect bone growth in children.
AVEED is a controlled substance (CIII) because it contains testosterone that can be a target for people who abuse prescription medicines.
AVEED is not meant for use in women.
Who should not receive AVEED?
Do not receive AVEED if you:
- have breast cancer
- have or might have prostate cancer
- are pregnant. AVEED may harm your unborn baby.
- are allergic to AVEED or to any of the ingredients in AVEED. See the end of this leaflet for a complete list of ingredients in AVEED.
Talk to your doctor before receiving this medicine if you have any of the above conditions.
What should I tell my doctor before receiving AVEED?
Before receiving AVEED, tell your doctor if you:
- have breast cancer
- have or might have prostate cancer
- have urinary problems due to an enlarged prostate
- have heart problems
- have liver or kidney problems
- have problems breathing while you sleep (sleep apnea)
- have any other medical conditions
Tell your doctor about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Receiving AVEED with certain other medicines can affect each other. Especially tell your doctor if you take:
- insulin
- medicines that decrease blood clotting
- corticosteroids
Ask your doctor or pharmacist for a list of these medicines, if you are not sure.
Know the medicines you take. Keep a list of your medicines and show them to your doctor and pharmacist when you get a new medicine.
How will I receive AVEED?
See “What is the most important information I should know about AVEED?”
Your doctor will inject AVEED deep into the muscle of your buttock. You will get 1 injection when you start, 1 injection 4 weeks later, and then 1 injection every 10 weeks.
Your doctor will test your blood before you receive and while you are receiving AVEED.
What are the possible side effects of AVEED?
AVEED can cause serious side effects including:
- see “What is the most important information I should know about AVEED?”
- if you already have enlargement of your prostate gland, your signs and symptoms can get worse while receiving AVEED. This can include:
o increased urination at night
o trouble starting your urine stream
o having to pass urine many times during the day
o having an urge that you have to go to the bathroom right away
o having a urine accident
o being unable to pass urine or weak urine flow
- changes in certain blood tests
- possible increased risk of prostate cancer. Your doctor should check you for prostate cancer or any other prostate problems before you receive and while you are receiving AVEED.
- blood clots in the legs or lungs. Signs and symptoms of a blood clot in your leg can include leg pain, swelling or redness. Signs and symptoms of a blood clot in your lungs can include difficulty breathing or chest pain.
- possible increased risk of heart attack or stroke.
- in large doses AVEED may lower your sperm count.
- liver problems. Symptoms of liver problems may include:
o nausea or vomiting
o yellowing of your skin or whites of your eyes
o dark urine
o pain on the right side of your stomach area (abdominal pain)
- swelling of your ankles, feet, or body, with or without heart failure. This may cause serious problems for people who have heart, kidney, or liver disease.
- enlarged or painful breasts.
- have problems breathing while you sleep (sleep apnea).
Call your doctor right away if you have any of the serious side effects listed above.
The most common side effects of AVEED include:
- acne
- pain at the injection site
- increased prostate specific antigen (a test used to screen for prostate cancer)
- increased estradiol level
- low testosterone level
- feeling tired
- irritability
- increased red blood cell count
- difficulty sleeping
- mood swings
Other side effects include more erections than are normal for you or erections that last for a long time.
Tell your doctor if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects with AVEED. For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
General information about AVEED
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide.
This Medication Guide summarizes the most important information about AVEED. If you would like more information, talk with your doctor. You can ask your doctor or nurse for information about AVEED that is written for health professionals. For more information, go to www.AVEEDUSA.com or call 1-800-462-3636.
What are the ingredients in AVEED?
Active ingredient: testosterone undecanoate
Inactive ingredients: benzyl benzoate, refined castor oil
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Manufactured for:
Endo USA
Malvern, PA 19355
© 2024 Endo, Inc. or one of its affiliates.
Revised: 03/2024