WARNING
WARNING:ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION;ACCIDENTAL INGESTION; NEONATAL OPIOID; WITHDRAWAL SYNDROME; and HEPATOTOXICITY
Addiction, Abuse, and Misuse
Hydrocodone bitartrate and acetaminophen tablets exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’srisk prior to prescribing hydrocodone bitartrate and acetaminophen tablets, andmonitor all patients regularly for the development of these behaviors orconditions [see WARNINGS].
Life-ThreateningRespiratory Depression
Serious, life-threatening, or fatal respiratory depression may occur with use of hydrocodone bitartrate and acetaminophen tablets. Monitor for respiratory depression, especially during initiation of hydrocodone bitartrate and acetaminophen tablets or following adose increase [see WARNINGS].
Accidental Ingestion
Accidental ingestion of even one dose of hydrocodone bitartrate and acetaminophen tablets, especially by children, can result in a fatal overdose of Hydrocodone bitartrate and acetaminophen tablets[see WARNINGS].
Neonatal Opioid Withdrawal Syndrome
Prolonged use of hydrocodone bitartrate and acetaminophen tablets during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized andtreated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in apregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [seeWARNINGS].
Hepatotoxicity
Acetaminophenhas been associated with cases of acute liver failure, at times resulting inliver transplant and death. Most of the cases of liver injury are associatedwith the use of acetaminophen at doses that exceed 4,000 milligrams per day,and often involve more than one acetaminophen-containing product (seeWARNINGS).
Risks from concomitant use with Benzodiazepines or other CNS Depressants
Concomitant use of opiods with benzodiazepines or other central nervous system (CNS) depressants including alcohol, may result in profound sedation, respiratory depression, coma, and death. [see WARNINGS, PRECAUTIONS; Drug interactions]
• Reserve concomitant prescribing of Hydrocodone bitartrate and acetaminophen tablets and benzodiazepines or other CNS depressants for use in patients for whom alternative treatment options are inadequate.
• Limit dosages and durations to the minimum required.
• Follow patients for signs and symptoms of respiratory depression and sedation.
DESCRIPTION
Hydrocodone bitartrate and acetaminophen is supplied in tablet form for oral administration.
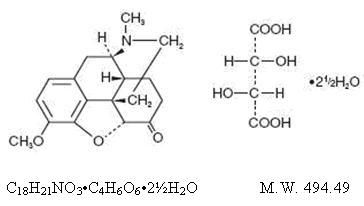
Hydrocodone bitartrate is an opioid analgesic and antitussive and occurs as fine, white crystals or as a crystalline powder. It is affected by light. The chemical name is: 4,5α-epoxy-3-methoxy-17-methylmorphinan-6-one tartrate (1:1) hydrate (2:5). It has the following structural formula:
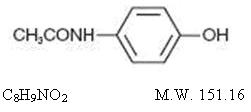
Acetaminophen, 4’-hydroxyacetanilide, a slightly bitter, white, odorless, crystalline powder, is a non-opiate, non-salicylate analgesic and antipyretic. It has the following structural formula:
Hydrocodone bitartrate and acetaminophen tablets USP, for oral administration, are available in a variety of strengths as described in the following table.
Each hydrocodone bitartrate and acetaminophen tablet contains:
|
Strength
|
Hydrocodone Bitartrate |
Acetaminophen |
|
5 mg/325 mg |
5 mg |
325 mg |
In addition each tablet contains the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, crospovidone, magnesium stearate, microcrystalline cellulose, povidone, pregelatinized starch and stearic acid.
Meets USP Dissolution Test 1.
CLINICAL PHARMACOLOGY
Hydrocodone is a semisynthetic narcotic analgesic and antitussive with multiple actions qualitatively similar to those of codeine. Most of these involve the central nervous system and smooth muscle. The precise mechanism of action of hydrocodone and other opiates is not known, although it is believed to relate to the existence of opiate receptors in the central nervous system. In addition to analgesia, narcotics may produce drowsiness, changes in mood and mental clouding.
The analgesic action of acetaminophen involves peripheral influences, but the specific mechanism is as yet undetermined. Antipyretic activity is mediated through hypothalamic heat regulating centers. Acetaminophen inhibits prostaglandin synthetase. Therapeutic doses of acetaminophen have negligible effects on the cardiovascular or respiratory systems; however, toxic doses may cause circulatory failure and rapid, shallow breathing.
Pharmacokinetics
The behavior of the individual components is described below.
Hydrocodone
Following a 10 mg oral dose of hydrocodone administered to five adult male subjects, the mean peak concentration was 23.6 ± 5.2 ng/mL. Maximum serum levels were achieved at 1.3 ± 0.3 hours and the half-life was determined to be 3.8 ± 0.3 hours. Hydrocodone exhibits a complex pattern of metabolism including O-demethylation, N-demethylation and 6-keto reduction to the corresponding 6-α- and 6-β-hydroxy-metabolites. See OVERDOSAGE for toxicity information.
Acetaminophen
Acetaminophen is rapidly absorbed from the gastrointestinal tract and is distributed throughout most body tissues. The plasma half-life is 1.25 to 3 hours, but may be increased by liver damage and following overdosage. Elimination of acetaminophen is principally by liver metabolism (conjugation) and subsequent renal excretion of metabolites. Approximately 85% of an oral dose appears in the urine within 24 hours of administration, most as the glucuronide conjugate, with small amounts of other conjugates and unchanged drug. See OVERDOSAGE for toxicity information.
INDICATIONS AND USAGE
Hydrocodone bitartrate and acetaminophentablets are indicated for the management of relief of moderate to moderatelysevere pain, pain severe enough to require an opioid analgesic and for whichalternative treatments are inadequate.
Limitations of Use
Because of the risks of addiction, abuse, andmisuse, with opioids, even at recommended doses [see WARNINGS], reserve hydrocodonebitartrate and acetaminophen tablets for use in patients for whom alternativetreatment options [e.g., non-opioid analgesics]
- •
- Have not been tolerated, or are not expected to be tolerated,
- •
- Have not provided adequate analgesia, or are not expected to provide adequate analgesia
CONTRAINDICATIONS
Hydrocodonebitartrate and acetaminophen tablets are contraindicated in patients with:
- •
- Significant respiratory depression [see WARNINGS]
- •
- Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment [see WARNINGS]
- •
- Hypersensitivity to hydrocodone or acetaminophen
- •
- Hypersensitive to other opioids which may exhibit cross-sensitivity to hydrocodone
WARNINGS
Addiction, Abuse, and Misuse
Hydrocodone bitartrate and acetaminophen tablet contains hydrocodone and acetaminophen a Schedule CII controlled substance. As an opioid, hydrocodone bitartrate andacetaminophen tablets exposes users to the risks of addiction, abuse, andmisuse [see DRUG ABUSE AND DEPENDENCE].
Although therisk of addiction in any individual is unknown, it can occur in patients appropriately prescribed hydrocodone bitartrate and acetaminophen tablets.Addiction can occur at recommended dosages and if the drug is misused orabused.
Assess eachpatient’s risk for opioid addiction, abuse, or misuse prior to prescribing hydrocodone bitartrate and acetaminophen tablets, and monitor all patients receiving hydrocodone bitartrate and acetaminophen tablets for the development of these behaviors or conditions. Risks are increased in patients with a personal or family historyof substance abuse (including drug or alcohol abuse or addiction) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the proper management of pain in any given patient. Patients at increased risk may be prescribed opioids such as hydrocodone bitartrate and acetaminophen tablets, but use in such patients necessitates intensive counseling about the risks andproperuse of hydrocodone bitartrate and acetaminophen tablets along with intensive monitoring for signs of addiction, abuse, and misuse.
Opioids are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing hydrocodone bitartrate and acetaminophen tablets. Strategies to reduce these risks includeprescribing the drug in the smallest appropriate quantity and advising thepatient on the proper disposal of unused drug [see PRECAUTIONS; Information for Patients]. Contact local state professional licensing board or statecontrolled substances authority for information on how to prevent and detectabuse or diversion of this product.
Hepatotoxicity
Acetaminophenhas been associated with cases of acute liver failure, at times resulting inliver transplant and death. Most of the cases of liver injury are associated withthe use of acetaminophen at doses that exceed 4,000 milligrams per day, andoften involve more than one acetaminophen-containing product. The excessiveintake of acetaminophen may be intentional to cause self-harm or unintentionalas patients attempt to obtain more pain relief or unknowingly take otheracetaminophen-containing products.
The riskof acute liver failure is higher in individuals who ingest alcohol while taking acetaminophen. Instruct patients to look for acetaminophen or APAP on package labels and not to use more than one product that contains acetaminophen. Instruct patients to seek medical attention immediately upon ingestion of more than 4,000 milligrams of acetaminophen per day, even if they feel well.
Life-Threatening Respiratory Depression
Serious, life-threatening, or fatal respiratory depression has been reported with theuse of opioids, even when used as recommended. Respiratory depression, if notimmediately recognized and treated, may lead to respiratory arrest and death.Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status [see OVERDOSAGE]. Carbon dioxide (CO2) retention from opioid-induced respiratory depression can exacerbate the sedating effects ofopioids.
While serious, life-threatening, or fatal respiratory depression can occur at anytime during the use of hydrocodone bitartrate and acetaminophen tablets, therisk is greatest during the initiation of therapy or following a dosageincrease. Monitor patients closely for respiratory depression, especiallywithin the first 24 to 72 hours of initiating therapy with and following dosage increases of hydrocodone bitartrate and acetaminophen tablets.
To reduce therisk of respiratory depression, proper dosing and titration of hydrocodonebitartrate and acetaminophen tablets are essential [see DOSAGE AND ADMINISTRATION]. Overestimating the hydrocodone bitartrate andacetaminophen tablets dosage when converting patients from another opioidproduct can result in a fatal overdose with the first dose.
Accidentalingestion of even one dose of hydrocodone bitartrate and acetaminophen tablets,especially by children, can result in respiratory depression and death due toan overdose of hydrocodoneand acetaminophen.
Neonatal Opioid Withdrawal Syndrome
Prolonged useof hydrocodone bitartrate and acetaminophen tablets during pregnancy can resultin withdrawal in the neonate. Neonatal opioid withdrawal syndrome, unlikeopioid withdrawal syndrome in adults, may be life-threatening if not recognizedand treated, and requires management according to protocols developed byneonatology experts. If opioid use is required for a prolonged period in apregnant woman, advise the patient of the risk of neonatal opioid withdrawalsyndrome and ensure that appropriate treatment will be available [seePRECAUTIONS;Information for Patients, Pregnancy].
Drug Interactions
Patientsreceiving other narcotic analgesics, antihistamines, antipsychotics, antianxietyagents, or other CNS depressants (including alcohol) concomitantly withhydrocodone bitartrate and acetaminophen tablets may exhibit an additive CNSdepression. When combined therapy is contemplated, the dose of one or bothagents should be reduced.
The use of MAO inhibitors or tricyclicantidepressants with hydrocodone preparations may increase the effect of eitherthe antidepressant or hydrocodone.
Drug/Laboratory Test Interactions
Acetaminophenmay produce false-positive test results for urinary 5-hydroxyindoleacetic acid.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Noadequate studies have been conducted in animals to determine whetherhydrocodone or acetaminophen have a potential for carcinogenesis, mutagenesis,or impairment of fertility.
Pregnancy
Teratogenic Effects
PregnancyCategory C
Thereare no adequate and well-controlled studies in pregnant women. Hydrocodone bitartrate and acetaminophen tablets should be used during pregnancy only ifthe potential benefit justifies the potential risk to the fetus.
Nonteratogenic Effects
Babies born to mothers who have been taking opioids regularly prior to delivery will be physically dependent. The withdrawal signs include irritability and excessive crying, tremors, hyperactive reflexes, increased respiratory rate, increased stools, sneezing, yawning, vomiting, and fever. The intensity of the syndrome does not always correlate with the duration of maternal opioid use ordose. There is no consensus on the best method of managing withdrawal.
Labor and Delivery
Aswith all narcotics, administration of this product to the mother shortly beforedelivery may result in some degree of respiratory depression in the newborn,especially if higher doses are used.
Nursing Mothers
Acetaminophenis excreted in breast milk in small amounts, but the significance of itseffects on nursing infants is not known. It is not known whether hydrocodone isexcreted in human milk. Because many drugs are excreted in human milk andbecause of the potential for serious adverse reactions in nursing infants fromhydrocodone and acetaminophen, a decision should be made whether to discontinuenursing or to discontinue the drug, taking into account the importance of thedrug to the mother.
Pediatric Use
Safetyand effectiveness in the pediatric population have not been established.
Geriatric Use
Clinicalstudies of hydrocodone bitartrate 5 mg and acetaminophen 500 mg did not includesufficient numbers of subjects aged 65 and over to determine whether theyrespond differently from younger subjects. Other reported clinical experiencehas not identified differences in responses between the elderly and youngerpatients. In general, dose selection for an elderly patient should be cautious,usually starting at the low end of the dosing range, reflecting the greaterfrequency of decreased hepatic, renal, or cardiac function, and of concomitantdisease or other drug therapy.
Hydrocodoneand the major metabolites of acetaminophen are known to be substantiallyexcreted by the kidney. Thus the risk of toxic reactions may be greater inpatients with impaired renal function due to the accumulation of the parentcompound and/or metabolites in the plasma. Because elderly patients are morelikely to have decreased renal function, care should be taken in doseselection, and it may be useful to monitor renal function.
Hydrocodonemay cause confusion and over-sedation in the elderly; elderly patientsgenerally should be started on low doses of hydrocodone bitartrate andacetaminophen tablets and observed closely.
Risks from Concomitant Use with Benzodiazepines or Other CNS Depressants
Profound sedation, respiratory depression, coma, and death may result from the concomitant use of Hydrocodone bitartrate and acetaminophen tablets with benzodiazepines or other CNS depressants (e.g., non-benzodiazepine sedatives/hypnotics, anxiolytics,tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other opioids, alcohol). Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate.
Observational studies have demonstrated that concomitant use of opioid analgesics and benzodiazepines increases the risk of drug-related mortality compared to use of opioid analgesics alone. Because of similar pharmacological properties, it is reasonable to expect similar risk with the concomitant use of other CNS depressant drugs with opioid analgesics [see PRECAUTIONS; Drug Interactions].
If the decision is made to prescribe a benzodiazepine or other CNS depressant concomitantly with an opioid analgesic, prescribe the lowest effective dosages and minimum durations of concomitant use. In patients already receiving an opioid analgesic, prescribe a lower initial dose of the benzodiazepine or other CNS depressant than indicated in the absence of an opioid, and titrate based on clinical response. If an opioid analgesic is initiated in a patient already taking a benzodiazepine or other CNS depressant, prescribe a lower initial dose of the opioid analgesic, and titrate based on clinical response. Follow patients closely for signs and symptoms of respiratory depression and sedation.
Advise both patients and caregivers about the risks of respiratory depression and sedation when Hydrocodone bitartrate and acetaminophen tablet is used with benzodiazepines or other CNS depressants (including alcohol and illicit drugs). Advice patients not to drive or operate heavy machinery until the effects of concomitant use of the benzodiazepine or other CNS depressant have been determined. Screen patients for risk of substance use disorders, including opioid abuse and misuse, and warn them of the risk for overdose and death associated with the use of additional CNS depressants including alcohol and illicit drugs [seePRECAUTIONS; Drug Interactions) and PRECAUTIONS; Information for Patients ].
Life-Threatening Respiratory Depression in Patients with Chronic Pulmonary Disease or in Elderly, Cachectic, or Debilitated Patients
The use of hydrocodone bitartrate and acetaminophen tablets in patients with acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipmentis contraindicated.
Patientswith Chronic Pulmonary Disease: Hydrocodonebitartrate and acetaminophen tablets-treated patients with significant chronicobstructive pulmonary disease or cor pulmonale, and those with a substantiallydecreased respiratory reserve, hypoxia, hypercapnia, or pre-existingrespiratory depression are at increased risk of decreased respiratory driveincluding apnea, even at recommended dosages of hydrocodone bitartrate andacetaminophen tablets [see WARNINGS].
Elderly,Cachetic, or Debilitated Patients: Life-threateningrespiratory depression is more likely to occur in elderly, cachectic, ordebilitated patients because they may have altered pharmacokinetics or alteredclearance compared to younger, healthier patients [see WARNINGS].
Monitor suchpatients closely, particularly when initiating and titrating hydrocodonebitartrate and acetaminophen tablets and when hydrocodone bitartrate andacetaminophen tablets is given concomitantly with other drugs that depressrespiration [see WARNINGS].Alternatively, consider the use ofnon-opioid analgesics in these patients.
Adrenal Insufficiency
Cases of adrenal insufficiency have beenreported with opioid use, more often following greater than 1 month of use.Presentation of adrenal insufficiency may include non-specific symptoms andsigns including nausea, vomiting, anorexia, fatigue, weakness, dizziness, andlow blood pressure. If adrenal insufficiency is suspected, confirm thediagnosis with diagnostic testing as soon as possible. If adrenal insufficiencyis diagnosed, treat with physiologic replacement doses of corticosteroids. Weanthe patient off of the opioid to allow adrenal function to recover and continuecorticosteroid treatment until adrenal function recovers. Other opioids may betried as some cases reported use of a different opioid without recurrence ofadrenal insufficiency. The information available does not identify anyparticular opioids as being more likely to be associated with adrenal insufficiency.
PRECAUTIONS
General
Special Risk Patients
As with any narcotic analgesic agent, hydrocodonebitartrate and acetaminophen tablets should be used with caution in elderly ordebilitated patients and those with severe impairment of hepatic or renalfunction, hypothyroidism, Addison’s disease, prostatic hypertrophy or urethralstricture. The usual precautions should be observed and the possibility of respiratorydepression should be kept in mind.
Cough Reflex
Hydrocodone suppresses the cough reflex;as with all narcotics, caution should be exercised when hydrocodone bitartrateand acetaminophen tablets are used postoperatively and in patients with pulmonarydisease.
Information for Patients/Caregivers
Addiction, Abuse, and Misuse
Informpatients that the use of hydrocodone bitartrate and acetaminophen tablets, even when taken as recommended, can result in addiction, abuse, and misuse, which can lead to overdose and death [see WARNINGS]. Instruct patients not to share hydrocodone bitartrate and acetaminophen tablets with others and to take steps to protect hydrocodone bitartrate and acetaminophen tablets from theft ormisuse.
Life-Threatening Respiratory Depression
Informpatients of the risk of life-threatening respiratory depression, including information that the risk is greatest when starting hydrocodone bitartrate andacetaminophen tablets or when the dosage is increased, and that it can occureven at recommended dosages [see WARNINGS]. Advise patients how to recognize respiratory depression and to seek medical attention if breathing difficulties develop.
Accidental Ingestion
Inform patients that accidental ingestion, especially by children, may result inrespiratory depression or death [see WARNINGS]. Instruct patients totake steps to store hydrocodone bitartrate and acetaminophen tablets securely.Opioids are sought by drug abusers and people with addiction disorders and aresubject to criminal diversion. Consider these risks when prescribing ordispensing hydrocodone bitartrate and acetaminophen tablets. Strategies toreduce these risks include prescribing the drug in the smallest appropriatequantity and advising the patient on the proper disposal of unused drug [see PRECAUTIONS; Information for Patients]. Contact local state professional licensing boardor state controlled substances authority for information on how to prevent anddetect abuse or diversion of this product.
Interactions with Benzodiazepines and Other CNS Depressants
Inform patients and caregivers that potentially fatal additive effects may occur if Hydrocodone bitartrate and acetaminophen tablets is used with benzodiazepines or other CNS depressants, including alcohol, and not to use these concomitantly unless supervised by a health care provider [see WARNINGS and PRECAUTIONS; Drug Interactions].
Serotonin Syndrome
Inform patients that hydrocodone bitartrate and acetaminophen tablets could cause a rare but potentially life-threatening condition resulting from concomitant administration of serotonergic drugs. Warn patients of the symptoms ofserotonin syndrome and to seek medical attention right away if symptoms develop. Instruct patients to inform their physicians if they are taking, orplan to take serotonergic medications [see PRECAUTIONS; Error! Hyperlink reference not valid.].
Adrenal Insufficiency
Inform patients that hydrocodone bitartrate and acetaminophen tablets could cause adrenal insufficiency, a potentially life-threatening condition. Adrenal insufficiency may present with non-specific symptoms and signs such as nausea,vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure.Advise patients to seek medical attention if they experience a constellation ofthese symptoms [seeWARNINGS].
Pregnancy
Neonatal Opioid Withdrawal Syndrome
Inform patients that prolonged use of hydrocodone bitartrate and acetaminophen tablets during pregnancy can result in neonatal opioid withdrawal syndrome, which maybe life-threatening if not recognized and treated [see WARNINGS, PRECAUTIONS;Error! Hyperlink reference not valid.] Embryo-Fetal Toxicity
Inform female patients of reproductive potential that hydrocodone bitartrate andacetaminophen can cause fetal harm and to inform the prescriber of a known orsuspected pregnancy [see PRECAUTIONS; Error! Hyperlink reference not valid.].
Lactation
Advise nursing mothers to monitor infants for increased sleepiness (more than usual), breathing difficulties, or limpness. Instruct nursing mothers to seek immediate medical care if they notice these signs [see PRECAUTIONS; Error! Hyperlink reference not valid.].
Disposal of Unused Hydrocodone Bitartrate and Acetaminophen Tablets
Advise patients on the proper disposal of unused drug [see PRECAUTIONS; Information for Patients/Caregivers] by contacting local state professional licensing board orstate controlled substances authority for information on how to prevent anddetect abuse or diversion of this product.
Drug Interactions
Patients receiving other narcotic analgesics, antihistamines, antipsychotics, antianxiety agents, or other CNS depressants (including alcohol) concomitantlywith hydrocodone bitartrate and acetaminophen tablets may exhibit an additiveCNS depression. When combined therapy is contemplated, the dose of one or bothagents should be reduced.
The use of MAO inhibitors or tricyclic antidepressants with hydrocodone preparations may increase the effect of either the antidepressant or hydrocodone.
Hydrocodone bitartrate and acetaminophen tablets contains hydrocodone and acetaminophen, asubstance with a high potential for abuse similar to other opioids including withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity (e.g., naloxone, nalmefene), mixedagonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine), orpartial agonists (buprenorphine). Physical dependence may not occur to aclinically significant degree until after several days to weeks of continuedopioid usage. Hydrocodone bitartrate and acetaminophen tablets can be abusedand is subject to misuse, addiction, and criminal diversion [seeWARNINGS].
Benzodiazepines and other Central Nervous System (CNS) Depressants
Due to additive pharmacologic effect, the concomitant use of benzodiazepines or other CNS depressants such as alcohol, other sedatives/hypnotics, anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, and other opioids, can increases the risk of respiratory depression, profound sedation, coma, and death. Reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate. Limit dosages and durations to the minimum required. Follow patients closely for signs of respiratory depression and sedation [see WARNINGS].
Serotonergic Drugs
The concomitantuse of opioids with other drugs that affect the serotonergic neurotransmitter system, such as selective serotonin reuptake inhibitors (SSRIs), serotonin andnorepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs),triptans, 5-HT3 receptor antagonists, drugs that effect theserotonin neurotransmitter system (e.g., mirtazapine, trazodone, tramadol), andmonoamine oxidase (MAO) inhibitors (those intended to treat psychiatricdisorders and also others, such as linezolid and intravenous methylene blue),has resulted in serotonin syndrome [see PRECAUTIONS; Information for Patients/Caregivers].
If concomitant use is warranted, carefully observe the patient, particularly during treatment initiation and dose adjustment. Discontinue hydrocodone bitartrateand acetaminophen tablets if serotonin syndrome is suspected.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Infertility
Chronic useof opioids may cause reduced fertility in females and males of reproductivepotential. It is not known whether these effects on fertility are reversible[see ADVERSE REACTIONS].
Pregnancy
Fetal/Neonatal Adverse Reactions
Prolonged useof opioid analgesics during pregnancy for medical or nonmedical purposes canresult in physical dependence in the neonate and neonatal opioid withdrawalsyndrome shortly after birth.
Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormalsleep pattern, high pitched cry, tremor, vomiting, diarrhea and failure to gainweight. The onset, duration, and severity of neonatal opioid withdrawalsyndrome vary based on the specific opioid used, duration of use, timing andamount of last maternal use, and rate of elimination of the drug by thenewborn. Observe newborns for symptoms of neonatal opioid withdrawal syndromeand manage accordingly [see WARNINGS].
Labor or Delivery
Opioids cross the placenta and may produce respiratory depression and psycho-physiologic effects in neonates. An opioid antagonist, such as naloxone, must be availablefor reversal of opioid-induced respiratory depression in the neonate. Hydrocodone bitartrate and acetaminophen tablets is not recommended for use inpregnant women during or immediately prior to labor, when other analgesic techniques are more appropriate. Opioid analgesics, including hydrocodonebitartrate and acetaminophen, can prolong labor through actions which temporarily reduce the strength, duration, and frequency of uterine contractions. However, this effect is not consistent and may be offset by anincreased rate of cervical dilation, which tends to shorten labor. Monitorneonates exposed to opioid analgesics during labor for signs of excess sedationand respiratory depression.
Nursing Mothers
The developmental and health benefits of breastfeeding should be considered alongwith the mother’s clinical need for hydrocodone bitartrate and acetaminophen and any potential adverse effects on the breastfed infant from hydrocodone bitartrate and acetaminophen tablets or from the underlying maternal condition.Infants exposed to hydrocodone bitartrate and acetaminophen through breast milkshould be monitored for excess sedation and respiratory depression. Withdrawal symptoms can occur in breastfed infants when maternal administration of anopioid analgesic is stopped, or when breast-feeding is stopped.
Geriatric Use
Elderly patients (aged 65 years or older) may have increased sensitivity to hydrocodone bitartrate and acetaminophen tablets. In general, use caution when selecting adosage for an elderly patient, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy. Respiratory depression is the chief risk for elderly patients treated with opioids, and hasoccurred after large initial doses were administered to patients who were not opioid-tolerant or when opioids were co-administered with other agents that depress respiration. Titrate the dosage of hydrocodone bitartrate andacetaminophen tablets slowly in geriatric patients [see WARNINGS].
ADVERSE REACTIONS
The most frequently reported adverse reactions include: lightheadedness, dizziness, sedation, nausea and vomiting. These effects seem to be more prominent in ambulatory than in nonambulatory patients and some of these adverse reactions may be alleviated if the patient lies down.
Other adverse reactions include
Central Nervous System
Drowsiness, mental clouding, lethargy, impairment of mental and physical performance, anxiety, fear, dysphoria, psychic dependence, mood changes.
Gastrointestinal System
Prolonged administration of hydrocodone bitartrate and acetaminophen tablets may produce constipation.
Genitourinary System
Ureteral spasm, spasm of vesical sphincters and urinary retention have been reported with opiates.
Respiratory Depression
Hydrocodone bitartrate may produce dose-related respiratory depression by acting directly on the brain stem respiratory center. (see OVERDOSAGE).
Special Senses
Cases of hearing impairment or permanent loss have been reported predominantly in patients with chronic overdose.
Dermatological
Skin rash, pruritus.
The following adverse drug events may be borne in mind as potential effects of acetaminophen: allergic reactions, rash, thrombocytopenia, agranulocytosis.
Potential effects of high dosage are listed in the OVERDOSAGE section.
Postmarketing Experience
- •
- serotonin syndrome
- •
- adrenal insufficiency
Androgen Deficiency
Chronic useof opioids may influence the hypothalamic-pituitary-gonadal axis, leading toandrogen deficiency that may manifest as symptoms of hypogonadism, such asimpotence, erectile dysfunction, or amenorrhea. The causal role of opioids inthe syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date. Patients presenting with symptoms of androgen deficiency should undergo laboratory evaluation.
DRUG ABUSE AND DEPENDENCE
Controlled Substance
Hydrocodone bitartrate and acetaminophen tablets contains hydrocodone and acetaminophen, aSchedule CII controlled substance.
Abuse
Hydrocodone bitartrate and acetaminophen tablets contains hydrocodone and acetaminophen, asubstance with a high potential for abuse similar to other opioids including withdrawal also may be precipitated through the administration of drugs withopioid antagonist activity (e.g., naloxone, nalmefene), mixedagonist/antagonist analgesics (pentazocine, butorphanol, nalbuphine), orpartial agonists (buprenorphine). Physical dependence may not occur to aclinically significant degree until after several days to weeks of continuedopioid usage. Hydrocodone bitartrate and acetaminophen tablets can be abusedand is subject to misuse, addiction, and criminal diversion [see WARNINGS].
All patients treated with opioids require careful monitoring for signs of abuse and addiction, since use of opioid analgesic products carries the risk of addiction even under appropriate medical use.
Prescription drug abuse is the intentional non-therapeutic use of a prescription drug, evenonce, for its rewarding psychological or physiological effects.
Drug addiction is a cluster of behavioral, cognitive, and physiological phenomenathat develop after repeated substance use and includes: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal.
“Drug-seeking”behavior is very common in persons with substance use disorders. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing, or referral, repeated “loss” of prescriptions, tampering with prescriptions and reluctance to provide priormedical records or contact information for other treating health careprovider(s). “Doctor shopping” (visiting multiple prescribers) to obtainadditional prescriptions is common among drug abusers and people suffering from untreated addiction. Preoccupation with achieving adequate pain relief can beappropriate behavior in a patient with poor pain control.
Abuse and addiction are separate and distinct from physical dependence and tolerance.Health care providers should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. Inaddition, abuse of opioids can occur in the absence of true addiction.
Hydrocodone bitartrate and acetaminophen tablets, like other opioids, can be diverted fornon-medical use into illicit channels of distribution. Careful record-keepingof prescribing information, including quantity, frequency, and renewalrequests, as required by state and federal law, is strongly advised. Properassessment of the patient, proper prescribing practices, periodic re-evaluationof therapy, and proper dispensing and storage are appropriate measures thathelp to limit abuse of opioid drugs.
Risks Specific to Abuse of Hydrocodone Bitartrate and Acetaminophen Tablets
Hydrocodone
Serious overdose with hydrocodone is characterized by respiratory depression (adecrease in respiratory rate and/or tidal volume, Cheyne-Stokes respiration,cyanosis), extreme somnolence progressing to stupor or coma, skeletal muscleflaccidity, cold and clammy skin, and sometimes bradycardia and hypotension. Insevere overdosage, apnea, circulatory collapse, cardiac arrest and death mayoccur.
Acetaminophen
In acetaminophen overdosage: dose-dependent, potentially fatal hepatic necrosis isthe most serious adverse effect. Renal tubular necrosis, hypoglycemic coma, andcoagulation defects may also occur.
Early symptoms following a potentially hepatotoxic overdose may include: nausea,vomiting, diaphoresis and general malaise. Clinical and laboratory evidence ofhepatic toxicity may not be apparent until 48 to 72 hours post-ingestion.
Treatment
A single or multiple drug overdose with hydrocodone and acetaminophen is a potentially lethal polydrug overdose, and consultation with a regional poison control center is recommended. Immediate treatment includes support of cardiorespiratory function and measures to reduce drug absorption. Oxygen, intravenous fluids, vasopressors, and other supportive measures should beemployed as indicated. Assisted or controlled ventilation should also beconsidered.
For hydrocodone overdose, primary attention should be given to the reestablishment of adequate respiratory exchange through provision of a patent airway and the institution of assisted or controlled ventilation. The narcotic antagonistnaloxone hydrochloride is a specific antidote against respiratory depressionwhich may result from overdosage or unusual sensitivity to narcotics, includinghydrocodone. Since the duration of action of hydrocodone may exceed that of theantagonist, the patient should be kept under continued surveillance, andrepeated doses of the antagonist should be administered as needed to maintainadequate respiration. A narcotic antagonist should not be administered in theabsence of clinically significant respiratory or cardiovascular depression.
Gastricdecontamination with activated charcoal should be administered just prior toN-acetylcysteine (NAC) to decrease systemic absorption if acetaminophen isknown or suspected to have occurred within a few hours of presentation. Serumacetaminophen levels should be obtained immediately if the patient presents 4hours or more after ingestion to assess potential risk of hepatotoxicity;acetaminophen levels drawn less than 4 hours post-ingestion may be misleading.To obtain the best possible outcome, NAC should be administered as soon aspossible where impending or evolving liver injury is suspected. Intravenous NACmay be administered when circumstances preclude oral administration.
Vigoroussupportive therapy is required in severe intoxication. Procedures to limit thecontinuing absorption of the drug must be readily performed since the hepaticinjury is dose-dependent and occurs early in the course of intoxication.
Dependence
Bothtolerance and physical dependence can develop during chronic opioid therapy.Tolerance is the need for increasing doses of opioids to maintain a definedeffect such as analgesia (in the absence of disease progression or otherexternal factors). Tolerance may occur to both the desired and undesiredeffects of drugs, and may develop at different rates for different effects.Physical dependence results in withdrawal symptoms after abrupt discontinuationor a significant dosage reduction of a drug. Withdrawal also may beprecipitated through the administration of drugs with opioid antagonistactivity (e.g., naloxone, nalmefene), mixed agonist/antagonist analgesics(pentazocine, butorphanol, nalbuphine), or partial agonists (buprenorphine).Physical dependence may not occur to a clinically significant degree untilafter several days to weeks of continued opioid usage.
Hydrocodonebitartrate and acetaminophen tablets should not be abruptly discontinued [see DOSAGE AND ADMINISTRATION]. If hydrocodone bitartrate and acetaminophentablets is abruptly discontinued in a physically dependent patient, awithdrawal syndrome may occur. Some or all of the following can characterizethis syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration,chills, myalgia, and mydriasis. Other signs and symptoms also may develop,including: irritability, anxiety, backache, joint pain, weakness, abdominalcramps, insomnia, nausea, anorexia, vomiting, diarrhea, or increased bloodpressure, respiratory rate, or heart rate.
Infants bornto mothers physically dependent on opioids will also be physically dependentand may exhibit respiratory difficulties and withdrawal signs [see PRECAUTIONS;Error! Hyperlink reference not valid.].
OVERDOSAGE
Clinical Presentation
Acuteoverdose with hydrocodone bitartrate and acetaminophen tablets can bemanifested by respiratory depression, somnolence progressing to stupor or coma,skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and, insome cases, pulmonary edema, bradycardia, hypotension, partial or completeairway obstruction, atypical snoring, and death. Marked mydriasis rather thanmiosis may be seen with hypoxia in overdose situations.
Treatment of Overdose
In case ofoverdose, priorities are the reestablishment of a patent and protected airwayand institution of assisted or controlled ventilation, if needed. Employ othersupportive measures (including oxygen and vasopressors) in the management ofcirculatory shock and pulmonary edema as indicated. Cardiac arrest orarrhythmias will require advanced life-support techniques.
The opioidantagonists, naloxone or nalmefene, are specific antidotes to respiratorydepression resulting from opioid overdose. For clinically significantrespiratory or circulatory depression secondary to hydrocodone bitartrate andacetaminophen tablets overdose, administer an opioid antagonist. Opioidantagonists should not be administered in the absence of clinically significantrespiratory or circulatory depression secondary to hydrocodone bitartrate andacetaminophen tablets overdose.
Because theduration of opioid reversal is expected to be less than the duration of actionof hydrocodone bitartrate and acetaminophen tablets in hydrocodone bitartrateand acetaminophen tablets, carefully monitor the patient until spontaneousrespiration is reliably re-established. If the response to an opioid antagonistis suboptimal or only brief in nature, administer additional antagonist asdirected by the product’s prescribing information.
In anindividual physically dependent on opioids, administration of the recommendedusual dosage of the antagonist will precipitate an acute withdrawal syndrome.The severity of the withdrawal symptoms experienced will depend on the degreeof physical dependence and the dose of the antagonist administered. If adecision is made to treat serious respiratory depression in the physicallydependent patient, administration of the antagonist should be begun with careand by titration with smaller than usual doses of the antagonist.
DOSAGE AND ADMINISTRATION
Important Dosage and Administration Instructions
Initiate thedosing regimen for each patient individually, taking into account the patient'sseverity of pain, patient response, prior analgesic treatment experience, andrisk factors for addiction, abuse, and misuse [see WARNINGS].
Monitorpatients closely for respiratory depression, especially within the first 24 to 72hours of initiating therapy and following dosage increases with hydrocodonebitartrate and acetaminophen tablets and adjust the dosage accordingly [see WARNINGS].
Dosage should be adjusted according tothe severity of the pain and the response of the patient. However, it should bekept in mind that tolerance to hydrocodone can develop with continued use andthat the incidence of untoward effects is dose related.
Initial Dosage Treatment with Hydrocodone Bitartrate and Acetaminophen Tablets
The usual adult dosageis one tablet every four to six hours as needed for pain. The total dailydosage should not exceed 6 tablets.
|
5 mg/325 mg |
The usual adult dosage is one or two tablets every four to six hours as needed for pain. |
|
7.5 mg/325 mg |
The usual adult dosage is one tablet every four to six hours as needed for pain. The total daily dosage should not exceed 6 tablets. |
|
10 mg/325 mg |
The usual adult dosage is one tablet every four to six hours as needed for pain. The total daily dosage should not exceed 6 tablets. |
Titrationand Maintenance of Therapy
Individually titrate hydrocodonebitartrate and acetaminophen tablets to a dose that provides adequate analgesiaand minimizes adverse reactions. Continually reevaluate patients receiving hydrocodonebitartrate and acetaminophen tablets to assess the maintenance of pain controland the relative incidence of adverse reactions, as well as monitoring for thedevelopment of addiction, abuse, or misuse [see WARNINGS]. Frequentcommunication is important among the prescriber, other members of thehealthcare team, the patient, and the caregiver/family during periods ofchanging analgesic requirements, including initial titration.
If the levelof pain increases after dosage stabilization, attempt to identify the source ofincreased pain before increasing the hydrocodone bitartrate and acetaminophentablets dosage. If unacceptable opioid-related adverse reactions are observed,consider reducing the dosage. Adjust the dosage to obtain an appropriatebalance between management of pain and opioid-related adverse reactions.
Discontinuation of Hydrocodone Bitartrate and Acetaminophen Tablets
When apatient who has been taking hydrocodone bitartrate and acetaminophen tabletsregularly and may be physically dependent no longer requires therapy with hydrocodonebitartrate and acetaminophen tablets, use a gradual downward titration of thedosage to prevent signs and symptoms of withdrawal. Do not stop hydrocodonebitartrate and acetaminophen tablets abruptly [see WARNINGS, DRUG ABUSE ANDDEPENDENCE].
HOW SUPPLIED
Hydrocodone Bitartrate and Acetaminophen Tablets USP are available in the following strengths:
Hydrocodone Bitartrate and Acetaminophen Tablet USP, 10 mg/325 mg is available as white to off-white, oval shaped tablets, debossed with “U03” on one side and break-line on the other side. Each tablet contains 10 mg hydrocodone bitartrate and 325 mg acetaminophen.
Bottles of 12 NDC 63187-778-12
Bottles of 15 NDC 63187-778-15
Bottles of 20 NDC 63187-778-20
Bottles of 30 NDC 63187-778-30
Bottles of 60 NDC 63187-778-60
Bottles of 90 NDC 63187-778-90
Storage: Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
Dispense in a tight, light-resistant container as defined in the USP with a child-resistant closure. Keep this and all medication out of the reach of children.
A Schedule C-II controlled drug substance.
Dispense with Medication Guide available at www.aurobindousa.com/product-medication-guides
Manufactured by:
Aurolife Pharma LLC
Dayton, NJ 08810
Manufactured for:
Aurobindo Pharma USA, Inc.
Dayton, NJ 08810
Repackaged by:
Proficient Rx LP.
Thousand Oaks, CA 91320
Revised: 09/2016
MEDICATION GUIDE
Hydrocodone Bitartrate and Acetaminophen Tablets, USP CII
HIGH-droe-KOE-dohnby-TAR-trate/ass-eet-ah-MEE-noe-fen
Hydrocodone Bitartrate and Acetaminophen Tablets are:
- •
- A strong prescription pain medicine that contains an opioid (narcotic) that is used for the management of relief of moderate to moderately severe pain, pain severe enough to require an opioid analgesic and for which alternative treatments are inadequate or when non-opioid pain medicines do not treat your pain well enough or you cannot tolerate them.
- •
- An opioid pain medicine that can put you at risk for overdose and death. Even if you take your dose correctly as prescribed you are at risk for opioid addiction, abuse, and misuse that can lead to death.
Important information about Hydrocodone Bitartrate and Acetaminophen Tablets:
- •
- Get emergency help right away if you take too much hydrocodone bitartrate and acetaminophen tablets (overdose). When you first start taking hydrocodone bitartrate and acetaminophen tablets, when your dose is changed, or if you take too much (overdose), serious or life-threatening breathing problems that can lead to death may occur.
- •
- Taking hydrocodone bitartrate and acetaminophen tablets with other opioid medicines,benzodiazepines, alcohol, or other central nervous system depressants (including street drugs) can cause severe drowsiness, decreased awareness, breathing problems, coma and death.
- •
- Never give anyone else your hydrocodone bitartrate and acetaminophen tablets. They could die from taking it. Store hydrocodone bitartrate and acetaminophen tablets away from children and in a safe place to prevent stealing or abuse. Selling or giving away hydrocodone bitartrate and acetaminophen tablets is against the law.
Do not take Hydrocodone Bitartrate and Acetaminophen Tablets if you have:
- •
- acute or severe bronchial asthma, trouble breathing, or other lung problems.
- •
- a bowel blockage or have narrowing of the stomach or intestines.
- •
- significant respiratory depression
- •
- severe impairment of hepatic or renal function, hypothyroidism, Addison’s disease, prostatic hypertrophy or urethral stricture
Before taking Hydrocodone Bitartrate and Acetaminophen Tablets, tell your healthcareprovider if you have a history of:
• head injury, seizures
• liver, kidney, thyroid problems
• problems urinating
• pancreas or gallbladder problems
• abuse of street or prescription drugs, alcohol addiction, or mental health problems.
Tell your healthcare provider if you are:
- •
- pregnant or planning to become pregnant. Prolonged use of hydrocodone bitartrate and acetaminophen tablets during pregnancy can cause withdrawal symptoms in your newborn baby that could be life-threatening if not recognized and treated.
- •
- breastfeeding. Hydrocodone bitartrate and acetaminophen tablets passes into breast milk and may harm your baby.
- •
- taking prescription or over-the-counter medicines, vitamins, or herbal supplements. Taking hydrocodone bitartrate and acetaminophen tablets with certain other medicines can cause serious side effects that could lead to death.
Whentaking Hydrocodone Bitartrate and Acetaminophen Tablets:
- •
- Do not change your dose. Take hydrocodone bitartrate and acetaminophen tablets exactly as prescribed by your healthcare provider.
- •
- The usual adult dosage is one tablet every four to six hours as needed for pain. The total daily dosage should not exceed 6 tablets. Do not take more than your prescribed dose. If you miss a dose, take your next dose at your usual time.
- •
- Call your healthcare provider if the dose you are taking does not control your pain.
- •
- If you have been taking hydrocodone bitartrate and acetaminophen tablets regularly, do not stop taking hydrocodone bitartrate and acetaminophen tablets without talking to your healthcare provider.
- •
- After you stop taking hydrocodone bitartrate and acetaminophen tablets, contact local state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product.
While taking Hydrocodone Bitartrate and Acetaminophen Tablets DO NOT:
- •
- Drive or operate heavy machinery, until you know how hydrocodone bitartrate and acetaminophen tablets affects you. Hydrocodone bitartrate and acetaminophen tablets can make you sleepy, dizzy, or lightheaded.
- •
- Drink alcohol or use prescription or over-the-counter medicines that contain alcohol. Using products containing alcohol during treatment with hydrocodone bitartrate and acetaminophen tablets may cause you to overdose and die.
The possible side effects of hydrocodone Bitartrate and Acetaminophen Tablets:
- •
- constipation, nausea, sleepiness, vomiting, tiredness, headache, dizziness, abdominal pain. Call your healthcare provider if you have any of these symptoms and they are severe.
Get emergency medical help if you have:
- •
- trouble breathing, shortness of breath, fast heartbeat, chest pain, swelling of your face, tongue, or throat, extreme drowsiness, light-headedness when changing positions, feeling faint, agitation, high body temperature, trouble walking, stiff muscles, or mental changes such as confusion.
General Information about Hydrocodone Bitartrate and Acetaminophen Tablets
Medicinesare sometimes prescribed for purposes other than those listed in a MedicationGuide. Do not use hydrocodonebitartrate and acetaminophen tablets for a conditionfor which it was not prescribed. Do not give hydrocodone bitartrate andacetaminophen tablets to other people even if theyhave the same condition, they may harm them.
These are notall the possible side effects of hydrocodone bitartrate and acetaminophentablets. Call your doctor for medical advice about side effects. You may alsorequest medical information or to report suspected adverse reactions, contactAurobindo Pharma USA, Inc. at 1-866-850-2876 or FDA at 1-800-FDA-1088. Formore information go to dailymed.nlm.nih.gov
What are the ingredients in Hydrocodone Bitartrate andAcetaminophen Tablets?
Active Ingredients: hydrocodone bitartrate and acetaminophen
Inactive ingredients: colloidal silicon dioxide, croscarmellose sodium,crospovidone, magnesium stearate, microcrystalline cellulose, povidone,pregelatinized starch and stearic acid.
ThisMedication Guide has been approved by the U.S. Food and Drug Administration.
Manufacturedby:
AurolifePharma LLC
Dayton, NJ08810
Manufacturedfor:
AurobindoPharma USA, Inc.
Dayton, NJ 08810
Repackaged by:
Proficient Rx LP.
Thousand Oaks, CA 91320
Revised:09/2016