INVIRASE- saquinavir mesylate tablet, film coated
Genentech, Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use INVIRASE safely and effectively. See full prescribing information for INVIRASE.
INVIRASE® (saquinavir mesylate) tablets, for oral use Initial U.S. Approval: 1995 INDICATIONS AND USAGEINVIRASE is an HIV-1 protease inhibitor indicated for the treatment of HIV-1 infection in combination with ritonavir and other antiretroviral agents in adults (over the age of 16 years). (1) DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONSThe most common adverse reactions are nausea, vomiting, diarrhea, fatigue, pneumonia, lipodystrophy and abdominal pain. (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide. Revised: 9/2020 |
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
INVIRASE in combination with ritonavir and other antiretroviral agents is indicated for the treatment of HIV-1 infection in adults (over the age of 16 years).
The following points should be considered when initiating therapy with INVIRASE/ritonavir:
- –
- The twice daily administration of INVIRASE in combination with ritonavir is supported by safety data from the MaxCmin 1 trial [see Adverse Reactions (6.1)] and pharmacokinetic data [see Clinical Pharmacology (12.3)].
- –
- The efficacy of INVIRASE with ritonavir has not been compared against the efficacy of antiretroviral regimens currently considered standard of care.
- –
- The number of baseline primary protease inhibitor mutations affects the virologic response to INVIRASE/ritonavir.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose
INVIRASE must be used in combination with ritonavir because ritonavir significantly inhibits saquinavir's metabolism to provide increased plasma saquinavir levels.
Cobicistat is not interchangeable with ritonavir to increase systemic exposure of saquinavir [see Warnings and Precautions (5.1)].
- The standard recommended dose of INVIRASE is 1,000 mg twice daily in combination with ritonavir 100 mg twice daily.
- For treatment-naïve patients initiating treatment with INVIRASE/ritonavir, the recommended starting dose of INVIRASE is 500 mg twice daily with ritonavir 100 mg twice daily for the first 7 days of treatment. After 7 days, the recommended dose of INVIRASE is 1,000 mg twice daily with ritonavir 100 mg twice daily [see Warnings and Precautions (5.4) and Clinical Pharmacology (12.2)].
- Patients switching immediately (no washout period) from treatment with another ritonavir containing regimen or from a non-nucleoside reverse transcriptase inhibitor (NNRTI) based regimen (not including delavirdine, rilpivirine) should initiate and continue INVIRASE/ritonavir at the standard recommended dose of 1,000 mg twice daily with ritonavir 100 mg twice daily. For patients switching from a regimen containing delavirdine, the recommended dose is 500 mg twice daily with ritonavir 100 mg twice daily for the first 7 days of treatment [see Warnings and Precautions (5.4) and Drug Interactions (7.3)].
- Ritonavir should be taken at the same time as INVIRASE.
- INVIRASE and ritonavir should be taken within 2 hours after a meal.
- For patients already taking ritonavir 100 mg twice daily as part of their antiretroviral regimen, no additional ritonavir is needed.
- Pediatric dose recommendations that are both reliably effective and below thresholds of concern for QT and PR interval prolongation could not be determined.
3 DOSAGE FORMS AND STRENGTHS
Tablets: 500-mg light orange to greyish or brownish orange, oval cylindrical, biconvex film-coated with ROCHE and SQV 500 imprinted on the tablet face
4 CONTRAINDICATIONS
INVIRASE/ritonavir is contraindicated in patients with congenital long QT syndrome, those with refractory hypokalemia or hypomagnesemia, and in combination with drugs that both increase saquinavir plasma concentrations and prolong the QT interval [see Warnings and Precautions (5.4) and Clinical Pharmacology (12.2)].
INVIRASE/ritonavir is contraindicated in patients with complete atrioventricular (AV) block without implanted pacemakers, or patients who are at high risk of complete AV block [see Warnings and Precautions (5.3)].
INVIRASE/ritonavir is contraindicated in patients with clinically significant hypersensitivity (e.g., anaphylactic reaction, Stevens-Johnson syndrome) to saquinavir, saquinavir mesylate, or any of its ingredients.
INVIRASE/ ritonavir is contraindicated in patients with severe hepatic impairment.
INVIRASE/ritonavir is contraindicated with drugs that are CYP3A substrates for which increased plasma levels may result in serious or life-threatening reactions [see Warnings and Precautions (5.2), Drug Interactions (7) and Clinical Pharmacology (12.3)].
INVIRASE/ritonavir is contraindicated in patients receiving the following co-administered drugs; however, it should be noted that this list is not intended to be exhaustive [see Drug Interactions (7) and Clinical Pharmacology (12.3)]
- -
- Alpha 1-adrenoreceptor antagonist: alfuzosin
- -
- Antiarrhythmics: amiodarone, bepridil, dofetilide, flecainide, lidocaine (systemic), propafenone, quinidine
- -
- Antidepressant: trazodone
- -
- Anti-infectives: clarithromycin, erythromycin, halofantrine, pentamidine
- -
- Antimycobacterial Agents: rifampin
- -
- Antipsychotics: lurasidone, clozapine, haloperidol, pimozide, sertindole, ziprasidone, phenothiazines (e.g. chlorpromazine, mesoridazine, thioridazine).
- -
- Ergot Derivatives: dihydroergotamine, ergonovine, ergotamine, methylergonovine
- -
- HIV-1 Protease Inhibitor: atazanavir
- -
- HMG-CoA Reductase Inhibitors: lovastatin, simvastatin
- -
- Immunosuppressant: tacrolimus
- -
- Non-nucleoside reverse transcriptase inhibitor (NNRTI): rilpivirine (concomitant use and switching from rilpivirine to INVIRASE/ritonavir without a washout period of at least 2 weeks is contraindicated)
- -
- PDE5 Inhibitors: sildenafil (Revatio®)[for treatment of pulmonary arterial hypertension]
- -
- Sedative/Hypnotics: triazolam, and orally administered midazolam
- -
- Tyrosine kinase inhibitors: dasatinib, sunatinib
- -
- Other drugs that are CYP3A substrates: disopyramide, quinine
5 WARNINGS AND PRECAUTIONS
5.1 Importance of Co-administration with Ritonavir
INVIRASE must be used in combination with ritonavir. Refer to the ritonavir full prescribing information for additional precautionary measures.
INVIRASE is not recommended for use in combination with cobicistat. Dosing recommendations for this combination have not been established. Cobicistat is also not recommended in combination with regimens containing ritonavir due to similar effects of cobicistat and ritonavir on CYP3A. Refer to the cobicistat full prescribing information for additional precautionary measures.
5.2 Risk of Serious Adverse Reactions Due to Drug Interactions
Initiation of INVIRASE/ritonavir, a CYP3A inhibitor, in patients receiving medications metabolized by CYP3A or initiation of medications metabolized by CYP3A in patients already receiving INVIRASE/ritonavir, may increase plasma concentrations of medications metabolized by CYP3A. Initiation of medications that inhibit or induce CYP3A may increase or decrease concentrations of INVIRASE/ritonavir, respectively. These interactions may lead to:
- Clinically significant adverse reactions potentially leading to severe, life threatening, or fatal events from greater exposures of concomitant medications.
- Clinically significant adverse reactions from greater exposures of INVIRASE/ritonavir.
- Loss of therapeutic effect of INVIRASE/ritonavir and possible development of resistance.
See Table 2 for steps to prevent or manage these possible and known significant drug interactions, including dosing recommendations [see Drug Interactions (7)]. Consider the potential for drug interactions prior to and during INVIRASE/ritonavir therapy; review concomitant medications during INVIRASE/ritonavir therapy; and monitor for the adverse reactions associated with the concomitant medications [see Contraindications (4) and Drug Interactions (7)].
If a serious or severe toxicity occurs during treatment with INVIRASE/ritonavir, discontinue INVIRASE/ritonavir. For concomitantly used drugs including antiretroviral agents used in combination with INVIRASE/ritonavir, prescribers should refer to the complete product information for these drugs for dose adjustment recommendations and for information regarding drug-associated adverse reactions.
5.3 PR Interval Prolongation
INVIRASE/ritonavir prolongs the PR interval in a dose-dependent fashion. Cases of second or third degree atrioventricular block have been reported rarely. Patients with underlying structural heart disease, pre-existing conduction system abnormalities, cardiomyopathies and ischemic heart disease may be at increased risk for developing cardiac conduction abnormalities. ECG monitoring is recommended in these patients [see Warnings and Precautions (5.4)]. Discontinue INVIRASE/ritonavir if significant arrhythmias, QT or PR prolongation occur.
The impact on the PR interval of coadministration of INVIRASE/ritonavir with other drugs that prolong the PR interval (including calcium channel blockers, beta-adrenergic blockers, digoxin and atazanavir) has not been evaluated. As a result, coadministration of INVIRASE/ritonavir with these drugs should be undertaken with caution, particularly with those drugs metabolized by CYP3A, and clinical monitoring is recommended [see Clinical Pharmacology (12.2)].
For concomitantly used drugs, including antiretroviral agents used in combination with INVIRASE/ritonavir, physicians should refer to the complete product information for these drugs for dose adjustment recommendations and for information regarding drug-associated adverse reactions.
5.4 QT Interval Prolongation
INVIRASE/ritonavir causes dose-dependent QT prolongation. Torsade de pointes has been reported rarely post-marketing. Avoid INVIRASE/ritonavir in patients with long QT syndrome. ECG monitoring is recommended if therapy is initiated in patients with congestive heart failure, bradyarrhythmias, hepatic impairment and electrolyte abnormalities. Correct hypokalemia or hypomagnesemia prior to initiating INVIRASE/ritonavir and monitor these electrolytes periodically during therapy. Do not use in combination with drugs that both increase saquinavir plasma concentrations and prolong the QT interval (see Table 2) [see Clinical Pharmacology (12.2)]. For concomitantly used drugs, including antiretroviral agents used in combination with INVIRASE/ritonavir, refer to the complete product information for these drugs for dose adjustment recommendations and for information regarding drug-associated adverse reactions [see Contraindications (4) and Drug Interactions (7)]. Discontinue INVIRASE/ritonavir if significant arrhythmias, QT or PR prolongation occurs.
Patients initiating therapy with INVIRASE/ritonavir:
An ECG should be performed prior to initiation of treatment. Patients with a QT interval ≥ 450 msec should not initiate treatment with INVIRASE/ritonavir.
Treatment-naïve patients initiating treatment with INVIRASE/ritonavir should receive a reduced starting dose of INVIRASE 500 mg twice daily with ritonavir 100 mg twice daily for the first 7 days of treatment followed by INVIRASE/ritonavir 1000/100 mg twice daily due to potential for an increased risk of PR and QT interval prolongation with the standard 1000/100 mg twice daily dose [see Clinical Pharmacology (12.2)].
For patients with a baseline QT interval < 450 msec, an on-treatment ECG is recommended after approximately 10 days of therapy.
Discontinue INVIRASE/ritonavir in patients with a QT interval prolongation > 20 msec over pre-treatment.
Patients requiring treatment with medications with the potential to increase the QT interval and concomitant INVIRASE/ritonavir:
Such combinations should only be used where no alternative therapy is available, and the potential benefits outweigh the potential risks. An ECG should be performed prior to initiation of the concomitant therapy, and patients with a QT interval > 450 msec should not initiate the concomitant therapy. If baseline QT interval < 450 msec, an on-treatment ECG should be performed after 3–4 days of therapy. For patients demonstrating a subsequent increase in QT interval by > 20 msec after commencing concomitant therapy, the physician should use best clinical judgment to discontinue either INVIRASE/ritonavir or the concomitant therapy or both.
A cardiology consult is recommended if drug discontinuation or interruption is being considered on the basis of ECG assessment.
5.5 Diabetes Mellitus/Hyperglycemia
New onset of diabetes mellitus, exacerbation of preexisting diabetes mellitus and hyperglycemia have been reported during postmarketing surveillance in HIV-1-infected patients receiving protease-inhibitor therapy. Some patients required either initiation or dose adjustments of insulin or oral hypoglycemic agents for the treatment of these events. In some cases, diabetic ketoacidosis has occurred. In those patients who discontinued protease-inhibitor therapy, hyperglycemia persisted in some cases. Because these events have been reported voluntarily during clinical practice, estimates of frequency cannot be made and a causal relationship between protease-inhibitor therapy and these events has not been established.
5.6 Hepatotoxicity
In patients with underlying hepatitis B or C, cirrhosis, chronic alcoholism or other underlying liver abnormalities, there have been reports of worsening of the underlying liver disease and development of portal hypertension after starting INVIRASE/ritonavir. Jaundice and exacerbation of chronic liver disease with grade 4 elevated liver function tests were also observed. No dosage adjustment is necessary for patients with mild or moderate hepatic impairment based on limited data [see Clinical Pharmacology (12.3)]. INVIRASE/ritonavir is contraindicated in patients with severe hepatic impairment [see Contraindications (4)]. If a serious or severe toxicity occurs during treatment with INVIRASE/ritonavir, discontinue INVIRASE/ritonavir.
5.7 Hemophilia
There have been reports of spontaneous bleeding in patients with hemophilia A and B treated with protease inhibitors. In some patients, additional factor VIII was required. In the majority of reported cases, treatment with protease inhibitors was continued or restarted. A causal relationship between protease inhibitor therapy and these episodes has not been established.
5.8 Hyperlipidemia
Elevated cholesterol and/or triglyceride levels have been observed in some patients taking saquinavir in combination with ritonavir. Marked elevation in triglyceride levels is a risk factor for development of pancreatitis. Cholesterol and triglyceride levels should be monitored prior to initiating combination dosing regimen of INVIRASE/ritonavir, and at periodic intervals while on such therapy. In these patients, lipid disorders should be managed as clinically appropriate.
5.9 Lactose Intolerance
Each tablet contains lactose (monohydrate) 38.5 mg. INVIRASE is not recommended in patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption (autosomal recessive disorder).
5.10 Fat Redistribution
Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), facial wasting, peripheral wasting, breast enlargement, and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established.
5.11 Immune Reconstitution Syndrome
Immune reconstitution syndrome has been reported in patients treated with combination antiretroviral therapy, including INVIRASE/ritonavir. During the initial phase of combination antiretroviral treatment, patients whose immune system responds may develop an inflammatory response to indolent or residual opportunistic infections (such as Mycobacterium avium infection, cytomegalovirus, Pneumocystis jiroveci pneumonia [PCP], or tuberculosis), which may necessitate further evaluation and treatment.
Autoimmune disorders (such as Graves' disease, polymyositis, and Guillain-Barré syndrome) have also been reported to occur in the setting of immune reconstitution; however, the time to onset is more variable and can occur many months after initiation of treatment.
5.12 Resistance/Cross-resistance
Varying degrees of cross-resistance among HIV-1 protease inhibitors have been observed. Continued administration of INVIRASE/ritonavir therapy following loss of viral suppression may increase the likelihood of cross-resistance to other protease inhibitors [see Microbiology (12.4)].
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
- PR Interval Prolongation [see Warnings and Precautions (5.3)]
- QT Interval Prolongation [see Warnings and Precautions (5.4)]
6.1 Clinical Trial Experience in Adult Subjects
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The original INVIRASE safety database consisted of a total of 574 adult subjects who received 600 mg of saquinavir mesylate capsules (hard gel) alone or in combination with zidovudine (ZDV) or zalcitabine (ddC). Combination dosing with ritonavir is based on 352 HIV-1 infected subjects and 166 healthy subjects who received various combinations of either saquinavir mesylate capsules (hard gel or soft gel) with ritonavir.
The recommended dose of INVIRASE is 1,000 mg twice daily co-administered with ritonavir 100 mg twice daily. Table 1 lists Grade 2, 3 and 4 adverse events that occurred in ≥2% of subjects receiving saquinavir mesylate capsules (soft gel) with ritonavir (1000/100 mg bid).
| Adverse Events | Saquinavir Mesylate Capsules (soft gel) 1000 mg plus Ritonavir 100 mg bid (48 weeks) N=148 n (%=n/N) |
|---|---|
|
|
| Endocrine Disorders | |
| Diabetes mellitus/hyperglycemia | 4 (3) |
| Lipodystrophy | 8 (5) |
| Gastrointestinal Disorders | |
| Nausea | 16 (11) |
| Vomiting | 11 (7) |
| Diarrhea | 12 (8) |
| Abdominal Pain | 9 (6) |
| Constipation | 3 (2) |
| General Disorders and Administration Site Conditions | |
| Fatigue | 9 (6) |
| Fever | 5 (3) |
| Musculoskeletal Disorders | |
| Back Pain | 3 (2) |
| Respiratory Disorders | |
| Pneumonia | 8 (5) |
| Bronchitis | 4 (3) |
| Influenza | 4 (3) |
| Sinusitis | 4 (3) |
| Dermatological Disorders | |
| Rash | 5 (3) |
| Pruritus | 5 (3) |
| Dry lips/skin | 3 (2) |
| Eczema | 3 (2) |
Limited experience is available from three trials investigating the pharmacokinetics of the INVIRASE 500-mg film-coated tablet compared to the 200-mg saquinavir mesylate capsules (hard gel) in healthy volunteers (n=140). In two of these trials, saquinavir was combined with ritonavir; in the other trial, saquinavir was administered as single drug. The INVIRASE tablet and the saquinavir mesylate capsule (hard gel) were similarly tolerated. The most common adverse events were gastrointestinal disorders (nausea, vomiting, and diarrhea). Similar bioavailability was demonstrated and no clinically significant differences in saquinavir exposures were seen. Thus, similar safety profiles are expected between the two INVIRASE formulations.
A study investigating the drug-drug interaction of rifampin 600 mg/day daily and INVIRASE 1000 mg/ritonavir 100 mg twice daily enrolled 28 healthy volunteers. Eleven of 17 (65%) healthy volunteers exposed concomitantly to rifampin and INVIRASE/ritonavir developed severe hepatocellular toxicity which presented as increased hepatic transaminases. In some subjects, transaminases increased up to > 20-fold the upper limit of normal and were associated with gastrointestinal symptoms, including abdominal pain, gastritis, nausea, and vomiting. Following discontinuation of all three drugs, clinical symptoms abated and hepatic transaminases normalized [see Contraindications (4)].
Additional Adverse Reactions Reported During Clinical Trials with Saquinavir
Blood and lymphatic system disorders: anemia, hemolytic anemia, leukopenia, lymphadenopathy, neutropenia, pancytopenia, thrombocytopenia
Cardiac disorders: heart murmur, syncope
Ear and labyrinth disorders: tinnitus
Eye disorders: visual impairment
Gastrointestinal disorders: abdominal discomfort, ascites, dyspepsia, dysphagia, eructation, flatulence, gastritis, gastrointestinal hemorrhage, intestinal obstruction, mouth dry, mucosal ulceration, pancreatitis
General disorders and administration site conditions: anorexia, asthenia, chest pain, edema, lethargy, wasting syndrome, weight increased
Hepatobiliary disorders: chronic active hepatitis, hepatitis, hepatomegaly, hyperbilirubinemia, jaundice, portal hypertension
Immune system disorders: allergic reaction
Investigations: ALT increase, AST increase, blood creatine phosphokinase increased, increased alkaline phosphatase, GGT increase, raised amylase, raised LDH
Metabolism and nutrition disorders: increased or decreased appetite, dehydration, hypertriglyceridemia
Musculoskeletal and connective tissue disorders: arthralgia, muscle spasms, myalgia, polyarthritis
Neoplasms benign, malignant and unspecified (including cysts and polyps): acute myeloid leukemia, papillomatosis
Nervous system disorders: confusion, convulsions, coordination abnormal, dizziness, dysgeusia, headache, hypoesthesia, intracranial hemorrhage leading to death, loss of consciousness, paresthesia, peripheral neuropathy, somnolence, tremor
Psychiatric disorders: anxiety, depression, insomnia, libido disorder, psychotic disorder, sleep disorder, suicide attempt
Renal and urinary disorders: nephrolithiasis
Respiratory, thoracic and mediastinal disorders: cough, dyspnea
Skin and subcutaneous tissue disorders: acne, alopecia, dermatitis bullous, drug eruption, erythema, severe cutaneous reaction associated with increased liver function tests, Stevens-Johnson syndrome, sweating increased, urticaria
Vascular disorders: hypertension, hypotension, thrombophlebitis, peripheral vasoconstriction
6.2 Clinical Trial Experience in Pediatric Subjects
Limited safety data are available from two pediatric clinical trials of saquinavir mesylate capsules (hard gel) (approximately 50 mg per kg twice daily) used in combination with either low dose ritonavir or lopinavir/ritonavir. These trials enrolled pediatric subjects aged 4 months to 16 years old. In the HIVNAT 017 study (saquinavir mesylate capsules (hard gel) + lopinavir/ritonavir), adverse events were reported in 90% of the 50 subjects enrolled. The most commonly reported adverse events considered related to study treatment were diarrhea (18%) and vomiting (10%). In the NV20911 study (saquinavir mesylate capsules (hard gel) + ritonavir), 4 subjects (22% of 18 enrolled) experienced adverse events that were considered related to INVIRASE + ritonavir. These events (n) were vomiting (3), abdominal pain (1) and diarrhea (1). All reported adverse events were mild or moderate in intensity. The adverse reaction profile of INVIRASE in the pediatric trials is similar to that observed in adult trials.
6.3 Postmarketing Experience
Additional adverse events identified during postmarketing use are similar to those observed in clinical trials with INVIRASE, saquinavir mesylate capsules (hard gel and soft gel) alone or in combination with ritonavir. Because these events are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to INVIRASE exposure. In addition, torsade de pointes has been reported rarely [see Warnings and Precautions (5.4)].
7 DRUG INTERACTIONS
Drug interaction studies have been completed with INVIRASE and saquinavir mesylate capsules (hard gel and soft gel). Observations from drug interaction studies with saquinavir mesylate capsules (soft gel) may not be predictive for INVIRASE/ritonavir. Because ritonavir is coadministered with INVIRASE, prescribers should also refer to the prescribing information for ritonavir regarding drug interactions associated with this agent.
7.1 Potential for INVIRASE/Ritonavir to Affect Other Drugs
The combination INVIRASE/ritonavir is a potent inhibitor of CYP3A and may significantly increase the exposure of drugs primarily metabolized by CYP3A. Drugs that are contraindicated specifically due to the observed or expected magnitude of interaction and potential for serious or life-threatening adverse events are listed in Section 4 Contraindications [see Contraindications (4)]. Coadministration with other CYP3A substrates may require a dose adjustment or additional monitoring (see Table 2).
7.2 Potential for Other Drugs to Affect INVIRASE/Ritonavir
The metabolism of saquinavir is mediated primarily by CYP3A. Additionally, saquinavir is a substrate for P-glycoprotein (P-gp). Therefore, drugs that affect CYP3A and/or P-gp may modify the pharmacokinetics of saquinavir. Coadministration with drugs that are potent inducers of CYP3A (e.g., phenobarbital, phenytoin, carbamazepine) may result in decreased plasma concentrations of saquinavir and reduced therapeutic effect.
7.3 Established and Other Potentially Significant Drug Interactions
Based on the finding of dose-dependent prolongations of QT and PR intervals in healthy volunteers receiving INVIRASE/ritonavir, additive effects on QT and/or PR interval prolongation may occur with certain members of the following drug classes: antiarrhythmics class IA or class III, neuroleptics, antidepressants, PDE5 inhibitors (when used for pulmonary arterial hypertension), antimicrobials, antihistaminics and others. This effect might lead to an increased risk of ventricular arrhythmias, notably torsade de pointes. Therefore, concurrent administration of these agents with INVIRASE/ritonavir is contraindicated [see Contraindications (4)].
Table 2 provides examples of established or potentially clinically significant drug interactions. This table includes potentially significant interactions but is not all inclusive. Alteration in dose or avoidance of the combination may be recommended depending on the interaction.
| Concomitant Drug Class: Drug Name | Effect† on Concentration of Saquinavir or Concomitant Drug | Clinical Comment |
|---|---|---|
|
||
| HIV-1 Antiviral Agents | ||
| Non-nucleoside reverse transcriptase inhibitor:
Rilpivirine | ↑ Rilpivirine | Co-administration with INVIRASE/ritonavir and switching from rilpivirine to Invirase/ritonavir within 2 weeks is contraindicated due to the potential for life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Non-nucleoside reverse transcriptase inhibitor:
Delavirdine‡ | ↑ Saquinavir Effect on delavirdine is not well established | Appropriate doses of the combination with respect to safety and efficacy have not been established. Co-administration is not recommended. Liver function should be monitored frequently if this combination is prescribed. |
| Efavirenz§, nevirapine‡ | ↓ Saquinavir ↔ Efavirenz | Appropriate doses of the combination of efavirenz or nevirapine and INVIRASE/ritonavir with respect to safety and efficacy have not been established. Co-administration is not recommended. |
| HIV-1 protease inhibitor:
Atazanavir | ↑ Saquinavir ↑ Ritonavir ↑ Atazanavir | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| HIV-1 protease inhibitor:
Indinavir‡ | ↑ Saquinavir ↑ Indinavir | Appropriate doses of the combination of indinavir and INVIRASE/ritonavir with respect to safety and efficacy have not been established. Co-administration is not recommended. |
| Increased concentrations of indinavir may result in nephrolithiasis. For further details see complete prescribing information for indinavir. | ||
| Lopinavir/ritonavir§
(coformulated tablet) | ↔ Saquinavir ↔ Lopinavir ↓ Ritonavir | Evidence from several clinical trials indicates that saquinavir concentrations achieved with the saquinavir and lopinavir/ritonavir combination are similar to those achieved following INVIRASE/ritonavir 1000/100 mg. The recommended dose for this combination is INVIRASE 1000 mg plus lopinavir/ritonavir 400/100 mg bid. |
| Lopinavir/ritonavir in combination with INVIRASE should be used with caution. Additive effects on QT and/or PR interval prolongation may occur with INVIRASE [see Warnings and Precautions (5.3, 5.4)]. | ||
| Nelfinavir§ | ↑ Saquinavir | Combining saquinavir/ritonavir with nelfinavir is not recommended |
| Tipranavir/ritonavir§ | ↓ Saquinavir | Combining saquinavir with tipranavir/ritonavir is not recommended. |
| HIV-1 CCR5 antagonist:Maraviroc | ↑ Maraviroc | Maraviroc dose should be 150 mg twice daily when co-administered with INVIRASE/ritonavir. For further details see complete prescribing information for Selzentry® (maraviroc). |
| Other Agents | ||
| Alpha 1-adrenoreceptor antagonist: Alfuzosin | ↑ Alfuzosin | Co-administration is contraindicated with INVIRASE/ritonavir as potentially increased alfuzosin concentrations can result in hypotension, and potentially life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Antiarrhythmics:
Amiodarone, bepridil, dofetilide, flecainide, lidocaine (systemic), propafenone, quinidine | ↑ Amiodarone ↑ Bepridil ↑ Dofetilide ↑ Flecainide ↑ Lidocaine (systemic) ↑ Propafenone ↑ Quinidine | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Antiarrhythmics:
Ibutilide‡ Sotalol‡ | Effects on ibutilide, sotalol, and saquinavir concentrations are not well-established | Additive effects on QT and/or PR interval prolongation may occur with INVIRASE/ritonavir [see Contraindications (4) and Warnings and Precautions (5.3, 5.4)]. Co-administration of INVIRASE/ritonavir and ibutilide or sotalol is not recommended. |
| Anticoagulant: Warfarin‡ | ↑ Warfarin | Concentrations of warfarin may be affected. It is recommended that INR (international normalized ratio) be monitored. |
| Anticonvulsants:
Carbamazepine‡, phenobarbital‡, phenytoin‡ | ↓ Saquinavir Effect on carbamazepine, phenobarbital, and phenytoin is not well established | Saquinavir may be less effective due to decreased saquinavir plasma concentrations in patients taking these agents concomitantly. Co-administration is not recommended. |
| Antidepressant:
Trazodone | ↑ Trazodone | Co-administration is contraindicated with INVIRASE/ritonavir as increased trazodone concentrations can result in potentially life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Tricyclic antidepressants‡
Amitriptyline, clomipramine, imipramine, maprotiline | ↑ Tricyclics | Therapeutic concentration monitoring is recommended for tricyclic antidepressants when co-administered with INVIRASE/ritonavir. |
| Other antidepressants: Nefazodone‡ | ↑ Saquinavir | Use with caution due to possible cardiac arrhythmias. Clinical monitoring for saquinavir toxicity is recommended. |
| Antifungals: Ketoconazole§, | ↔ Saquinavir ↔ Ritonavir ↑ Ketoconazole | When INVIRASE/ritonavir and ketoconazole are co-administered, plasma concentrations of ketoconazole are increased (see Table 5). Hence, doses of ketoconazole or itraconazole > 200 mg/day are not recommended. |
| Itraconazole‡ | ↑ Itraconazole ↑ Saquinavir | Clinical monitoring for saquinavir toxicity is recommended. Use with caution due to possible cardiac arrhythmias. |
| Anti-gout: Colchicine | ↑ Colchicine | Treatment of gout flares-co-administration of colchicine in patients on INVIRASE/ritonavir:
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (half tablet) 1 hour later. Dose to be repeated no earlier than 3 days. Treatment of familial Mediterranean fever (FMF) co-administration of colchicine in patients on INVIRASE/ritonavir: Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day). Prophylaxis of gout flares-co-administration of colchicine in patients on INVIRASE/ritonavir: If the original colchicine regimen was 0.6 mg twice a day, the regimen should be adjusted to 0.3 mg once a day. If the original colchicine regimen was 0.6 mg once a day, the regimen should be adjusted to 0.3 mg once every other day. Patients with renal or hepatic impairment should not be given colchicine with INVIRASE/ritonavir. |
| Anti-infectives:
Clarithromycin, Erythromycin Halofantrine Pentamidine | ↑ Clarithromycin ↑ Erythromycin ↑ Halofantrine ↔ Pentamidine | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Anti-infectives:
Streptogramin antibiotics (quinupristin/dalfopristin‡) | Streptogramin antibiotics such as quinupristin/ dalfopristin inhibit CYP3A4; saquinavir concentrations may be increased | Monitoring for saquinavir toxicity is recommended. Use with caution due to possible cardiac arrhythmias. |
| Fusidic Acid | ↑ Saquinavir ↑ Fusidic Acid ↑ Ritonavir | Concomitant use of fusidic acid and INVIRASE/ritonavir is not recommended due to potential for increased mutual toxicities. The interaction between INVIRASE/ritonavir and fusidic acid has not been formally evaluated. Co-administration of fusidic acid and INVIRASE/ritonavir can cause increased plasma concentrations of fusidic acid, saquinavir and ritonavir. |
| Antimycobacterial: Rifabutin§ Dapsone‡ | ↔ Saquinavir ↑ Rifabutin ↔ Ritonavir ↑ Dapsone | No dose adjustment of INVIRASE/ritonavir (1000/100 mg bid) is required if INVIRASE/ritonavir is administered in combination with rifabutin. Dosage reduction of rifabutin by at least 75% of the usual dose of 300 mg/day is recommended (i.e., a maximum dose of 150 mg every other day or three times per week). Increased monitoring for adverse events including neutropenia and liver enzyme levels is warranted in patients receiving the combination. Consider monitoring rifabutin concentrations to ensure adequate exposure. Co-administration of saquinavir/ritonavir with drugs that are metabolized by CYP3A4 pathway may result in elevated plasma concentrations of these drugs. Co-administration with oral dapsone is not recommended. |
| Antimycobacterial:
Rifampin | ↑ Rifampin | Co-administration is contraindicated with INVIRASE/ritonavir as part of an ART regimen due to the risk of severe hepatocellular toxicity [see Contraindications (4)]. |
| Antipsychotic:
Quetiapine | ↑ Quetiapine | Initiation of INVIRASE with ritonavir in patients taking quetiapine:
Consider alternative antiretroviral therapy to avoid increases in quetiapine drug exposures. If co-administration is necessary, reduce the quetiapine dose to 1/6 of the current dose and monitor for quetiapine-associated adverse reactions. Refer to the quetiapine prescribing information for recommendations on adverse reaction monitoring. Initiation of quetiapine in patients taking INVIRASE with ritonavir: Refer to the quetiapine prescribing information for initial dosing and titration of quetiapine. |
| Antipsychotic:
Lurasidone | ↑ Lurasidone | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening reactions [see Contraindications (4)]. |
| Antipsychotics:
clozapine, haloperidol, pimozide, sertindole, ziprasidone, phenothiazines (e.g. chlorpromazine, mesoridazine, thioridazine). | ↑ Clozapine ↑ Haloperidol ↑ Pimozide ↑ Ziprasidone ↑ Chlorpromazine ↑ Mesoridazine ↑ Sertindole ↑ Thioridazine | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening reactions such as cardiac arrhythmias [see Contraindications (4)]. |
| Benzodiazepine: Triazolam, orally administered Midazolam | ↑ Midazolam ↑ Triazolam | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening reactions such as prolonged or increased sedation or respiratory depression [see Contraindications (4)]. |
| Benzodiazepines‡: Alprazolam, clorazepate, diazepam, flurazepam | ↑ Benzodiazepines | Clinical significance is unknown. Careful monitoring of patients for benzodiazepine effects is warranted; a decrease in benzodiazepine dose may be needed. |
| Intravenously administered Midazolam | ↑ Midazolam | If INVIRASE/ritonavir is co-administered with parenteral midazolam, close clinical monitoring for respiratory depression and/or prolonged sedation should be exercised and dosage adjustment should be considered. |
| Calcium channel blockers‡: Diltiazem, felodipine, nifedipine, nicardipine, nimodipine, verapamil, amlodipine, nisoldipine, isradipine | ↑ Calcium channel blockers | Close clinical monitoring of patients is recommended. |
| Systemic/Inhaled/Nasal/ Ophthalmic Corticosteroids: e.g. betamethasone, budesonide, ciclesonide, dexamethasone‡, fluticasone‡, methylprednisolone, mometasone, prednisone, triamcinolone | ↓ Saquinavir | Co-administration of INVIRASE/ritonavir with systemic dexamethasone or other systemic corticosteroids that induce CYP3A may result in loss of therapeutic effect and development of resistance to saquinavir. Consider alternative corticosteroids. |
| ↑Corticosteroids | Co-administration of INVIRASE/ritonavir with corticosteroids of which exposures are significantly increased by strong CYP3A inhibitors can increase the risk for Cushing's syndrome and adrenal suppression. Alternative corticosteroids including beclomethasone and prednisolone (for which PK and/or PD are less affected by strong CYP3A inhibitors relative to other steroids) should be considered, particularly for long term use. |
|
| Digitalis Glycosides: Digoxin§ | ↑ Digoxin Increases in serum digoxin concentration were greater in female subjects as compared to male subjects when digoxin was coadministered with INVIRASE/ritonavir. | Caution should be exercised when INVIRASE/ritonavir and digoxin are co-administered; serum digoxin concentrations should be monitored and the dose of digoxin may need to be reduced when co-administered with INVIRASE/ritonavir. |
| Endothelin receptor antagonists: Bosentan | ↑ Bosentan | Co-administration of bosentan in patients on INVIRASE/ritonavir:
In patients who have been receiving INVIRASE/ritonavir for at least 10 days, start bosentan at 62.5 mg once daily or every other day based upon individual tolerability. Co-administration of INVIRASE/ritonavir in patients on bosentan: Discontinue use of bosentan at least 36 hours prior to initiation of INVIRASE/ritonavir. After at least 10 days following the initiation of INVIRASE/ritonavir, resume bosentan at 62.5 mg once daily or every other day based upon individual tolerability. |
| Ergot derivatives:
Dihydroergotamine, ergonovine, ergotamine, methylergonovine | ↑ Dihydroergotamine, ↑ Ergonovine, ↑ Ergotamine, ↑ Methylergonovine | Co-administration is contraindicated in INVIRASE/ritonavir due to the potential for serious and life-threatening reactions such as ergot toxicity characterized by peripheral vasospasm and ischemia of the extremities and other tissues [see Contraindications (4)]. |
| Herbal Product:
St. John's wort‡ (hypericum perforatum) | ↓ Saquinavir | Herbal products containing St. John's wort should not be used concomitantly with INVIRASE/ritonavir because co-administration may lead to loss of virologic response and possible resistance to INVIRASE or to the class of protease inhibitors. |
| Garlic Capsules‡ | Co-administration of garlic capsules and saquinavir is not recommended due to the potential for garlic capsules to induce the metabolism of saquinavir which may result in sub-therapeutic saquinavir concentrations. | |
| HMG-CoA reductase inhibitors:
Lovastatin, Simvastatin | ↑ Lovastatin ↑ Simvastatin | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for myopathy including rhabdomyolysis [see Contraindications (4)]. |
| HMG-CoA reductase inhibitors‡:
Atorvastatin | ↑ Atorvastatin | Titrate atorvastatin dose carefully and use the lowest dose necessary; do not exceed atorvastatin 20 mg/day. Patients should be carefully monitored for signs and symptoms of myopathy (e.g., muscle weakness, muscle pain, rising creatine kinase). |
| Immunosuppressants:
Tacrolimus | ↑Tacrolimus | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Immunosuppressants: Cyclosporine‡, rapamycin‡ | ↑ Immunosuppressants | Therapeutic concentration monitoring is recommended for immunosuppressant agents when co-administered with INVIRASE/ritonavir. |
| Inhaled beta agonist:
Salmeterol | ↑ Salmeterol | Concurrent administration of salmeterol with INVIRASE/ritonavir is not recommended. The combination may result in increased risk of cardiovascular adverse events associated with salmeterol, including QT prolongation, palpitations and sinus tachycardia. |
| Narcotic analgesic:
Methadone§ | ↓ Methadone | Dosage of methadone may need to be increased when co-administered with INVIRASE/ritonavir. Use with caution. Additive effects on QT and/or PR interval prolongation may occur with INVIRASE/ritonavir [see Contraindications (4) and Warnings and Precautions (5.3, 5.4)]. |
| Oral contraceptives: Ethinyl estradiol‡ | ↓ Ethinyl estradiol | Alternative or additional contraceptive measures should be used when estrogen-based oral contraceptives and INVIRASE/ritonavir are co-administered. |
| PDE5 inhibitors (phosphodiesterase type 5 inhibitors):
Sildenafil§, vardenafil‡, tadalafil‡ | ↑ Sildenafil ↔ Saquinavir ↑ Vardenafil ↑ Tadalafil Only the combination of sildenafil with saquinavir mesylate capsules (soft gel) has been studied at doses used for treatment of erectile dysfunction. | May result in an increase in PDE5 inhibitor-associated adverse events, including hypotension, syncope, visual disturbances, and priapism. Use of PDE-5 inhibitors for pulmonary arterial hypertension (PAH):
Co-administration of Adcirca in patients on INVIRASE/ritonavir: In patients receiving INVIRASE/ritonavir for at least one week, start Adcirca at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability. Co-administration of INVIRASE/ritonavir in patients on Adcirca: Avoid use of Adcirca during the initiation of INVIRASE/ritonavir. Stop Adcirca at least 24 hours prior to starting INVIRASE/ritonavir. After at least one week following the initiation of INVIRASE/ritonavir, resume Adcirca at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability. Use of PDE5 inhibitors for erectile dysfunction: Use sildenafil with caution at reduced doses of 25 mg every 48 hours with increased monitoring of adverse events when administered concomitantly with INVIRASE/ritonavir. Use vardenafil with caution at reduced doses of no more than 2.5 mg every 72 hours with increased monitoring of adverse events when administered concomitantly with INVIRASE/ritonavir. Use tadalafil with caution at reduced doses of no more than 10 mg every 72 hours with increased monitoring of adverse events when administered concomitantly with INVIRASE/ritonavir. |
| Proton pump inhibitors: Omeprazole§ | ↑ Saquinavir | When INVIRASE/ritonavir is co-administered with omeprazole, saquinavir concentrations are increased significantly. If omeprazole or another proton pump inhibitor is taken concomitantly with INVIRASE/ritonavir, caution is advised and monitoring for potential saquinavir toxicities is recommended, particularly gastrointestinal symptoms, increased triglycerides, deep vein thrombosis, and QT prolongation. Use with caution due to possible cardiac arrhythmias. |
| Tyrosine kinase inhibitors:
Dasatinib Sunitinib | ↑ Dasatinib ↑ Sunitinib | Co-administration is contraindicated with INVIRASE/ritonavir due to potentially life-threatening cardiac arrhythmia [see Contraindications (4)] |
| Vasodilators (peripheral):
Intravenously administered Vincamine | ↑ Vincamine | Monitoring for vincamine toxicity is recommended. Use with caution due to potential cardiac arrhythmias. |
| Other drugs that are substrates of CYP3A:
Disopyramide Quinine | ↑ Disopyramide ↑ Quinine | Co-administration is contraindicated with INVIRASE/ritonavir due to the potential for serious and/or life-threatening cardiac arrhythmia [see Contraindications (4)]. |
| Other drugs that are substrates of CYP3A:
Fentanyl‡ Alfentanil‡ | ↑ Fentanyl ↑ Alfentanil | Co-administration with these drugs may accentuate the side effects reported with use of fentanyl or alfentanil including respiratory depression, apnea and bradycardia. |
7.4 Drugs without Clinically Significant Interactions with INVIRASE/Ritonavir
Based on drug interaction studies conducted with INVIRASE/ritonavir, no clinically significant effect was observed for saquinavir when coadministered with fosamprenavir. No clinically significant effect was observed for enfuvirtide when coadministered with INVIRASE/ritonavir.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in individuals exposed to antiretrovirals during pregnancy. Healthcare providers are encouraged to register patients by calling the Antiretroviral Pregnancy Registry (APR) at 1-800-258-4263.
Risk Summary
Prospective pregnancy data from the APR are not sufficient to adequately assess a drug-associated risk of birth defects or fetal outcomes. Limited number of reports on the use of saquinavir during pregnancy has been submitted to the APR and the number of exposures to saquinavir is insufficient to make a risk assessment compared to a reference population. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. The estimated background rate for major birth defects is 2.7% in the U.S. reference population of the Metropolitan Atlanta Congenital Defects Program (MACDP). The estimated rate of miscarriage is not reported in the APR. The estimated background rate of miscarriage in the U.S. general population is 15–20%.
In animal reproduction studies with saquinavir, no evidence of adverse developmental effects were observed at the highest achievable plasma exposures (AUC) in both rats and rabbits, resulting in exposures approximately 25% of those obtained in humans at the recommended human dose (RHD) combined with ritonavir. Saquinavir should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus (see Data).
Data
Human Data
Based on prospective reports to the APR following exposure to saquinavir-containing regimens, there were 7 birth defects reported in 183 first trimester exposures and 9 birth defects reported in 221 second and third trimester exposures. Insufficient numbers of pregnancies with exposure to saquinavir have been reported to the APR to calculate the prevalence (95% CI) or for a detailed assessment about the risk of saquinavir with regard to birth defects in this population. The background rate for major birth defects is 2.7% in a U.S. reference population of the MACDP. Prospective reports from the APR of overall major birth defects in pregnancies exposed to saquinavir are compared with the U.S. background major birth defect rate. Methodological limitations of the APR include the use of the MACDP as the external comparator group. Limitations of using an external comparator include differences in methodology and populations as well as confounding due to the underlying disease.
Animal Data
In animal reproduction studies, no evidence of harm to the fetus was detected when saquinavir was administered orally to pregnant rats and rabbits twice-daily during the period of organogenesis at dose levels up to 1200 (rats) or 1000 (rabbits) mg/kg/day. However, because of limited bioavailability of saquinavir in animals and/or dosing limitations, plasma exposures (AUC) in these species were only 29% (rat) and 21% (rabbits) of those obtained in humans at the RHD combined with ritonavir. In a pre- and postnatal development study, saquinavir was administered orally to pregnant rats (up to 1600 mg/kg/day) from gestation day 15 to post-partum day 20. No adverse effects were observed in the offspring exposed daily from before birth through lactation at maternal exposures (AUC) approximately 27% of those obtained in humans at the RHD combined with ritonavir.
8.2 Lactation
The Centers for Disease Control and Prevention recommends that HIV-infected mothers in the United States not breastfeed their infants to avoid risking postnatal transmission of HIV-1.
There are no data available regarding the presence of saquinavir in human milk, the effects on the breastfed infant, or the effects on milk production.
Because of the potential for (1) HIV-1 transmission (in HIV-negative infants), (2) developing viral resistance (in HIV-positive infants) and (3) adverse reactions in breastfed infants similar to those seen in adults, instruct mothers not to breastfeed if they are receiving INVIRASE.
8.4 Pediatric Use
The safety and activity of INVIRASE have been evaluated in 68 pediatric subjects 4 months to less than 16 years of age treated with saquinavir mesylate capsules (hard gel) combined with either ritonavir or with lopinavir/ritonavir in two clinical trials. Data from the NV20911 trial demonstrated that saquinavir mesylate capsules (hard gel) combined with low dose ritonavir provided plasma levels of saquinavir that were significantly higher than those historically observed in adults at the approved dose [see Clinical Pharmacology (12.3)]. The HIVNAT 017 trial provided long term 96-week activity and safety data; however, pharmacokinetic data from this study could not be validated.
HIVNAT 017 was an open-label, single-arm trial at two centers in Thailand that evaluated the use of saquinavir mesylate capsules (hard gel) (50 mg per kg twice daily given as 200-mg capsules) with lopinavir/ritonavir (230/57.5 mg/m2 twice daily) for 96 weeks. Fifty subjects 4 years to less than 16 years of age were enrolled. In this trial population, treatment resulted in HIV-1 RNA < 400 copies/mL at week 96 in 78% of subjects (HIV-1 RNA < 50 copies per mL at week 96 in 66%). Mean CD4 lymphocyte percentage increased from 8% at screening to 22% at week 96.
NV20911 was an open-label, multinational trial that evaluated the pharmacokinetics, safety, and activity of saquinavir mesylate capsules (hard gel) (50 mg per kg twice daily as 200-mg capsules, up to the adult dose of 1,000 mg twice daily) and ritonavir oral solution plus ≥ 2 background ARVs. Eighteen subjects 4 months to less than 6 years of age were enrolled. Treatment with INVIRASE/ritonavir resulted in HIV-1 RNA < 400 copies per mL at week 48 in 72% of subjects (HIV-1 RNA < 50 copies per mL at week 48 in 61%). The percentage of subjects with HIV-1 RNA < 50 copies per mL at week 48 was 61%. Mean CD4 lymphocyte percentage increased from 29% at screening to 34% at week 48.
Steady-state saquinavir exposures observed in pediatric trials were substantially higher than historical data in adults where dose- and exposure-dependent QTc and PR prolongation were observed [see Warnings and Precautions (5.3, 5.4), Clinical Pharmacology (12.2, 12.3)]. Although electrocardiogram abnormalities were not reported in these pediatric trials, the trials were small and not designed to evaluate QT or PR intervals. Modeling and simulation assessment of pharmacokinetic/pharmacodynamic relationships in pediatric subjects suggest that reducing the INVIRASE dose to minimize risk of QT prolongation is likely to reduce antiviral efficacy. In addition, no clinical efficacy data are available at INVIRASE doses less than 50 mg per kg in pediatric subjects. Therefore, pediatric dose recommendations that are both reliably effective and below thresholds of concern with respect to QT and PR prolongation could not be determined.
8.5 Geriatric Use
Clinical trials of INVIRASE did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. In general, dosing INVIRASE/ritonavir in elderly patients should be undertaken with caution keeping in mind the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
8.6 Impaired Renal Function
Renal clearance is a minor elimination pathway; the principal route of excretion for saquinavir is by hepatic metabolism. Therefore, no initial dose adjustment is necessary for patients with renal impairment. However, patients with severe renal impairment or end-stage renal disease (ESRD) have not been studied, and caution should be exercised when prescribing INVIRASE/ritonavir in this population.
8.7 Impaired Hepatic Function
No dosage adjustment is necessary for HIV-1-infected patients with mild or moderate hepatic impairment based on limited data. In patients with underlying hepatitis B or C, cirrhosis, chronic alcoholism and/or other underlying liver abnormalities, there have been reports of worsening liver disease [see Clinical Pharmacology (12.3)]. INVIRASE/ritonavir is contraindicated in patients with severe hepatic impairment [see Contraindications (4)].
10 OVERDOSAGE
There is limited experience of overdose with saquinavir.
No acute toxicities or sequelae were noted in one subject who ingested 8 grams of INVIRASE as a single dose. The subject was treated with induction of emesis within 2 to 4 hours after ingestion. A second subject ingested 2.4 grams of INVIRASE in combination with 600 mg of ritonavir and experienced pain in the throat that lasted for 6 hours and then resolved. In an exploratory Phase II study of oral dosing with INVIRASE at 7,200 mg per day (1,200 mg q4h), there were no serious toxicities reported through the first 25 weeks of treatment.
Treatment of overdose with saquinavir should consist of general supportive measures, including monitoring of vital signs and ECG and observations of the patient's clinical status. Since saquinavir is highly protein bound, dialysis is unlikely to be beneficial in significant removal of the active substance.
11 DESCRIPTION
INVIRASE brand of saquinavir mesylate is an inhibitor of the human immunodeficiency virus type 1 (HIV-1) protease.
The chemical name for saquinavir mesylate is N-tert-butyl-decahydro-2-[2(R)-hydroxy-4-phenyl-3(S)-[[N-(2-quinolylcarbonyl)-L-asparaginyl]amino]butyl]-(4aS,8aS)-isoquinoline-3(S)-carboxamide methanesulfonate with a molecular formula C38H50N6O5∙CH4O3S and a molecular weight of 766.96. The molecular weight of the free base is 670.86. Saquinavir mesylate has the following structural formula:
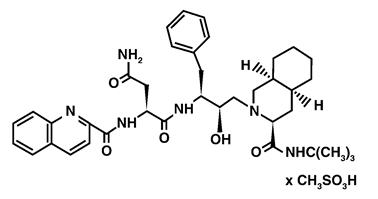
Saquinavir mesylate is a white to off-white, very fine powder with an aqueous solubility of 2.22 mg per mL at 25°C.
INVIRASE tablets are available as light orange to greyish- or brownish-orange, oval cylindrical, biconvex film-coated tablet for oral administration in 500-mg strength (as saquinavir free base). Each tablet also contains the inactive ingredients lactose, microcrystalline cellulose, povidone K30, croscarmellose sodium, and magnesium stearate. Each film coat contains hypromellose, titanium dioxide, talc, iron oxide yellow, iron oxide red, and triacetin.
12 CLINICAL PHARMACOLOGY
12.2 Pharmacodynamics
QTcS interval was evaluated in a randomized, placebo and active (moxifloxacin 400 mg once daily) controlled crossover study in 59 healthy adults, with ECG measurements on Day 3. The maximum mean (95% upper confidence bound) differences in QTcS interval from placebo after baseline-correction were 18.9 (22.0) and 30.2 (33.4) ms for 1000/100 mg twice daily and supratherapeutic 1500/100 mg twice daily of INVIRASE/ritonavir, respectively. There is a delayed effect between QTc interval change and drug concentrations, with the maximum placebo-adjusted baseline-corrected QTcS observed at about 12-20 hours post-dose. INVIRASE/ritonavir 1500/100 mg twice daily resulted in a Day 3 mean Cmax of INVIRASE approximately 40% higher than the mean Cmax observed on Day 3 with the approved therapeutic dose in healthy volunteers (within the same study). QTcS in this study was QT/RR0.319 for males and QT/RR0.337 for females, which are similar to Fridericia's correction (QTcF=QT/RR0.3333).
PR and QRS interval prolongations were also noted in subjects receiving INVIRASE/ritonavir in the same study on Day 3. The maximum mean (95% upper confidence bound) difference from placebo in the PR interval after baseline-correction were 28.6 (31.6) and 38.4 (41.4) ms for 1000/100 mg twice daily and supratherapeutic 1500/100 mg twice daily saquinavir/ritonavir respectively. The maximum mean (95% upper confidence bound) difference from placebo in QRS interval after baseline correction were 2.9 (3.9) and 4.4 (5.3) ms for 1000/100 mg twice daily and supratherapeutic 1500/100 mg twice daily INVIRASE/ritonavir respectively. In this study using healthy subjects, PR interval prolongation of > 200 ms was also observed in 40% and 47% of subjects receiving INVIRASE/ritonavir 1000/100 mg bid and 1500/100 mg bid, respectively, on Day 3. Three (3%) subjects in the active control moxifloxacin arm and 5% in the placebo arm experienced PR prolongation of > 200 ms.
The effect of treatment initiation with a dosing regimen of INVIRASE/ritonavir 500/100 mg twice daily in combination with two nucleoside reverse transcriptase inhibitors (NRTIs) for the first 7 days of treatment followed by INVIRASE/ritonavir 1000/100 mg twice daily in combination with two NRTIs in the subsequent 7 days on QTc interval, PK, and viral load was evaluated in an open-label 2-week observational study in 23 HIV-1 infected, treatment-naive patients. ECG and PK measurements were collected on Days 3, 4, 7, 10, and 14 of treatment. Two of 21 (9%) patients across all study days had maximum QTcF change from dense predose baseline ≥ 30 msec following administration of the modified INVIRASE/ritonavir regimen and the maximum mean change from dense predose baseline in the QTcF was < 10 msec across all study days. The proportion of patients with a reported PR interval prolongation > 200 msec in this study ranged from 3/22 (14%) (Day 3) to 8/21 (38%) (Day14). These results suggest that the risk of QTc interval prolongation is reduced with the modified INVIRASE/ritonavir dosing regimen, based on a cross-study comparison to the moxifloxacin-controlled QTc study described above.
12.3 Pharmacokinetics
The pharmacokinetics of INVIRASE/ritonavir 1000/100 mg twice daily have been evaluated in HIV-1-infected subjects and healthy subjects. Steady-state saquinavir AUC, Cmax, and Cmin in healthy subjects are approximately 50% higher than observed in HIV-1-infected subjects.
Adults
Absorption and Bioavailability in Adults
Similar bioavailability was demonstrated when 1,000 mg of INVIRASE tablets or 1,000 mg of saquinavir mesylate capsules (hard gel) was administered with low-dose ritonavir (100 mg) under fed conditions. The ratio of mean exposures (90% confidence intervals) of tablets vs capsules was 1.10 (1.04-1.16) for AUC0-∞ and 1.19 (1.14-1.25) for Cmax.
Absolute bioavailability of saquinavir administered as saquinavir mesylate capsules (hard gel) averaged 4% (CV 73%, range: 1% to 9%) in 8 healthy volunteers who received a single 600 mg dose (3 × 200-mg) of saquinavir mesylate following a high-fat breakfast (48 g protein, 60 g carbohydrate, 57 g fat; 1006 kcal). The low bioavailability is thought to be due to a combination of incomplete absorption and extensive first-pass metabolism.
INVIRASE/ritonavir at a dose of 1000/100 mg twice daily provides saquinavir systemic exposures over a 24-hour period that are similar to those achieved with saquinavir soft gel capsules with ritonavir 1000/100 mg twice daily and greater than that achieved with saquinavir soft gel capsules 1200 mg three times daily (see Table 3).
| Dosing Regimen | N | AUCτ
(ng∙h/mL) | AUC24h
(ng∙h/mL) | Cmin
(ng/mL) |
|---|---|---|---|---|
| τ is the dosing interval (i.e., 8h if three times daily and 12h if twice daily) | ||||
| Saquinavir mesylate capsules (hard gel) 600 mg tid (arithmetic mean, %CV) | 10 | 866 (62) | 2598 | 79 |
| Saquinavir mesylate capsules (soft gel) 1,200 mg tid (arithmetic mean) | 31 | 7249 | 21747 | 216 |
| Saquinavir mesylate capsules (hard gel) 1000 mg bid + ritonavir 100 mg bid (geometric mean and 95% CI) | 24 | 14607 (10218-20882) | 29214 | 371 (245-561) |
| Saquinavir mesylate capsules (soft gel) 1000 mg bid + ritonavir 100 mg bid (geometric mean and 95% CI) | 24 | 19085 (13943-26124) | 38170 | 433 (301-622) |
In treatment-naïve HIV-1 infected patients initiating INVIRASE/ritonavir treatment with a modified INVIRASE/ritonavir dosing regimen of INVIRASE 500 mg twice daily with ritonavir 100 mg twice daily for the first 7 days of treatment followed by an increase in the INVIRASE dose to 1000 mg twice daily with ritonavir 100 mg twice daily for an additional 7 days, saquinavir systemic exposures on Day 3 were approximately 70% lower compared to INVIRASE/ritonavir 1000/100 mg twice daily regimen on Day 3 in healthy volunteers. Saquinavir systemic exposures across study days generally approached or exceeded the range of historical steady-state values with the standard INVIRASE/ritonavir 1000 mg/100 mg twice daily dosing regimen (see Table 3 and Table 4).
| Parameter | Day 3 500/100 mg (n=22) | Day 7 500/100 mg (n=21) | Day 14 1000/100 mg (n=21) | TQT Study Day 3* (1000/100 mg) (n=57) |
|---|---|---|---|---|
|
||||
| AUCτ (ng*hr/ml) | 27100 (35.7) | 12600 (54.5) | 31100 (49.6) | 94800 (32.2) |
| Cmax (ng/ml) | 4030 (29.1) | 1960 (53.3) | 4860 (46.8) | 11200 (29.2) |
| C12 (ng/ml) | 899 (64.9) | 416 (98.5) | 1120 (80.9) | - |
Food Effect
The mean 24-hour AUC after a single 600 mg oral dose (6 × 100 mg) in healthy volunteers (n=6) was increased from 24 ng∙h/mL (CV 33%), under fasting conditions, to 161 ng∙h/mL (CV 35%) when INVIRASE was given following a high-fat breakfast (48 g protein, 60 g carbohydrate, 57 g fat; 1006 kcal). Saquinavir 24-hour AUC and Cmax (n=6) following the administration of a higher calorie meal (943 kcal, 54 g fat) were on average 2 times higher than after a lower calorie, lower fat meal (355 kcal, 8 g fat). The effect of food has been shown to persist for up to 2 hours.
INVIRASE/ritonavir should be taken within 2 hours after a meal.
Distribution
The mean steady-state volume of distribution following intravenous administration of a 12-mg dose of saquinavir (n=8) was 700 L (CV 39%), suggesting saquinavir partitions into tissues. Saquinavir was approximately 98% bound to plasma proteins over a concentration range of 15 to 700 ng/mL. In two subjects receiving saquinavir mesylate 600 mg three times daily, cerebrospinal fluid concentrations were negligible when compared to concentrations from matching plasma samples.
Metabolism and Elimination
In vitro studies using human liver microsomes have shown that the metabolism of saquinavir is cytochrome P450 mediated with the specific isoenzyme, CYP3A4, responsible for more than 90% of the hepatic metabolism. Based on in vitro studies, saquinavir is rapidly metabolized to a range of mono- and di-hydroxylated inactive compounds. In a mass balance study using 600 mg 14C saquinavir mesylate (n=8), 88% and 1% of the orally administered radioactivity was recovered in feces and urine, respectively, within 5 days of dosing. In an additional 4 subjects administered 10.5 mg 14C-saquinavir intravenously, 81% and 3% of the intravenously administered radioactivity was recovered in feces and urine, respectively, within 5 days of dosing. In mass balance studies, 13% of circulating radioactivity in plasma was attributed to unchanged drug after oral administration and the remainder attributed to saquinavir metabolites. Following intravenous administration, 66% of circulating radioactivity was attributed to unchanged drug and the remainder attributed to saquinavir metabolites, suggesting that saquinavir undergoes extensive first-pass metabolism.
Systemic clearance of saquinavir was rapid, 1.14 L/h/kg (CV 12%) after intravenous doses of 6, 36, and 72 mg. The mean residence time of saquinavir was 7 hours (n=8).
Special Populations
Renal Impairment
Saquinavir pharmacokinetics in patients with renal impairment has not been investigated. Only 1% of saquinavir is excreted in the urine, so the impact of renal impairment on saquinavir elimination would likely be minimal. However, subjects with severe renal impairment or end-stage renal disease (ESRD) have not been studied, and concentrations of saquinavir may be elevated in these populations.
Hepatic Impairment
The effect of hepatic impairment on the steady state pharmacokinetics of INVIRASE/ritonavir (1000/100 mg bid for 14 days) was investigated in 7 HIV-1-infected subjects with moderate liver impairment (6 with Child-Pugh score of 7 and 1 with Child-Pugh score of 9). The study included a control group consisting of 7 HIV-1-infected subjects with normal hepatic function matched with hepatically impaired subjects for age, gender, weight and tobacco use. The mean (% coefficient of variation in parentheses) values for INVIRASE AUC0-12 and Cmax were 24.3 (102%) µg∙hr/mL and 3.6 (83%) µg/mL, respectively, for HIV-1-infected subjects with moderate hepatic impairment. The corresponding values in the control group were 28.5 (71%) µg∙hr/mL and 4.3 (68%) µg/mL. The geometric mean ratio (ratio of pharmacokinetic parameters in hepatically impaired subjects to subjects with normal liver function) (90% confidence interval) was 0.7 (0.3 to 1.6) for both AUC0-12 and Cmax, which suggests approximately 30% reduction in saquinavir exposure in subjects with moderate hepatic impairment. No dose adjustment is warranted for INVIRASE/ritonavir in HIV-1-infected patients with mild or moderate hepatic impairment [see Warnings and Precautions (5.6)].
Gender, Race, and Age
A gender difference was observed, with females showing higher saquinavir exposure than males (mean AUC 56% higher, mean Cmax 26% higher), in the relative bioavailability study comparing 1,000 mg of INVIRASE tablets to 1,000 mg of saquinavir mesylate capsules (hard gel) in combination with ritonavir. There was no evidence that age and body weight explained the gender difference in this study. A clinically significant difference in safety and efficacy between men and women has not been reported with the approved dosage regimen (saquinavir 1,000 mg/ritonavir 100 mg twice daily).
The effect of race on the pharmacokinetics of saquinavir has not been investigated.
The pharmacokinetics of saquinavir have not been evaluated in the elderly.
Pediatric Subjects
Steady-state pharmacokinetic information is available from HIV-1 infected pediatric subjects from study NV20911. In this study, five subjects less than 2 years of age and 13 subjects between 2 and less than 6 years of age received 50 mg per kg saquinavir twice daily (not to exceed 1000 mg twice daily) combined with ritonavir at 3 mg/kg for subjects with body weight ranging from 5 to <15 kg or 2.5 mg per kg for subjects with body weight ranging from 15 to 40 kg (not to exceed 100 mg twice daily). For subjects unable to swallow the saquinavir mesylate capsules (hard gel), the contents of saquinavir mesylate capsules (hard gel) were mixed with sugar syrup, or sorbitol syrup (for subjects with Type I diabetes or glucose intolerance), jam, or baby formula. The mean steady state saquinavir PK parameters for pediatric subjects 2 to less than 6 years of age were: AUC0-12h 37269 ± 18232 ng∙h/mL; Ctrough 1811± 998 ng/mL; Cmax 5464± 2782 ng/mL, and day 3 exposures may be within the range of exposure associated with QT and PR prolongation [see Clinical Pharmacology (12.2)]. The subject number was too low and the pharmacokinetic data too variable in subjects less than 2 years to establish an appropriate dosing recommendation for this age group. Pharmacokinetic data for subjects ages 6 to 16 years were not available for comparisons with observations from NV20911, as the data from HIVNAT 017 could not be validated [see Use in Specific Populations (8.4)].
Drug Interactions
Table 5 summarizes the effect of saquinavir mesylate capsules (soft gel) and INVIRASE with and without ritonavir on the geometric mean AUC and Cmax of coadministered drugs. Table 6 summarizes the effect of coadministered drugs on the geometric mean AUC and Cmax of saquinavir.
| Coadministered Drug | Saquinavir Mesylate Capsules (soft gel) with and without Ritonavir | N | % Change for Coadministered Drug | |
|---|---|---|---|---|
| Dosage | AUC (95% CI) | Cmax (95% CI) | ||
| ↑ Denotes an average increase in exposure by the percentage indicated. | ||||
| ↓ Denotes an average decrease in exposure by the percentage indicated. | ||||
| ↔ Denotes no statistically significant change in exposure was observed. | ||||
| V Healthy Volunteers | ||||
| M Methadone-dependent, HIV negative subjects. None of the 12 subjects experienced withdrawal symptoms. | ||||
| NA Not Available | ||||
| Clarithromycin 500 mg bid × 7 days Clarithromycin 14-OH clarithromycin metabolite | 1200 mg tid × 7 days | 12V | ↑45% (17-81%) ↓24% (5-40%) | ↑39% (10-76%) ↓34% (14-50%) |
| Sildenafil 100-mg single dose | 1200 mg tid × 8 days | 27V | ↑210% (150-300%) | ↑140% (80-230%) |
| Efavirenz 600 mg qd | 1200 mg tid | 13V | ↓12% | ↓13% |
| INVIRASE/ritonavir Dosage | ||||
| Digoxin 0.5 mg single dose | 1000/100 mg bid × 16 days | 16V | ↑49% (32-69%)* | ↑27% (5-54%)* |
| R-Methadone 60-120 mg qd | 1000/100 mg bid × 14 days | 12M | ↓19% (9-29%)* | NA |
| Ketoconazole 200 mg/day | 1000/100 mg bid | 12V | ↑168% (146-193%)* | ↑45% (32-59%)* |
| Midazolam 7.5 mg oral single dose | 1000/100 mg bid | 16V | ↑1144% (975-1339%)* | ↑327% (264-402%)* |
| Rifabutin 150 mg q4d | 1000/100 mg bid | 11V | ↑60%†‡
(43-79%)* ↔§ (-10 to 13%)* | ↑111%†‡
(75-153%)* ↑68%§ (38-105%)* |
| ↑ Denotes an average increase in exposure by the percentage indicated. | ||||
| ↓ Denotes an average decrease in exposure by the percentage indicated. | ||||
| ↔ Mean change <10% | ||||
| S Subjects | ||||
| V Healthy Volunteers | ||||
| Coadministered Drug | Saquinavir Mesylate Capsules (soft gel) with and without ritonavir | N | % Change for Saquinavir | |
| Dosage | AUC (95% CI) | Cmax (95% CI) | ||
| Clarithromycin 500 mg bid × 7 days | 1200 mg tid × 7 days | 12V | ↑177% (108-269%) | ↑187% (105-300%) |
| Efavirenz 600 mg qd | 1200 mg tid | 13V | ↓62% | ↓50% |
| Indinavir 800 mg q8h × 2 days | 1200 mg single dose | 6V | ↑364% (190-644%) | ↑299% (138-568%) |
| Ritonavir 400 mg bid × 14 days | 400 mg bid × 14 days* | 8V | ↑121% (7-359%) | ↑64%† |
| Lopinavir/ritonavir Evidence from several clinical trials indicates that saquinavir concentrations achieved with saquinavir 1000 mg + lopinavir/ritonavir 400/100 mg BID are similar to those achieved following saquinavir/ritonavir 1000/100 mg BID. |
||||
| Coadministered Drug | Saquinavir Mesylate Capsules (hard gel) or INVIRASE with and without ritonavir | N | % Change for Saquinavir | |
| Dosage | AUC (95% CI) | Cmax (95% CI) | ||
| Atazanavir 300 mg qd | 1600/100 mg qd | 18S | ↑60% (16-122%) | ↑42% (10-84%) |
| Ritonavir 100 mg bid | 1000 mg bid‡ | 24S | ↑1124% | ↑1325% |
| Tenofovir 300 mg qd | 1000 mg bid/100 mg bid | 18S | ↔ | ↔ |
| Tipranavir 500 mg + ritonavir 200 mg bid | 600 mg bid/100 mg bid | 20S | ↓76% (68-81%)§ | ↓70% (60-77%)§ |
| Omeprazole 40 mg qd × 5 days | 1000/100 mg bid × 15 days | 19V | ↑82% (37-234%)§ | ↑ 75% (31-234%)§ |
| Ketoconazole 200 mg/day | 1000 mg bid/100 mg bid | 20V | ↔§ | ↔ |
| Rifabutin 150 mg q3d | 1000 mg bid/100 mg bid | 19V | ↓13% (-31% to 9%)§ | ↓15% (-32% to 7%)§ |
The HIV-1 antiviral drugs didanosine, tenofovir, and zidovudine are not predicted to have any clinically significant effect on the pharmacokinetics of saquinavir with and without ritonavir. No clinically significant effect on the pharmacokinetic parameters of enfuvirtide was observed with coadministration of INVIRASE/ritonavir. No clinically significant effect on the pharmacokinetic parameters of saquinavir was observed with coadministration of fosamprenavir.
12.4 Microbiology
Mechanism of Action
Saquinavir is an inhibitor of HIV-1 protease. HIV-1 protease is an enzyme required for the proteolytic cleavage of viral polyprotein precursors into individual functional proteins found in HIV-1 particles. Saquinavir is a peptide-like substrate analogue that binds to the protease active site and inhibits the activity of the enzyme. Saquinavir inhibition prevents cleavage of the viral polyproteins resulting in the formation of immature noninfectious viral particles.
Antiviral Activity
The antiviral activity of saquinavir was assessed in lymphoblastoid and monocytic cell lines and in peripheral blood lymphocytes in cell culture. Saquinavir inhibited HIV-1 activity in both acutely and chronically infected cells. EC50 and EC90 values (50% and 90% inhibitory concentrations) ranged from 1 to 30 nM and 5 to 80 nM, respectively. In the presence of 40% human serum, the mean EC50 value of saquinavir against laboratory strain HIV-1 RF in MT4 cells was 37.7± 5 nM representing a 4-fold increase in the EC50 value. Saquinavir displayed antiviral activity in cell culture against HIV-1 clades A–H (EC50 values ranged from 0.9 to 2.5 nM). In cell culture, saquinavir was not antagonistic in combination with the protease inhibitors amprenavir, atazanavir and lopinavir, the non-nucleoside reverse transcriptase inhibitor nevirapine, and the nucleoside analog reverse transcriptase inhibitors didanosine, lamivudine, stavudine and zidovudine. The EC50 and EC90 values of saquinavir against HIV-2 isolates in cell culture ranged from 0.25 nM to 14.6 nM and 4.65 nM to 28.6 nM, respectively.
Resistance
HIV-1 isolates with reduced susceptibility to saquinavir have been selected during passage in cell culture. Genotypic analyses of these isolates showed several amino acid substitutions in the HIV-1 protease. Only the G48V and L90M substitutions were associated with reduced susceptibility to saquinavir and conferred an increase in the EC50 value of 8- and 3-fold, respectively.
HIV-1 isolates with reduced susceptibility (≥ 4-fold increase in the EC50 value) to saquinavir emerged in some subjects treated with INVIRASE. Genotypic analysis of these isolates identified resistance conferring primary amino acid substitutions in the protease G48V and L90M, and secondary substitutions L10I/R/V, I54V/L, A71V/T, G73S, V77I, V82A and I84V that contributed additional resistance to saquinavir. Forty-one isolates from 37 subjects failing therapy with INVIRASE had a median decrease in susceptibility to saquinavir of 4.3-fold.
The degree of reduction in cell culture susceptibility to saquinavir of clinical isolates bearing substitutions G48V and L90M depends on the number of secondary substitutions present. In general, higher levels of resistance are associated with greater number of substitutions only in association with either or both of the primary substitutions G48V and L90M. No data are currently available to address the development of resistance in patients receiving saquinavir/ritonavir.
Cross-resistance
Among protease inhibitors, variable cross-resistance has been observed. In one clinical study, 22 HIV-1 isolates with reduced susceptibility (> 4-fold increase in the EC50 value) to saquinavir following therapy with INVIRASE were evaluated for cross-resistance to amprenavir, indinavir, nelfinavir and ritonavir. Six of the 22 isolates (27%) remained susceptible to all 4 protease inhibitors, 12 of the 22 isolates (55%) retained susceptibility to at least one of the protease inhibitors and 4 out of the 22 isolates (18%) displayed broad cross-resistance to all protease inhibitors. Sixteen (73%) and 11 (50%) of the 22 isolates remained susceptible (< 4-fold) to amprenavir and indinavir, respectively. Four of 16 (25%) and nine of 21 (43%) with available data remained susceptible to nelfinavir and ritonavir, respectively.
After treatment failure with amprenavir, cross-resistance to saquinavir was evaluated. HIV-1 isolates from 22/22 subjects failing treatment with amprenavir and containing one or more substitutions M46L/I, I50V, I54L, V32I, I47V, and I84V were susceptible to saquinavir.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies found no indication of carcinogenic activity in rats and mice administered saquinavir for approximately 2 years. Because of limited bioavailability of saquinavir in animals, the plasma exposures (AUC values) in the respective species were approximately 29% (using rat) and 65% (using mouse) of those obtained in humans at the recommended clinical dose combined with ritonavir.
Mutagenesis
Mutagenicity and genotoxicity studies, with and without metabolic activation where appropriate, have shown that saquinavir has no mutagenic activity in vitro in either bacterial (Ames test) or mammalian cells (Chinese hamster lung V79/HPRT test). Saquinavir does not induce chromosomal damage in vivo in the mouse micronucleus assay or in vitro in human peripheral blood lymphocytes, and does not induce primary DNA damage in vitro in the unscheduled DNA synthesis test.
Impairment of Fertility
No adverse effects were reported in fertility and reproductive performance study conducted in rats. Because of limited bioavailability of saquinavir in animals, the maximal plasma exposures achieved in rats were approximately 26% of those obtained in humans at the recommended clinical dose combined with ritonavir.
14 CLINICAL STUDIES
14.1 Description of Clinical Studies in Adults
In a randomized, double-blind clinical study NV14256 in zidovudine-experienced, HIV-1-infected adult subjects, saquinavir mesylate capsules (hard gel) in combination with zalcitabine1 was shown to be superior to monotherapy with either saquinavir mesylate capsules (hard gel) or zalcitabine in decreasing the cumulative incidence of clinical disease progression to AIDS-defining events or death. In another randomized study ACTG229/NV14255, subjects with advanced HIV-1 infection with history of prolonged zidovudine treatment were administered saquinavir mesylate capsules (hard gel) 600 mg (three times daily) + zidovudine + zalcitabine. Subjects receiving this regimen experienced greater increases in CD4+ cell counts as compared to those who received saquinavir mesylate capsules (hard gel) + zidovudine or zalcitabine + zidovudine. It should be noted the HIV treatment regimens that were used in these clinical trials are no longer considered standard of care.
In the MaxCmin1 trial, saquinavir gel capsule 1,000 mg twice daily coadministered with ritonavir 100 mg twice daily was evaluated in a heterogeneous population of 148 HIV-1-infected subjects. A total of 42 subjects enrolled were treatment naïve, and 106 subjects were treatment experienced (of which 52 subjects had HIV-1 RNA < 400 copies/mL at baseline). Results showed that 91/148 (61%) subjects achieved and/or sustained an HIV-1 RNA < 400 copies per mL at the completion of 48 weeks of treatment.
- 1
- No longer available in the US.
16 HOW SUPPLIED/STORAGE AND HANDLING
INVIRASE 500-mg film-coated tablets are light orange to greyish or brownish orange, oval cylindrical, biconvex tablets with ROCHE and SQV 500 imprinted on the tablet face—bottles of 120 (NDC 0004-0244-51). INVIRASE tablets should be stored at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature] in tightly closed bottles.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Important Dosing Instructions
Advise patients that INVIRASE must be used in combination with ritonavir, which significantly inhibits saquinavir's metabolism to provide increased plasma saquinavir levels.
Advise patients that INVIRASE administered with ritonavir should be taken within 2 hours after a meal [see Clinical Pharmacology (12.3)]. When INVIRASE/ritonavir is taken without food, concentrations of saquinavir in the blood are substantially reduced and may result in no antiviral activity. Advise patients of the importance of taking their medication every day, as prescribed, to achieve maximum benefit. Patients should not alter the dose or discontinue therapy without consulting their physician. If a dose is missed, patients should take the next dose as soon as possible; however, the patient should not double the next dose.
Risk of Serious Adverse Reactions Drug Interactions
INVIRASE/ritonavir may interact with many drugs; therefore, advise patients to report the use of any other prescription, nonprescription medication, or herbal products, particularly St. John's wort [see Contraindications (4), Warnings and Precautions (5.2), and Drug Interactions (7)].
PR and QT Interval Prolongation
Inform patients that INVIRASE/ritonavir may produce changes in the electrocardiogram (PR interval or QT interval prolongation). Advise patients to consult their health care provider if they are experiencing symptoms such as dizziness, lightheadedness, or palpitations [see Warnings and Precautions (5.3, 5.4)].
Diabetes Mellitus/Hyperglycemia
Inform patients that new onset of diabetes or exacerbation of pre-existing diabetes mellitus, and hyperglycemia have been reported during INVIRASE/ritonavir use. Advise patients to notify their healthcare provider if they develop signs and symptoms of diabetes [see Warnings and Precautions (5.5)].
Hepatotoxicity
Inform patients with underlying liver abnormalities that there have been reports of worsening liver disease and development of portal hypertension with INVIRASE/ritonavir. Advise patients about the signs and symptoms of liver problems [see Warnings and Precautions (5.6)]
Hyperlipidemia
Advise patients that treatment with INVIRASE/ritonavir can result in substantial increases in total cholesterol and triglycerides [see Warnings and Precautions (5.8)]
Fat Redistribution
Inform patients that redistribution or accumulation of body fat may occur in patients receiving antiretroviral therapy, including INVIRASE/ritonavir, and that the cause and long-term health effects of these conditions are not known at this time [see Warnings and Precautions (5.10)].
Immune Reconstitution Syndrome
Advise patients to inform their healthcare provider immediately of any symptoms of infection, as in some patients with advanced HIV infection (AIDS), signs and symptoms of inflammation from previous infections may occur soon after anti-HIV treatment is started [see Warnings and Precautions (5.11)].
Pregnancy Exposure Registry
Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to antiretrovirals during pregnancy [see Use in Specific Populations (8.1)].
Lactation
Instruct mothers with HIV-1 infection not to breastfeed because HIV-1 can be passed to the baby in breast milk [see Use in Specific Populations (8.2)].
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: September 2020 | ||
| Medication Guide | |||
| INVIRASE® (in-ver-ase) (saquinavir mesylate) Tablets |
|||
| Important: Ask your healthcare provider or pharmacist about medicines that should not be taken with INVIRASE. For more information, see the section "Who should not take INVIRASE?" Read this Medication Guide before you start taking INVIRASE and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your healthcare provider about your medical condition or treatment. You and your healthcare provider should talk about your treatment with INVIRASE before you start taking it and at regular checkups. You should stay under a healthcare provider's care when taking INVIRASE. |
|||
| Also read the Medication Guide for ritonavir. | |||
What is the most important information I should know about INVIRASE?
|
|||
|
|
||
| See the section below "What are the possible side effects of INVIRASE?" for more information about serious side effects. | |||
| What is INVIRASE?
INVIRASE is a prescription medicine used with ritonavir and other antiretroviral medicines to treat Human Immunodeficiency Virus-1 (HIV-1) in people over 16 years of age. HIV is the virus that causes Acquired Immune Deficiency Syndrome (AIDS). In children under 16 years of age, INVIRASE doses that are both effective and safe could not be determined. |
|||
|
Do not take INVIRASE with ritonavir if you have the following conditions:
|
|||
| Taking INVIRASE with certain medicines can cause serious problems or life-threatening reactions. Do not take INVIRASE with ritonavir if you take any of the following medicines: |
|||
|
|
||
| Talk to your healthcare provider before taking any medicines listed above during treatment with INVIRASE and ritonavir. Though not complete, this is a list of medicines that should not be taken when INVIRASE is taken with ritonavir. | |||
Before taking INVIRASE, tell your healthcare provider about all of your medical conditions, including if you:
INVIRASE may affect the way other medicines work, and other medicines may affect how INVIRASE works.
|
|||
How should I take INVIRASE?
|
|||
|
What are the possible side effects of INVIRASE?
|
|||
|
|
||
|
|||
|
|
||
| These are not all of the possible side effects of INVIRASE. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. You may also report side effects to Genentech at 1-888-835-2555. |
|||
How should I store INVIRASE?
|
|||
| General information about the safe and effective use of INVIRASE.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use INVIRASE for a condition for which it was not prescribed. Do not give INVIRASE to other people even if they have the same condition you have. It may harm them. You can ask your pharmacist or healthcare provider for information about INVIRASE that is written for health professionals. |
|||
| Active ingredient: saquinavir mesylate Inactive ingredients: 500 mg Tablet: lactose, microcrystalline cellulose, povidone K30, croscarmellose sodium, and magnesium stearate. Film coat: hypromellose, titanium dioxide, talc, iron oxide yellow, iron oxide red, and triacetin. INVIRASE is a registered trademark of Hoffmann-La Roche Inc. Distributed by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 © 2020 Genentech, Inc. All rights reserved. For more information, go to http://www.gene.com/gene/products/information/invirase or call 1-877-436-3683. |
|||
Representative sample of labeling (see the HOW SUPPLIED section for complete listing):
PRINCIPAL DISPLAY PANEL - 500 mg Tablet Bottle Label
NDC 0004-0244-51
Invirase®
(saquinavir
mesylate) Tablets
500 mg
Each tablet contains saquinavir mesylate
equivalent to 500 mg saquinavir (free base).
ALERT: Find out about medicines that
should NOT be taken with INVIRASE.
Rx only
Attention Pharmacist: Dispense the
enclosed Medication Guide to each
patient. Do not cover ALERT box with
pharmacy label.
120 tablets
Genentech
10172487
| INVIRASE
saquinavir mesylate tablet, film coated |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| Labeler - Genentech, Inc. (080129000) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| F. Hoffmann-La Roche AG | 482242971 | API MANUFACTURE(0004-0244) , ANALYSIS(0004-0244) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| F. Hoffmann-La Roche Ltd | 485244961 | ANALYSIS(0004-0244) | |