LEVOTHYROXINE SODIUM- levothyroxine sodium tablet
REMEDYREPACK INC.
----------
DESCRIPTION
DESCRIPTIONLevothyroxine sodium tablets, USP contains synthetic crystalline L-3,3222,5,5222-tetraiodothyronine sodium salt [levothyroxine (T4)sodium]. Synthetic T4 is identical to that produced in the human thyroid gland.Levothyroxine (T4) sodium has an empirical formula of C15H10I4N NaO4 x H2O, molecular weight of 798.86 g/mol (anhydrous), andstructural formula as shown:
CLINICAL PHARMACOLOGY
CLINICAL PHARMACOLOGYThyroid hormone synthesis and secretion is regulated by the hypothalamic-pituitary-thyroid axis. Thyrotropin-releasing hormone(TRH) released from the hypothalamus stimulates secretion of thyrotropin-stimulating hormone, TSH, from the anterior pituitary.TSH, in turn, is the physiologic stimulus for the synthesis and secretion of thyroid hormones, L-thyroxine (T4) and L-triiodothyronine(T3), by the thyroid gland. Circulating serum T3 and T4 levels exert a feedback effect on both TRH and TSH secretion. When serumT3 and T4 levels increase, TRH and TSH secretion decrease. When thyroid hormone levels decrease, TRH and TSH secretionincrease.The mechanisms by which thyroid hormones exert their physiologic actions are not completely understood, but it is thought that theirprincipal effects are exerted through control of DNA transcription and protein synthesis. T3 and T4 diffuse into the cell nucleus andbind to thyroid receptor proteins attached to DNA. This hormone nuclear receptor complex activates gene transcription and synthesisof messenger RNA and cytoplasmic proteins. page 2 of 12 Thyroid hormones regulate multiple metabolic processes and play an essential role in normal growth and development, and normalmaturation of the central nervous system and bone. The metabolic actions of thyroid hormones include augmentation of cellularrespiration and thermogenesis, as well as metabolism of proteins, carbohydrates and lipids. The protein anabolic effects of thyroidhormones are essential to normal growth and development.The physiological actions of thyroid hormones are produced predominantly by T3, the majority of which (approximately 80%) isderived from T4 by deiodination in peripheral tissues.Levothyroxine, at doses individualized according to patient response, is effective as replacement or supplemental therapy inhypothyroidism of any etiology, except transient hypothyroidism during the recovery phase of subacute thyroiditis.Levothyroxine is also effective in the suppression of pituitary TSH secretion in the treatment or prevention of various typesof euthyroid goiters, including thyroid nodules, Hashimoto222s thyroiditis, multinodular goiter and, as adjunctive therapyin the management of thyrotropin-dependent well-differentiated thyroid cancer (seeINDICATIONS AND USAGE,
PHARMACOKINETICS
PHARMACOKINETICSAbsorption 226 Absorption of orally administered T4 from the gastrointestinal (GI) tract ranges from 40% to 80%. The majority of thelevothyroxine dose is absorbed from the jejunum and upper ileum. The relative bioavailability of this brand of Levothyroxine sodiumtablets, USP product, compared to an equal nominal dose of oral levothyroxine sodium solution, is approximately 99 %. T4 absorptionis increased by fasting, and decreased in malabsorption syndromes and by certain foods such as soybean infant formula. Dietaryfiber decreases bioavailability of T4. Absorption may also decrease with age. In addition, many drugs and foods affect T4 absorption(seePRECAUTIONS,
DRUG INTERACTIONS
Drug Interactions andDrug-Food Interactions).Distribution 226 Circulating thyroid hormones are greater than 99% bound to plasma proteins, including thyroxine-binding globulin(TBG), thyroxine-binding prealbumin (TBPA), and albumin (TBA), whose capacities and affinities vary for each hormone. The higheraffinity of both TBG and TBPA for T4 partially explains the higher serum levels, slower metabolic clearance, and longer half-life ofT4 compared to T3. Protein-bound thyroid hormones exist in reverse equilibrium with small amounts of free hormone. Only unboundhormone is metabolically active. Many drugs and physiologic conditions affect the binding of thyroid hormones to serum proteins(seePRECAUTIONS, Drug Interactions andDrug-Laboratory Test Interactions). Thyroid hormones do not readily cross theplacental barrier (seePRECAUTIONS,
WARNINGS
WARNINGSandPRECAUTIONS), including thyroid nodules (seeWARNINGS andPRECAUTIONS), subacute or chronic lymphocyticthyroiditis (Hashimoto222s thyroiditis), multinodular goiter (seeWARNINGS andPRECAUTIONS) and, as an adjunct to surgery andradioiodine therapy in the management of thyrotropin-dependent well-differentiated thyroid cancer. page 3 of 12
GERIATRIC USE
Geriatric Use, andDOSAGE AND ADMINISTRATION). If cardiac symptoms developor worsen, the levothyroxine dose should be reduced or withheld for one week and then cautiously restarted at a lower dose.Overtreatment with levothyroxine sodium may have adverse cardiovascular effects such as an increase in heart rate, cardiac wallthickness, and cardiac contractility and may precipitate angina or arrhythmias. Patients with coronary artery disease who arereceiving levothyroxine therapy should be monitored closely during surgical procedures, since the possibility of precipitating cardiacarrhythmias may be greater in those treated with levothyroxine. Concomitant administration of levothyroxine and sympathomimeticagents to patients with coronary artery disease may precipitate coronary insufficiency.Patients with nontoxic diffuse goiter or nodular thyroid disease- Exercise caution when administering levothyroxine to patientswith nontoxic diffuse goiter or nodular thyroid disease in order to prevent precipitation of thyrotoxicosis (seeWARNINGS). If theserum TSH is already suppressed, levothyroxine sodium should not be administered (seeCONTRAINDICATIONS).Associated endocrine disordersHypothalamic/pituitary hormone deficiencies- In patients with secondary or tertiary hypothyroidism, additional hypothalamic/pituitary hormone deficiencies should be considered, and, if diagnosed, treated (seePRECAUTIONS, Autoimmune polyglandularsyndrome for adrenal insufficiency).Autoimmune polyglandular syndromeOccasionally, chronic autoimmune thyroiditis may occur in association with other autoimmune disorders such as adrenalinsufficiency, pernicious anemia, and insulin-dependent diabetes mellitus. Patients with concomitant adrenal insufficiency should betreated with replacement glucocorticoids prior to initiation of treatment with levothyroxine sodium. Failure to do so may precipitatean acute adrenal crisis when thyroid hormone therapy is initiated, due to increased metabolic clearance of glucocorticoids by thyroid page 4 of 12 hormone. Patients with diabetes mellitus may require upward adjustments of their antidiabetic therapeutic regimens when treated withlevothyroxine (seePRECAUTIONS, Drug Interactions).Other associated medical conditionsInfants with congenital hypothyroidism appear to be at increased risk for other congenital anomalies, with cardiovascular anomalies(pulmonary stenosis, atrial septal defect, and ventricular septal defect) being the most common association.
INFORMATION FOR PATIENTS
Information for PatientsPatients should be informed of the following information to aid in the safe and effective use of Levothyroxine sodium tablets, USP:1.Notify your physician if you are allergic to any foods or medicines, are pregnant or intend to become pregnant, are breast-feedingor are taking any other medications, including prescription and over-the-counter preparations.2.Notify your physician of any other medical conditions you may have, particularly heart disease, diabetes, clotting disorders, andadrenal or pituitary gland problems. Your dose of medications used to control these other conditions may need to be adjustedwhile you are taking Levothyroxine sodium tablets, USP. If you have diabetes, monitor your blood and/or urinary glucose levelsas directed by your physician and immediately report any changes to your physician. If you are taking anticoagulants (bloodthinners), your clotting status should be checked frequently.3.Use Levothyroxine sodium tablets, USP only as prescribed by your physician. Do not discontinue or change the amount you takeor how often you take it, unless directed to do so by your physician.4.The levothyroxine in Levothyroxine sodium tablets, USP is intended to replace a hormone that is normally produced by yourthyroid gland. Generally, replacement therapy is to be taken for life, except in cases of transient hypothyroidism, which is usuallyassociated with an inflammation of the thyroid gland (thyroiditis).5.Take Levothyroxine sodium tablets, USP as a single dose, preferably on an empty stomach, one-half to one hour before breakfast.Levothyroxine absorption is increased on an empty stomach.6.Levothyroxine sodium tablets, USP may rapidly disintegrate. It is very important that you take the tablet with a full glass of water.7.It may take several weeks before you notice an improvement in your symptoms.8.Notify your physician if you experience any of the following symptoms: rapid or irregular heartbeat, chest pain, shortness ofbreath, leg cramps, headache, nervousness, irritability, sleeplessness, tremors, change in appetite, weight gain or loss, vomiting,diarrhea, excessive sweating, heat intolerance, fever, changes in menstrual periods, hives or skin rash, or any other unusualmedical event.9.Notify your physician if you become pregnant while taking Levothyroxine sodium tablets, USP. It is likely that your dose ofLevothyroxine sodium tablets, USP will need to be increased while you are pregnant.10.Notify your physician or dentist that you are taking Levothyroxine sodium tablets, USP prior to any surgery.11.Partial hair loss may occur rarely during the first few months of Levothyroxine sodium tablets, USP therapy, but this is usuallytemporary.12.Levothyroxine sodium tablets, USP should not be used as a primary or adjunctive therapy in a weight control program.13.Keep Levothyroxine sodium tablets, USP out of the reach of children. Store Levothyroxine sodium tablets, USP away from heat,moisture, and light.14.Agents such as iron and calcium supplements and antacids can decrease the absorption of levothyroxine sodium tablets. Therefore,levothyroxine sodium tablets should not be administered within 4 hrs of these agents.
NURSING MOTHERS
Nursing MothersAlthough thyroid hormones are excreted only minimally in human milk, caution should be exercised when Levothyroxine sodiumtablets, USP are administered to a nursing woman. However, adequate replacement doses of levothyroxine are generally needed tomaintain normal lactation.
PEDIATRIC USE
Pediatric UseGeneral The goal of treatment in pediatric patients with hypothyroidism is to achieve and maintain normal intellectual and physical growth anddevelopment.The initial dose of levothyroxine varies with age and body weight (seeDOSAGE AND ADMINISTRATION, Table 3). Dosingadjustments are based on an assessment of the individual patient222s clinical and laboratory parameters (seePRECAUTIONS,Laboratory Tests).In children in whom a diagnosis of permanent hypothyroidism has not been established, it is recommended that levothyroxineadministration be discontinued for a 30-day trial period, but only after the child is at least 3 years of age. Serum T4 and TSHlevels should then be obtained. If the T4 is low and the TSH high, the diagnosis of permanent hypothyroidism is established, andlevothyroxine therapy should be reinstituted. If the T4 and TSH levels are normal, euthyroidism may be assumed and, therefore,the hypothyroidism can be considered to have been transient. In this instance, however, the physician should carefully monitor the page 9 of 12 child and repeat the thyroid function tests if any signs or symptoms of hypothyroidism develop. In this setting, the clinician shouldhave a high index of suspicion of relapse. If the results of the levothyroxine withdrawal test are inconclusive, careful follow-up andsubsequent testing will be necessary.Since some more severely affected children may become clinically hypothyroid when treatment is discontinued for 30 days, analternate approach is to reduce the replacement dose of levothyroxine by half during the 30-day trial period. If, after 30 days, theserum TSH is elevated above 20 mU/L, the diagnosis of permanent hypothyroidism is confirmed, and full replacement therapy shouldbe resumed. However, if the serum TSH has not risen to greater than 20 mU/L, levothyroxine treatment should be discontinued foranother 30-day trial period followed by repeat serum T4 and TSH testing.The presence of concomitant medical conditions should be considered in certain clinical circumstances and, if present, appropriatelytreated (seePRECAUTIONS).Congenital Hypothyroidism ( seePRECAUTIONS, Laboratory Tests and DOSAGE and ADMINISTRATION)Rapid restoration of normal serum T4 concentrations is essential for preventing the adverse effects of congenital hypothyroidism onintellectual development as well as on overall physical growth and maturation. Therefore, Levothyroxine sodium tablets, USP therapyshould be initiated immediately upon diagnosis and is generally continued for life.During the first 2 weeks of Levothyroxine sodium tablets, USP therapy, infants should be closely monitored for cardiac overload,arrhythmias, and aspiration from avid suckling.The patient should be monitored closely to avoid undertreatment or overtreatment. Undertreatment may have deleterious effects onintellectual development and linear growth. Overtreatment has been associated with craniosynostosis in infants, and may adverselyaffect the tempo of brain maturation and accelerate the bone age with resultant premature closure of the epiphyses and compromisedadult stature.Acquired Hypothyroidism in Pediatric Patients The patient should be monitored closely to avoid undertreatment and overtreatment. Undertreatment may result in poor schoolperformance due to impaired concentration and slowed mentation and in reduced adult height. Overtreatment may accelerate the boneage and result in premature epiphyseal closure and compromised adult stature.Treated children may manifest a period of catch-up growth, which may be adequate in some cases to normalize adult height. Inchildren with severe or prolonged hypothyroidism, catch-up growth may not be adequate to normalize adult height.Geriatric UseBecause of the increased prevalence of cardiovascular disease among the elderly, levothyroxine therapy should not be initiated at thefull replacement dose (seeWARNINGS,PRECAUTIONS, andDOSAGE AND ADMINISTRATION).
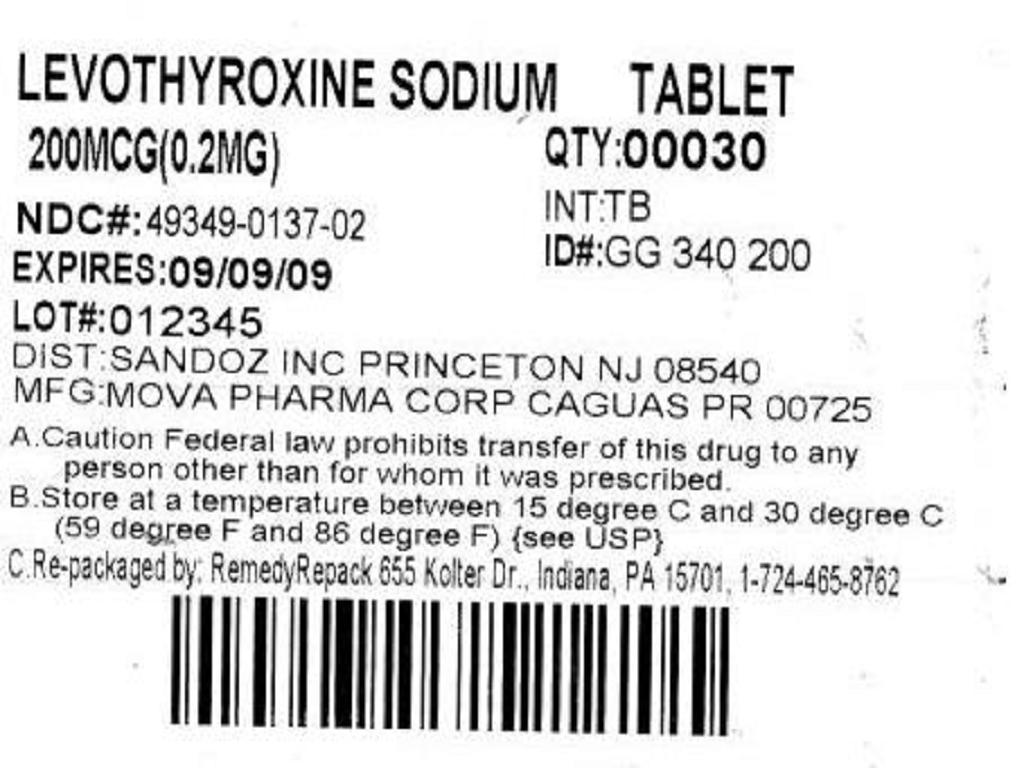

| LEVOTHYROXINE SODIUM
levothyroxine sodium tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - REMEDYREPACK INC. (829572556) |