Label: HUMALOG- insulin lispro injection, solution
HUMALOG PEN- insulin lispro injection, solution
HUMALOG CARTRIDGE- insulin lispro injection, solution



-
Contains inactivated NDC Code(s)
NDC Code(s): 54868-5108-0, 54868-5836-0, 54868-5899-0 - Packager: Physicians Total Care, Inc.
- This is a repackaged label.
- Source NDC Code(s): 0002-7510, 0002-7516, 0002-8725
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated May 22, 2012
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use HUMALOG safely and effectively. See full prescribing information for HUMALOG.
Humalog (insulin lispro injection, USP [rDNA origin]) for injection
Initial U.S. Approval: 1996RECENT MAJOR CHANGES
INDICATIONS AND USAGE
HUMALOG® is a rapid acting human insulin analog indicated to improve glycemic control in adults and children with diabetes mellitus. (1)
DOSAGE AND ADMINISTRATION
The dosage of HUMALOG must be individualized. (2.1)
Subcutaneous Injection
Administer within 15 minutes before a meal or immediately after a meal. Use in a regimen with an intermediate- or long-acting insulin. (2.2)
Continuous Subcutaneous Infusion Pump
Change the HUMALOG in the reservoir at least every 7 days, change the infusion set, and the infusion set insertion site at least every 3 days. HUMALOG must not be mixed or diluted when used in an external insulin infusion pump. (2.3)
DOSAGE FORMS AND STRENGTHS
HUMALOG 100 units/mL (U-100) is available as: (3)
- 10 mL vials
- 3 mL vials
- 3 mL prefilled pens
- 3 mL Humalog® KwikPen™ (prefilled)
- 3 mL cartridges
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Dose adjustment and monitoring: Closely monitor blood glucose in all patients treated with insulin. Change insulin regimens cautiously and only under medical supervision. (5.1)
- Hypoglycemia: Most common adverse reaction of insulin therapy and may be life-threatening. (5.2)
- Allergic reactions: Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with any insulin, including HUMALOG. (5.3)
- Hypokalemia: All insulins, including HUMALOG can cause hypokalemia, which if untreated, may result in respiratory paralysis, ventricular arrhythmia, and death. (5.4)
- Renal or hepatic impairment: Like all insulins, may require a reduction in the HUMALOG dose. (5.5)
- Mixing: HUMALOG for subcutaneous injection should not be mixed with insulins other than NPH insulin. Do not mix HUMALOG with any insulin for use in a continuous infusion pump. (5.6)
- Pump use: Select a new infusion site at least every 3 days and replace the HUMALOG in the pump reservoir at least every 7 days. (5.7)
ADVERSE REACTIONS
Adverse reactions associated with HUMALOG include hypoglycemia, allergic reactions, injection site reactions, lipodystrophy, pruritus, and rash. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Eli Lilly and Company at 1-800-LillyRx (1-800-545-5979) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
Pediatrics: Has not been studied in children with type 2 diabetes. Has not been studied in children with type 1 diabetes <3 years of age. (8.4)
See 17 for PATIENT COUNSELING INFORMATION, FDA-approved patient labeling and FDA-approved patient labeling.
Revised: 5/2012
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosage Considerations
2.2 Subcutaneous Administration
2.3 Continuous Subcutaneous Infusion (Insulin Pump)
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Dose Adjustment and Monitoring
5.2 Hypoglycemia
5.3 Hypersensitivity and Allergic Reactions
5.4 Hypokalemia
5.5 Renal or Hepatic Impairment
5.6 Mixing of Insulins
5.7 Subcutaneous Insulin Infusion Pumps
5.8 Drug Interactions
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and /or Pharmacology
14 CLINICAL STUDIES
14.1 Type 1 Diabetes — Adults and Adolescents
14.2 Type 2 Diabetes – Adults
14.3 Type 1 Diabetes – Pediatric and Adolescents
14.4 Type 1 Diabetes – Adults Continuous Subcutaneous Insulin Infusion
14.5 Type 1 Diabetes – Pediatric Continuous Subcutaneous Insulin Infusion
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage
16.3 Preparation and Handling
17 PATIENT COUNSELING INFORMATION
17.1 Instructions for All Patients
17.2 For Patients Using Continuous Subcutaneous Insulin Pumps
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Dosage Considerations
When given subcutaneously, HUMALOG has a more rapid onset of action and a shorter duration of action than regular human insulin.
The dosage of HUMALOG must be individualized. Blood glucose monitoring is essential in all patients receiving insulin therapy.
The total daily insulin requirement may vary and is usually between 0.5 to 1 unit/kg/day. Insulin requirements may be altered during stress, major illness, or with changes in exercise, meal patterns, or coadministered drugs.
2.2 Subcutaneous Administration
HUMALOG should be given within 15 minutes before a meal or immediately after a meal.
HUMALOG given by subcutaneous injection should generally be used in regimens with an intermediate- or long-acting insulin.
HUMALOG administered by subcutaneous injection should be given in the abdominal wall, thigh, upper arm, or buttocks. Injection sites should be rotated within the same region (abdomen, thigh, upper arm, or buttocks) from one injection to the next to reduce the risk of lipodystrophy [see Adverse Reactions (6.1)].
2.3 Continuous Subcutaneous Infusion (Insulin Pump)
HUMALOG may be administered by continuous subcutaneous infusion by an external insulin pump. Do not use diluted or mixed insulins in external insulin pumps. Infusion sites should be rotated within the same region to reduce the risk of lipodystrophy [see Adverse Reactions (6.1)]. Change the HUMALOG in the reservoir at least every 7 days, change the infusion sets and the infusion set insertion site at least every 3 days.
The initial programming of the external insulin infusion pump should be based on the total daily insulin dose of the previous regimen. Although there is significant variability among patients, approximately 50% of the total dose is usually given as meal-related boluses of HUMALOG and the remainder is given as a basal infusion. HUMALOG is recommended for use in pump systems suitable for insulin infusion such as MiniMed, Disetronic, and other equivalent pumps [see For Patients Using Continuous Subcutaneous Insulin Pumps (17.2)].
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Dose Adjustment and Monitoring
Glucose monitoring is essential for patients receiving insulin therapy. Changes to an insulin regimen should be made cautiously and only under medical supervision. Changes in insulin strength, manufacturer, type, or method of administration may result in the need for a change in insulin dose. Concomitant oral antidiabetic treatment may need to be adjusted.
As with all insulin preparations, the time course of action for HUMALOG may vary in different individuals or at different times in the same individual and is dependent on many conditions, including the site of injection, local blood supply, or local temperature. Patients who change their level of physical activity or meal plan may require adjustment of insulin dosages.
5.2 Hypoglycemia
Hypoglycemia is the most common adverse effect associated with insulins, including HUMALOG. The risk of hypoglycemia increases with tighter glycemic control. Patients must be educated to recognize and manage hypoglycemia. Hypoglycemia can happen suddenly and symptoms may be different for each person and may change from time to time. Severe hypoglycemia can cause seizures and may be life-threatening or cause death.
The timing of hypoglycemia usually reflects the time-action profile of the administered insulin formulations. Other factors such as changes in food intake (e.g., amount of food or timing of meals), injection site, exercise, and concomitant medications may also alter the risk of hypoglycemia [see Drug Interactions (7)].
As with all insulins, use caution in patients with hypoglycemia unawareness and in patients who may be predisposed to hypoglycemia (e.g., the pediatric population and patients who fast or have erratic food intake). The patient's ability to concentrate and react may be impaired as a result of hypoglycemia. This may present a risk in situations where these abilities are especially important, such as driving or operating other machinery.
Rapid changes in serum glucose levels may induce symptoms similar to hypoglycemia in persons with diabetes, regardless of the glucose value. Early warning symptoms of hypoglycemia may be different or less pronounced under certain conditions, such as longstanding diabetes, diabetic nerve disease, use of medications such as beta-blockers [see Drug Interactions (7)], or intensified diabetes control. These situations may result in severe hypoglycemia (and, possibly, loss of consciousness) prior to the patient's awareness of hypoglycemia.
5.3 Hypersensitivity and Allergic Reactions
Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with insulin products, including HUMALOG [see Adverse Reactions (6.1)].
5.4 Hypokalemia
All insulin products, including HUMALOG, cause a shift in potassium from the extracellular to intracellular space, possibly leading to hypokalemia. Untreated hypokalemia may cause respiratory paralysis, ventricular arrhythmia, and death. Use caution in patients who may be at risk for hypokalemia (e.g., patients using potassium-lowering medications, patients taking medications sensitive to serum potassium concentrations).
5.5 Renal or Hepatic Impairment
Frequent glucose monitoring and insulin dose reduction may be required in patients with renal or hepatic impairment [see Clinical Pharmacology (12.3)].
5.6 Mixing of Insulins
HUMALOG for subcutaneous injection should not be mixed with insulin preparations other than NPH insulin. If HUMALOG is mixed with NPH insulin, HUMALOG should be drawn into the syringe first. Injection should occur immediately after mixing.
Do not mix HUMALOG with other insulins for use in an external subcutaneous infusion pump.
5.7 Subcutaneous Insulin Infusion Pumps
When used in an external insulin pump for subcutaneous infusion, HUMALOG should not be diluted or mixed with any other insulin. Change the HUMALOG in the reservoir at least every 7 days, change the infusion sets and the infusion set insertion site at least every 3 days. HUMALOG should not be exposed to temperatures greater than 98.6°F (37°C).
Malfunction of the insulin pump or infusion set or insulin degradation can rapidly lead to hyperglycemia and ketosis. Prompt identification and correction of the cause of hyperglycemia or ketosis is necessary. Interim subcutaneous injections with HUMALOG may be required. Patients using continuous subcutaneous insulin infusion pump therapy must be trained to administer insulin by injection and have alternate insulin therapy available in case of pump failure [see Dosage and Administration (2.3), How Supplied/Storage and Handling (16), and Patient Counseling Information (17.2)].
5.8 Drug Interactions
Some medications may alter insulin requirements and the risk for hypoglycemia or hyperglycemia [see Drug Interactions (7)].
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed elsewhere:
- Hypoglycemia [see Warnings and Precautions (5.2)].
- Hypokalemia [see Warnings and Precautions (5.4)].
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying designs, the adverse reaction rates reported in one clinical trial may not be easily compared with those rates reported in another clinical trial, and may not reflect the rates actually observed in clinical practice.
The frequencies of Treatment-Emergent Adverse Events during HUMALOG clinical trials in patients with type 1 diabetes mellitus and type 2 diabetes mellitus are listed in the tables below.
Table 1: Treatment-Emergent Adverse Events in Patients with Type 1 Diabetes Mellitus (adverse events with frequency ≥5%) Events, n (%) Lispro
(n=81)Regular human insulin
(n=86)Total
(n=167)Flu syndrome 28 (34.6) 28 (32.6) 56 (33.5) Pharyngitis 27 (33.3) 29 (33.7) 56 (33.5) Rhinitis 20 (24.7) 25 (29.1) 45 (26.9) Headache 24 (29.6) 19 (22.1) 43 (25.7) Pain 16 (19.8) 14 (16.3) 30 (18.0) Cough increased 14 (17.3) 15 (17.4) 29 (17.4) Infection 11 (13.6) 18 (20.9) 29 (17.4) Nausea 5 (6.2) 13 (15.1) 18 (10.8) Accidental injury 7 (8.6) 10 (11.6) 17 (10.2) Surgical procedure 5 (6.2) 12 (14.0) 17 (10.2) Fever 5 (6.2) 10 (11.6) 15 (9.0) Abdominal pain 6 (7.4) 7 (8.1) 13 (7.8) Asthenia 6 (7.4) 7 (8.1) 13 (7.8) Bronchitis 6 (7.4) 6 (7.0) 12 (7.2) Diarrhea 7 (8.6) 5 (5.8) 12 (7.2) Dysmenorrhea 5 (6.2) 6 (7.0) 11 (6.6) Myalgia 6 (7.4) 5 (5.8) 11 (6.6) Urinary tract infection 5 (6.2) 4 (4.7) 9 (5.4) Table 2: Treatment-Emergent Adverse Events in Patients with Type 2 Diabetes Mellitus (adverse events with frequency ≥5%) Events, n (%) Lispro
(n=714)Regular human insulin
(n=709)Total
(n=1423)Headache 63 (11.6) 66 (9.3) 149 (10.5) Pain 77 (10.8) 71 (10.0) 148 (10.4) Infection 72 (10.1) 54 (7.6) 126 (8.9) Pharyngitis 47 (6.6) 58 (8.2) 105 (7.4) Rhinitis 58 (8.1) 47 (6.6) 105 (7.4) Flu syndrome 44 (6.2) 58 (8.2) 102 (7.2) Surgical procedure 53 (7.4) 48 (6.8) 101 (7.1) Insulin initiation and intensification of glucose control
Intensification or rapid improvement in glucose control has been associated with a transitory, reversible ophthalmologic refraction disorder, worsening of diabetic retinopathy, and acute painful peripheral neuropathy. However, long-term glycemic control decreases the risk of diabetic retinopathy and neuropathy.
Lipodystrophy
Long-term use of insulin, including HUMALOG, can cause lipodystrophy at the site of repeated insulin injections or infusion. Lipodystrophy includes lipohypertrophy (thickening of adipose tissue) and lipoatrophy (thinning of adipose tissue), and may affect insulin absorption. Rotate insulin injection or infusion sites within the same region to reduce the risk of lipodystrophy [see Dosage and Administration (2.2, 2.3)].
Weight gain
Weight gain can occur with insulin therapy, including HUMALOG, and has been attributed to the anabolic effects of insulin and the decrease in glucosuria.
Peripheral Edema
Insulin, including HUMALOG, may cause sodium retention and edema, particularly if previously poor metabolic control is improved by intensified insulin therapy.
Adverse Reactions with Continuous Subcutaneous Insulin Infusion (CSII)
In a 12-week, randomized, crossover study in adult patients with type 1 diabetes (n=39), the rates of catheter occlusions and infusion site reactions were similar for HUMALOG and regular human insulin treated patients (see Table 3).
Table 3: Catheter Occlusions and Infusion Site Reactions HUMALOG
(n=38)Regular human insulin
(n=39)Catheter occlusions/month 0.09 0.10 Infusion site reactions 2.6% (1/38) 2.6% (1/39) In a randomized, 16-week, open-label, parallel design study of children and adolescents with type 1 diabetes, adverse event reports related to infusion-site reactions were similar for insulin lispro and insulin aspart (21% of 100 patients versus 17% of 198 patients, respectively). In both groups, the most frequently reported infusion site adverse events were infusion site erythema and infusion site reaction.
Local Allergy — As with any insulin therapy, patients taking HUMALOG may experience redness, swelling, or itching at the site of the injection. These minor reactions usually resolve in a few days to a few weeks, but in some occasions, may require discontinuation of HUMALOG. In some instances, these reactions may be related to factors other than insulin, such as irritants in a skin cleansing agent or poor injection technique.
Systemic Allergy — Severe, life-threatening, generalized allergy, including anaphylaxis, may occur with any insulin, including HUMALOG. Generalized allergy to insulin may cause whole body rash (including pruritus), dyspnea, wheezing, hypotension, tachycardia, or diaphoresis.
In controlled clinical trials, pruritus (with or without rash) was seen in 17 patients receiving regular human insulin (n=2969) and 30 patients receiving HUMALOG (n=2944).
Localized reactions and generalized myalgias have been reported with injected metacresol, which is an excipient in HUMALOG [see Contraindications (4)].
Antibody Production
In large clinical trials with patients with type 1 (n=509) and type 2 (n=262) diabetes mellitus, anti-insulin antibody (insulin lispro-specific antibodies, insulin-specific antibodies, cross-reactive antibodies) formation was evaluated in patients receiving both regular human insulin and HUMALOG (including patients previously treated with human insulin and naive patients). As expected, the largest increase in the antibody levels occurred in patients new to insulin therapy. The antibody levels peaked by 12 months and declined over the remaining years of the study These antibodies do not appear to cause deterioration in glycemic control or necessitate an increase in insulin dose. There was no statistically significant relationship between the change in the total daily insulin dose and the change in percent antibody binding for any of the antibody types.
6.2 Postmarketing Experience
The following additional adverse reactions have been identified during post-approval use of HUMALOG. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Medication errors in which other insulins have been accidentally substituted for HUMALOG have been identified during postapproval use [see Patient Counseling Information (17)].
-
7 DRUG INTERACTIONS
A number of drugs affect glucose metabolism and may require insulin dose adjustment and particularly close monitoring.
Following are some of the examples:
- Drugs That May Increase the Blood-Glucose-Lowering Effect of HUMALOG and Susceptibility to Hypoglycemia: Oral antidiabetic agents, salicylates, sulfonamide antibiotics, monoamine oxidase inhibitors, fluoxetine, pramlintide, disopyramide, fibrates, propoxyphene, pentoxifylline, ACE inhibitors, angiotensin II receptor blocking agents, and somatostatin analogs (e.g., octreotide).
- Drugs That May Reduce the Blood-Glucose-Lowering Effect of HUMALOG: corticosteroids, isoniazid, niacin, estrogens, oral contraceptives, phenothiazines, danazol, diuretics, sympathomimetic agents (e.g., epinephrine, albuterol, terbutaline), somatropin, atypical antipsychotics, glucagon, protease inhibitors, and thyroid hormones.
- Drugs That May Increase or Reduce the Blood-Glucose-Lowering Effect of HUMALOG: beta-blockers, clonidine, lithium salts, and alcohol. Pentamidine may cause hypoglycemia, which may sometimes be followed by hyperglycemia.
- Drugs That May Reduce the Signs of Hypoglycemia: beta-blockers, clonidine, guanethidine, and reserpine.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category B. All pregnancies have a background risk of birth defects, loss, or other adverse outcome regardless of drug exposure. This background risk is increased in pregnancies complicated by hyperglycemia and may be decreased with good metabolic control. It is essential for patients with diabetes or history of gestational diabetes to maintain good metabolic control before conception and throughout pregnancy. In patients with diabetes or gestational diabetes insulin requirements may decrease during the first trimester, generally increase during the second and third trimesters, and rapidly decline after delivery. Careful monitoring of glucose control is essential in these patients. Therefore, female patients should be advised to tell their physicians if they intend to become, or if they become pregnant while taking HUMALOG.
Although there are limited clinical studies of the use of HUMALOG in pregnancy, published studies with human insulins suggest that optimizing overall glycemic control, including postprandial control, before conception and during pregnancy improves fetal outcome.
In a combined fertility and embryo-fetal development study, female rats were given subcutaneous insulin lispro injections of 5 and 20 units/kg/day (0.8 and 3 times the human subcutaneous dose of 1 unit/kg/day, based on units/body surface area, respectively) from 2 weeks prior to cohabitation through Gestation Day 19. There were no adverse effects on female fertility, implantation, or fetal viability and morphology. However, fetal growth retardation was produced at the 20 units/kg/day-dose as indicated by decreased fetal weight and an increased incidence of fetal runts/litter.
In an embryo-fetal development study in pregnant rabbits, insulin lispro doses of 0.1, 0.25, and 0.75 unit/kg/day (0.03, 0.08, and 0.24 times the human subcutaneous dose of 1 unit/kg/day, based on units/body surface area, respectively) were injected subcutaneously on Gestation days 7 through 19. There were no adverse effects on fetal viability, weight, and morphology at any dose.
8.3 Nursing Mothers
It is unknown whether insulin lispro is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when HUMALOG is administered to a nursing woman. Use of HUMALOG is compatible with breastfeeding, but women with diabetes who are lactating may require adjustments of their insulin doses.
8.4 Pediatric Use
HUMALOG is approved for use in children for subcutaneous daily injections and for subcutaneous continuous infusion by external insulin pump. HUMALOG has not been studied in pediatric patients younger than 3 years of age. HUMALOG has not been studied in pediatric patients with type 2 diabetes [see Clinical Studies (14)].
As in adults, the dosage of HUMALOG must be individualized in pediatric patients based on metabolic needs and results of frequent monitoring of blood glucose.
8.5 Geriatric Use
Of the total number of subjects (n=2834) in eight clinical studies of HUMALOG, twelve percent (n=338) were 65 years of age or over. The majority of these had type 2 diabetes. HbA1c values and hypoglycemia rates did not differ by age. Pharmacokinetic/pharmacodynamic studies to assess the effect of age on the onset of HUMALOG action have not been performed.
-
10 OVERDOSAGE
Excess insulin administration may cause hypoglycemia and hypokalemia. Mild episodes of hypoglycemia usually can be treated with oral glucose. Adjustments in drug dosage, meal patterns, or exercise may be needed. More severe episodes with coma, seizure, or neurologic impairment may be treated with intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate intake and observation may be necessary because hypoglycemia may recur after apparent clinical recovery. Hypokalemia must be corrected appropriately.
-
11 DESCRIPTION
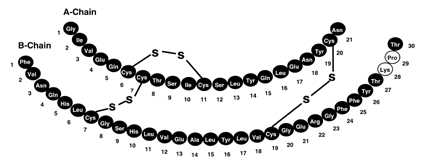
HUMALOG® (insulin lispro injection, USP [rDNA origin]) is a rapid-acting human insulin analog used to lower blood glucose. Insulin lispro is produced by recombinant DNA technology utilizing a non-pathogenic laboratory strain of Escherichia coli. Insulin lispro differs from human insulin in that the amino acid proline at position B28 is replaced by lysine and the lysine in position B29 is replaced by proline. Chemically, it is Lys(B28), Pro(B29) human insulin analog and has the empirical formula C257H383N65O77S6 and a molecular weight of 5808, both identical to that of human insulin.
HUMALOG has the following primary structure:
HUMALOG is a sterile, aqueous, clear, and colorless solution. Each milliliter of HUMALOG contains insulin lispro 100 units, 16 mg glycerin, 1.88 mg dibasic sodium phosphate, 3.15 mg Metacresol, zinc oxide content adjusted to provide 0.0197 mg zinc ion, trace amounts of phenol, and Water for Injection. Insulin lispro has a pH of 7.0 to 7.8. The pH is adjusted by addition of aqueous solutions of hydrochloric acid 10% and/or sodium hydroxide 10%.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Regulation of glucose metabolism is the primary activity of insulins and insulin analogs, including insulin lispro. Insulins lower blood glucose by stimulating peripheral glucose uptake by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulins inhibit lipolysis and proteolysis, and enhance protein synthesis.
12.2 Pharmacodynamics
HUMALOG has been shown to be equipotent to human insulin on a molar basis. One unit of HUMALOG has the same glucose-lowering effect as one unit of regular human insulin. Studies in normal volunteers and patients with diabetes demonstrated that HUMALOG has a more rapid onset of action and a shorter duration of activity than regular human insulin when given subcutaneously.
The time course of action of insulin and insulin analogs, such as HUMALOG, may vary considerably in different individuals or within the same individual. The parameters of HUMALOG activity (time of onset, peak time, and duration) as designated in Figure 1 should be considered only as general guidelines. The rate of insulin absorption, and consequently the onset of activity are known to be affected by the site of injection, exercise, and other variables [see Warnings and Precautions (5.1)].
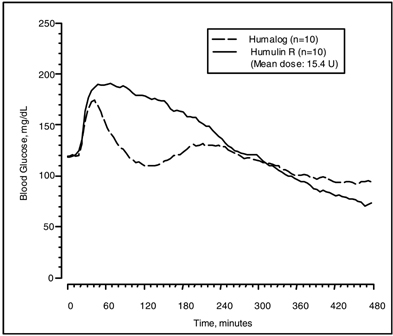
Figure 1: Blood Glucose Levels After Subcutaneous Injection of Regular Human Insulin or HUMALOG (0.2 unit/kg) Immediately Before a High Carbohydrate Meal in 10 Patients with Type 1 Diabetes.a
a Baseline insulin concentration was maintained by infusion of 0.2 mU/min/kg human insulin.
12.3 Pharmacokinetics
Absorption and Bioavailability — Studies in healthy volunteers and patients with diabetes demonstrated that HUMALOG is absorbed more quickly than regular human insulin. In healthy volunteers given subcutaneous doses of HUMALOG ranging from 0.1 to 0.4 unit/kg, peak serum levels were seen 30 to 90 minutes after dosing. When healthy volunteers received equivalent doses of regular human insulin, peak insulin levels occurred between 50 to 120 minutes after dosing. Similar results were seen in patients with type 1 diabetes (see Figure 2).
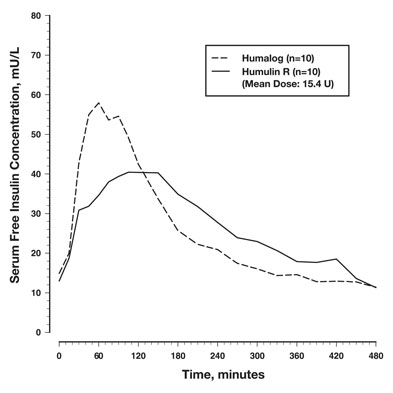
Figure 2: Serum HUMALOG and Insulin Levels After Subcutaneous Injection of Regular Human Insulin or HUMALOG (0.2 unit/kg) Immediately Before a High Carbohydrate Meal in 10 Patients with Type 1 Diabetes.a
a Baseline insulin concentration was maintained by infusion of 0.2 mU/min/kg human insulin.
HUMALOG was absorbed at a consistently faster rate than regular human insulin in healthy male volunteers given 0.2 unit/kg at abdominal, deltoid, or femoral subcutaneous sites. After HUMALOG was administered in the abdomen, serum drug levels were higher and the duration of action was slightly shorter than after deltoid or thigh administration. Bioavailability of HUMALOG is similar to that of regular human insulin. The absolute bioavailability after subcutaneous injection ranges from 55% to 77% with doses between 0.1 to 0.2 unit/kg, inclusive.
Distribution — After subcutaneous administration, the volume of distribution for HUMALOG is identical to that of regular human insulin, with a range of 0.26 to 0.36 L/kg. When administered intravenously, the volume of distribution of HUMALOG (range of 0.26 to 0.36 L/kg) was similar to that of regular human insulin (range of 0.32 to 0.67 L/kg).
Metabolism — Human metabolism studies have not been conducted. However, animal studies indicate that the metabolism of HUMALOG is identical to that of regular human insulin.
Elimination — After subcutaneous administration of HUMALOG, the t1/2 is shorter than that of regular human insulin (1 versus 1.5 hours, respectively). When administered intravenously, HUMALOG and regular human insulin demonstrated similar dose-dependent elimination, with a t1/2 of 0.44 hours (26 min) and 0.34 hours (20 min), respectively (0.1 unit/kg dose) and 0.86 hours (52 min) and 1.1 hours (66 min), respectively (0.2 unit/kg dose).
Age — The effect of age on the pharmacokinetics of HUMALOG has not been studied. However, in large clinical trials, sub-group analysis based on age did not indicate any difference in postprandial glucose parameters between HUMALOG and regular human insulin.
Gender — The effect of gender on the pharmacokinetics of HUMALOG has not been studied. However, in large clinical trials, sub-group analysis based on gender did not indicate any difference in postprandial glucose parameters between HUMALOG and regular human insulin.
Renal Impairment — Type 2 diabetic patients with varying degree of renal impairment showed no difference in pharmacokinetics of regular insulin and HUMALOG. However, the sensitivity of the patients to insulin did change, with an increased response to insulin as the renal function declined. Some studies with human insulin have shown increased circulating levels of insulin in patients with renal impairment. Careful glucose monitoring and dose adjustments of insulin, including HUMALOG, may be necessary in patients with renal dysfunction [see Warnings and Precautions (5.5)].
Hepatic Impairment — Type 2 diabetic patients with impaired hepatic function showed no effect on the pharmacokinetic of HUMALOG as compared to patients with no hepatic dysfunction. However, some studies with human insulin have shown increased circulating levels of insulin in patients with liver failure. Careful glucose monitoring and dose adjustments of insulin, including HUMALOG, may be necessary in patients with hepatic dysfunction.
Race – The effects of race on the pharmacokinetics and pharmacodynamics of HUMALOG have not been studied.
Obesity – The effect of obesity on the pharmacokinetics and pharmacodynamics of HUMALOG has not been studied.
Pregnancy – The effect of pregnancy on the pharmacokinetics and pharmacodynamics of HUMALOG has not been studied [see Use in Specific Populations (8.1)].
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Standard 2-year carcinogenicity studies in animals have not been performed. In Fischer 344 rats, a 12-month repeat-dose toxicity study was conducted with insulin lispro at subcutaneous doses of 20 and 200 units/kg/day (approximately 3 and 32 times the human subcutaneous dose of 1 unit/kg/day, based on units/body surface area). Insulin lispro did not produce important target organ toxicity including mammary tumors at any dose.
Insulin lispro was not mutagenic in the following genetic toxicity assays: bacterial mutation, unscheduled DNA synthesis, mouse lymphoma, chromosomal aberration and micronucleus assays.
Male fertility was not compromised when male rats given subcutaneous insulin lispro injections of 5 and 20 units/kg/day (0.8 and 3 times the human subcutaneous dose of 1 unit/kg/day, based on units/body surface area) for 6 months were mated with untreated female rats. In a combined fertility, perinatal, and postnatal study in male and female rats given 1, 5, and 20 units/kg/day subcutaneously (0.16, 0.8, and 3 times the human subcutaneous dose of 1 unit/kg/day, based on units/body surface area), mating and fertility were not adversely affected in either gender at any dose.
-
14 CLINICAL STUDIES
The safety and efficacy of HUMALOG were studied in children, adolescent, and adult patients with type 1 diabetes (n=789) and adult patients with type 2 diabetes (n=722).
14.1 Type 1 Diabetes — Adults and Adolescents
A 12-month, randomized, parallel, open-label, active-controlled study was conducted in patients with type 1 diabetes to assess the safety and efficacy of HUMALOG (n=81) compared with Humulin® R [REGULAR insulin human injection, USP (rDNA origin)] (n=86). HUMALOG was administered by subcutaneous injection immediately prior to meals and Humulin R was administered 30 to 45 minutes before meals. Humulin® U [ULTRALENTE® human insulin (rDNA origin) extended zinc suspension] was administered once or twice daily as the basal insulin. There was a 2- to 4-week run-in period with Humulin R and Humulin U before randomization. Most patients were Caucasian (97%). Forty-seven percent of the patients were male. The mean age was 31 years (range 12 to 70 years). Glycemic control, the total daily doses of HUMALOG and Humulin R, and the incidence of severe hypoglycemia (as determined by the number of events that were not self-treated) were similar in the two treatment groups. There were no episodes of diabetic ketoacidosis in either treatment group.
Table 4: Type 1 Diabetes Mellitus – Adults and Adolescents a Values are Mean ± SD
b Severe hypoglycemia refers to hypoglycemia for which patients were not able to self-treat.
Treatment Duration
Treatment in Combination with:12 months
Humulin UHUMALOG Humulin R N 81 86 Baseline HbA1c (%)a 8.2 ± 1.4 8.3 ± 1.7 Change from baseline HbA1c (%)a -0.1 ± 0.9 0.1 ± 1.1 Treatment Difference in HbA1c Mean (95% confidence interval) 0.4 (0.0, 0.8) Baseline short-acting insulin dose (units/kg/day) 0.3 ± 0.1 0.3 ± 0.1 End-of-Study short-acting insulin dose (units/kg/day) 0.3 ± 0.1 0.3 ± 0.1 Change from baseline short-acting insulin dose (units/kg/day) -0.0 ± 0.1 0.0 ±0.1 Baseline Body weight (kg) 72 ± 12.7 71 ± 11.3 Weight change from baseline (kg) 1.4 ± 3.6 1.0 ± 2.6 Patients with severe hypoglycemia (n, %)b 14 (17%) 18 (21%) 14.2 Type 2 Diabetes – Adults
A 6-month randomized, crossover, open-label, active-controlled study was conducted in insulin-treated patients with type 2 diabetes (n=722) to assess the safety and efficacy of HUMALOG for 3 months followed by Humulin R for 3 months or the reverse sequence. HUMALOG was administered by subcutaneous injection immediately before meals and Humulin R was administered 30 to 45 minutes before meals. Humulin® N [NPH human insulin (rDNA origin) isophane suspension] or Humulin U was administered once or twice daily as the basal insulin. All patients participated in a 2- to 4-week run-in period with Humulin R and Humulin N or Humulin U. Most of the patients were Caucasian (88%), and the numbers of men and women in each group were approximately equal. The mean age was 58.6 years (range 23.8 to 85 years). The average body mass index (BMI) was 28.2 kg/m2. During the study, the majority of patients used Humulin N (84%) compared with Humulin U (16%) as their basal insulin. The reductions from baseline in HbA1c and the incidence of severe hypoglycemia (as determined by the number of events that were not self-treated) were similar between the two treatments from the combined groups (see Table 5).
Table 5: Type 2 Diabetes Mellitus — Adults a Values are Mean ± SD
b Severe hypoglycemia refers to hypoglycemia for which patients were not able to self-treat.
End point Baseline HUMALOG
+
BasalHumulin R
+
BasalHbA1c (%)a 8.9 ± 1.7 8.2 ± 1.3 8.2 ± 1.4 Change from baseline HbA1c (%)a — -0.7 ± 1.4 -0.7 ± 1.3 Short-acting insulin dose (units/kg/day)a 0.3 ±0.2 0.3 ± 0.2 0.3 ±0.2 Change from baseline short-acting insulin dose (units/kg/day)a — 0.0 ± 0.1 0.0 ± 0.1 Body weight (kg)a 80 ± 15 81 ± 15 81 ±15 Weight change from baseline — 0.8 ± 2.7 0.9 ± 2.6 Patients with severe hypoglycemia (n, %)b — 15 (2%) 16 (2%) 14.3 Type 1 Diabetes – Pediatric and Adolescents
An 8-month, crossover study of adolescents with type 1 diabetes (n=463), aged 9 to 19 years, compared two subcutaneous multiple-dose treatment regimens: HUMALOG or Humulin R, both administered with Humulin N (NPH human insulin) as the basal insulin. HUMALOG achieved glycemic control comparable to Humulin R, as measured by HbA1c (see Table 6), and both treatment groups had a comparable incidence of hypoglycemia. In a 9-month, crossover study of prepubescent children (n=60) with type 1 diabetes, aged 3 to 11 years, HUMALOG administered immediately before meals, HUMALOG administered immediately after meals and Humulin R administered 30 minutes before meals resulted in similar glycemic control, as measured by HbA1c, and incidence of hypoglycemia, regardless of treatment group.
Table 6: Pediatric Subcutaneous Administration of HUMALOG in Type 1 Diabetes a Values are Mean ± SD
b Severe hypoglycemia refers to hypoglycemia that required glucagon or glucose injection or resulted in coma.
End point Baseline HUMALOG
+
NPHHumulin R
+
NPHHbA1c (%)a 8.6 ± 1.5 8.7 ± 1.5 8.7 ± 1.6 Change from baseline HbA1c (%)a — 0.1 ± 1.1 0.1 ± 1.3 Short-acting insulin dose (units/kg/day)a 0.5 ± 0.2 0.5 ± 0.2 0.5 ± 0.2 Change from baseline short-acting insulin dose (units/kg/day)a — 0.01 ± 0.1 -0.01 ± 0.1 Body weight (kg)a 59.1 ± 13.1 61.1 ± 12.7 61.4 ± 12.9 Weight change from baseline (kg)a — 2.0 ± 3.1 2.3 ± 3.0 Patients with severe hypoglycemia (n, %)b — 5 (1.1%) 5 (1.1%) Diabetic ketoacidosis (n, %) — 11 (2.4%) 9 (1.9%) 14.4 Type 1 Diabetes – Adults Continuous Subcutaneous Insulin Infusion
To evaluate the administration of HUMALOG via external insulin pumps, two open-label, crossover design studies were performed in patients with type 1 diabetes. One study involved 39 patients, ages 19 to 58 years, treated for 24 weeks with HUMALOG or regular human insulin. After 12 weeks of treatment, the mean HbA1c values decreased from 7.8% to 7.2% in the HUMALOG-treated patients and from 7.8% to 7.5% in the regular human insulin-treated patients. Another study involved 60 patients (mean age 39, range 15 to 58 years) treated for 24 weeks with either HUMALOG or buffered regular human insulin. After 12 weeks of treatment, the mean HbA1c values decreased from 7.7% to 7.4% in the HUMALOG-treated patients and remained unchanged from 7.7% in the buffered regular human insulin-treated patients. Rates of hypoglycemia were comparable between treatment groups in both studies.
14.5 Type 1 Diabetes – Pediatric Continuous Subcutaneous Insulin Infusion
A randomized, 16-week, open-label, parallel design, study of children and adolescents with type 1 diabetes (n=298) aged 4 to 18 years compared two subcutaneous infusion regimens administered via an external insulin pump: insulin aspart (n=198) or HUMALOG (n=100). These two treatments resulted in comparable changes from baseline in HbA1c and comparable rates of hypoglycemia after 16 weeks of treatment (see Table 7). Infusion site reactions were similar between groups.
Table 7: Pediatric Insulin Pump Study in Type 1 Diabetes (16 weeks; n=298) a Values are Mean ± SD
b Severe hypoglycemia refers to hypoglycemia associated with central nervous system symptoms and requiring the intervention of another person or hospitalization.
HUMALOG Aspart N 100 198 Baseline HbA1c (%)a 8.2 ± 0.8 8.0 ± 0.9 Change from Baseline HbA1c (%) -0.1 ± 0.7 -0.1 ± 0.8 Treatment Difference in HbA1c, Mean (95% confidence interval) 0.1 (-0.3, 0.1) Baseline insulin dose (units/kg/24 hours)a 0.9 ± 0.3 0.9 ± 0.3 End-of-Study insulin dose (units/kg/24 hours)a 0.9 ± 0.2 0.9 ± 0.2 Patients with severe hypoglycemia (n, %)b 8 (8%) 19 (10%) Diabetic ketoacidosis (n, %) 0 (0) 1 (0.5%) Baseline body weight (kg)a 55.5 ± 19.0 54.1 ± 19.7 Weight Change from baseline (kg)a 1.6 ± 2.1 1.8 ± 2.1 -
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
HUMALOG 100 units per mL (U-100) is available as:
10 mL vials NDC 54868-5108-0 (VL-7510) 5 x 3 mL cartridges1 NDC 54868-5836-0 (VL-7516) 5 x 3 mL prefilled pen NDC 54868-5899-0 (HP-8725) 16.2 Storage
Do not use after the expiration date.
Unopened HUMALOG should be stored in a refrigerator (36° to 46°F [2° to 8°C]), but not in the freezer. Do not use HUMALOG if it has been frozen. In-use HUMALOG vials, cartridges, pens, and HUMALOG KwikPen® should be stored at room temperature, below 86°F (30°C) and must be used within 28 days or be discarded, even if they still contain HUMALOG. Protect from direct heat and light. See table below:
Not In-Use (Unopened) Room Temperature (Below 86°F [30°C]) Not In-Use (Unopened) Refrigerated In-Use (Opened) Room Temperature, (Below 86°F [30°C]) 10 mL vial 28 days Until expiration date 28 days, refrigerated/room temperature. 3 mL vial 28 days Until expiration date 28 days, refrigerated/room temperature. 3 mL cartridge 28 days Until expiration date 28 days, Do not refrigerate. 3 mL prefilled pen 28 days Until expiration date 28 days, Do not refrigerate. 3 mL Humalog KwikPen (prefilled) 28 days Until expiration date 28 days, Do not refrigerate. Use in an External Insulin Pump — Change the HUMALOG in the reservoir at least every 7 days, change the infusion sets and the infusion set insertion site at least every 3 days or after exposure to temperatures that exceed 98.6°F (37°C). A HUMALOG 3 mL cartridge used in the D-Tron pumps should be discarded after 7 days, even if it still contains HUMALOG. However, as with other external insulin pumps, the infusion set should be replaced and a new infusion set insertion site should be selected at least every 3 days.
16.3 Preparation and Handling
Diluted HUMALOG for Subcutaneous Injection — HUMALOG may be diluted with Sterile Diluent for HUMALOG for subcutaneous injection. Diluting one part HUMALOG to nine parts diluent will yield a concentration one-tenth that of HUMALOG (equivalent to U-10). Diluting one part HUMALOG to one part diluent will yield a concentration one-half that of HUMALOG (equivalent to U-50).
-
17 PATIENT COUNSELING INFORMATION
See FDA-approved patient labeling.
17.1 Instructions for All Patients
Patients should be instructed on self-management procedures including glucose monitoring, proper injection technique, and management of hypoglycemia and hyperglycemia. Patients must be instructed on handling of special situations such as intercurrent conditions (illness, stress, or emotional disturbances), an inadequate or skipped insulin dose, inadvertent administration of an increased insulin dose, inadequate food intake, and skipped meals. Refer patients to the HUMALOG Patient Information Leaflet for additional information.
Women with diabetes should be advised to inform their doctor if they are pregnant or are contemplating pregnancy.
Accidental mix-ups between HUMALOG and other insulins have been reported. To avoid medication errors between HUMALOG and other insulins, patients should be instructed to always check the insulin label before each injection.
17.2 For Patients Using Continuous Subcutaneous Insulin Pumps
Patients using external pump infusion therapy should be trained appropriately.
The following insulin pumps have been tested in HUMALOG clinical trials conducted by Eli Lilly and Company.
- Disetronic® H-Tron® plus V100, D-Tron® and D-Tronplus® with Disetronic Rapid infusion sets2
- MiniMed® Models 506, 507 and 508 and Polyfin® infusion sets3
HUMALOG is recommended for use in pump systems suitable for insulin infusion such as MiniMed, Disetronic, and other equivalent pumps. Before using HUMALOG in a pump system, read the pump label to make sure the pump is indicated for continuous delivery of fast-acting insulin. HUMALOG is recommended for use in any reservoir and infusion sets that are compatible with insulin and the specific pump. Please see recommended reservoir and infusion sets in the pump manual.
To avoid insulin degradation, infusion set occlusion, and loss of the preservative (metacresol), insulin in the reservoir should be replaced at least every 7 days; infusion sets and infusion set insertion sites should be changed at least every 3 days.
Insulin exposed to temperatures higher than 98.6°F (37°C) should be discarded. The temperature of the insulin may exceed ambient temperature when the pump housing, cover, tubing or sport case is exposed to sunlight or radiant heat. Infusion sites that are erythematous, pruritic, or thickened should be reported to the healthcare professional, and a new site selected because continued infusion may increase the skin reaction or alter the absorption of HUMALOG.
Pump or infusion set malfunctions or insulin degradation can lead to rapid hyperglycemia and ketosis. This is especially pertinent for rapid acting insulin analogs that are more rapidly absorbed through skin and have a shorter duration of action. Prompt identification and correction of the cause of hyperglycemia or ketosis is necessary. Problems include pump malfunction, infusion set occlusion, leakage, disconnection or kinking, and degraded insulin. Less commonly, hypoglycemia from pump malfunction may occur. If these problems cannot be promptly corrected, patients should resume therapy with subcutaneous insulin injection and contact their healthcare professionals. [See Dosage and Administration (2.3), Warnings and Precautions (5.7), and How Supplied/Storage and Handling (16)].
____________
1 3 mL cartridge is for use in Eli Lilly and Company's HumaPen® Memoir™ and HumaPen® Luxura™ HD insulin delivery devices, Owen Mumford, Ltd.'s Autopen® 3-mL insulin delivery device and Disetronic D-TRON® and D-TRON® Plus pumps.
Autopen® is a registered trademark of Owen Mumford, Ltd.
Humalog®, Humalog® KwikPen™, HumaPen®, HumaPen® Memoir™, HumaPen® Luxura™ and HumaPen® Luxura™ HD are trademarks of Eli Lilly and Company.
2 Disetronic®, H-Tron®, D-Tron®, and D-Tronplus® are registered trademarks of Roche Diagnostics GmbH.
3 MiniMed® and Polyfin® are registered trademarks of MiniMed, Inc.
Other product and company names may be the trademarks of their respective owners.
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
Patient Information
HUMALOG®
insulin lispro injection, USP (rDNA origin)
Read the “Patient Information” that comes with HUMALOG (HU-ma-log) before you start using it and each time you get a refill. There may be new information. This leaflet does not take the place of talking with your healthcare provider about your diabetes or treatment. If you have questions about HUMALOG or diabetes, talk with your healthcare provider.
What is the most important information I should know about HUMALOG?
- Do not change the insulin you use without talking to your healthcare provider. Any change in insulin strength, manufacturer, type (regular, NPH, analog) may need a change in the dose you are using. This dose change may be needed right away or later on. Sometimes this dose change may happen during the first several weeks or months on the new insulin. Doses of oral anti-diabetic medicines may also need to change if your insulin is changed.
- You must test your blood sugar levels while using an insulin such as HUMALOG. Your healthcare provider will tell you how often you should test your blood sugar level, and what to do if it is high or low.
- When used in a pump do not mix HUMALOG with any other insulin or liquid.
What is HUMALOG?
HUMALOG (insulin lispro injection, USP [rDNA origin]) is an injectable rapid-acting man-made insulin. HUMALOG is used to treat people with diabetes for the control of high blood sugar.
- HUMALOG is a clear, colorless, sterile solution for injection under the skin (subcutaneously).
- You need a prescription to get HUMALOG. Always be sure you receive the right insulin from the pharmacy.
HUMALOG comes in:
- 10 mL vials (bottles) for use with a syringe or external insulin pump
- 3 mL vials (bottles) for use with a syringe or external insulin pump
- 3 mL prefilled pens
- 3 mL Humalog® KwikPen™
- 3 mL cartridges for use with a reusable pen or external insulin pump
Who should not take HUMALOG?
Do not take HUMALOG if:
- your blood sugar is too low (hypoglycemia). After treating your low blood sugar, follow your healthcare provider's instructions on the use of HUMALOG.
- you are allergic to insulin lispro or any of the ingredients in HUMALOG. See the end of this leaflet for a complete list of ingredients in HUMALOG. Check with your healthcare provider if you are not sure.
What should I tell my healthcare provider before taking HUMALOG?
Tell your healthcare provider:
- about all your medical conditions, including liver or kidney problems. Your dose may need to be adjusted.
- if you are pregnant or breastfeeding. You and your healthcare provider should talk about the best way to manage your diabetes while you are pregnant or breastfeeding. HUMALOG has not been studied in pregnant or nursing women.
- about all the medicines you take, including prescription and non-prescription medicines, vitamins and herbal supplements. Your HUMALOG dose may need to change if you take other medicines.
Know the medicines you take. Keep a list of your medicines with you to show your healthcare providers when you get a new medicine.
How should I use HUMALOG?
HUMALOG can be used with a syringe, prefilled pen, reusable pen or external insulin pump. Talk to your healthcare provider if you have any questions.
- Read the instructions for use that comes with your HUMALOG product. Talk to your healthcare provider if you have any questions. Your healthcare provider should show you how to inject HUMALOG before you start taking it.
- HUMALOG is a rapid-acting insulin. You should take HUMALOG within fifteen minutes before eating or right after eating a meal.
- Only use HUMALOG that is clear and colorless. If your HUMALOG is cloudy, colored, or has solid particles or clumps in it, return it to your pharmacy for a replacement.
-
Do not mix HUMALOG:
- with any type of insulin other than NPH when used with injections by syringe.
- with any other insulin or liquid when used in a pump.
- If your doctor recommends diluting HUMALOG, follow your doctor's instructions exactly so that you know:
- How to make HUMALOG more dilute (that is, a smaller number of units of HUMALOG for a given amount of liquid) and
- How to use this more dilute form of HUMALOG. Do not use dilute insulin in a pump.
- Inject HUMALOG under your skin (subcutaneously) in your upper arm, abdomen (stomach area), thigh (upper leg), or buttocks. Never inject it into a vein or muscle.
- Change (rotate) your injection site with each dose.
- If you have type 1 diabetes, you need to take a longer-acting insulin in addition to HUMALOG (except when using an external insulin pump).
- If you have type 2 diabetes, you may be taking oral anti-diabetic medicines and/or a longer-acting insulin in addition to HUMALOG.
- Follow the instructions given by your healthcare provider about the type or types of insulin you are using. Do not make any changes with your insulin unless you have talked to your healthcare provider. Always make sure that you received the correct type of HUMALOG from the pharmacy. Check to make sure you are injecting the correct insulin and dose, especially if you use other insulin with HUMALOG.
- If you take too much HUMALOG, your blood sugar may fall low (hypoglycemia). You can treat mild low blood sugar by drinking or eating something sugary right away (fruit juice, sugar candies, or glucose tablets). It is important to treat low blood sugar right away because it could get worse and you could pass out (become unconscious). If you pass out, you will need help from another person or emergency medical services right away, and will need treatment with glucagon injection or treatment at a hospital. See “What are the possible side effects of HUMALOG?” for more information on low blood sugar.
-
If you forget to take your dose of HUMALOG, your blood sugar may go too high (hyperglycemia). If high blood sugar is not treated it can lead to serious problems like loss of consciousness (passing out), coma or even death. Follow your healthcare provider's instructions for treating high blood sugar. Know your symptoms of high blood sugar which may include:
- increased thirst
- frequent urination
- drowsiness
- loss of appetite
- a hard time breathing
- fruity smell on the breath
- high amounts of sugar and ketones in your urine
- nausea, vomiting (throwing up) or stomach pain
-
Your insulin dosage may need to change because of:
- illness
- stress
- other medicines you take
- change in diet
- change in physical activity or exercise
What are the possible side effects of HUMALOG?
-
low blood sugar (hypoglycemia). Symptoms of low blood sugar may include:
- sweating
- dizziness or lightheadedness
- shakiness
- hunger
- fast heart beat
- tingling of lips and tongue
- trouble concentrating or confusion
- blurred vision
- slurred speech
- anxiety, irritability or mood changes
- headache
- Severe low blood sugar can cause unconsciousness (passing out), seizures, and death. Low blood sugar may affect your ability to drive a car or use mechanical equipment, risking injury to yourself or others. Know your symptoms of low blood sugar. Follow your healthcare provider's instructions for treating low blood sugar. Talk to your healthcare provider if low blood sugar is a problem for you.
- Serious allergic reaction (whole body reaction). Get medical help right away, if you develop a rash over your whole body, have trouble breathing, a fast heartbeat, or sweating.
- Reactions at the injection site (local allergic reaction). You may get redness, swelling, and itching at the injection site. If you keep having skin reactions or they are serious, talk to your healthcare provider. You may need to stop using HUMALOG and use a different insulin. Do not inject insulin to skin that is red, swollen or itchy.
- Skin thickens or pits at the injection site (lipodystrophy). Change (rotate) when you inject your insulin to help to prevent these skin changes from happening. Do not inject insulin into this type of skin.
- Swelling of your hands and feet
- Low potassium in your blood (hypokalemia)
- Weight gain
These are not all of the possible side effects from HUMALOG. Ask your healthcare provider or pharmacist for more information.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store HUMALOG?
- Store all unopened (unused) HUMALOG in the original carton in a refrigerator at 36°F to 46°F (2°C to 8°C).
- Do not freeze. Do not use HUMALOG if it has been frozen.
- Keep unopened HUMALOG in the carton to protect from light.
After starting use (open)
Vials:
- Keep in the refrigerator or at room temperature below 86°F (30°C) for up to 28 days.
- Keep vials away from direct heat or light.
- Throw away an opened vial after 28 days of use, even if there is insulin left in the vial.
- Unopened vials can be used until the expiration date on the HUMALOG carton and label, if the medicine has been stored in a refrigerator.
Cartridge and Prefilled Pens:
- Keep at room temperature below 86°F (30°C) for up to 28 days.
- Do not store a cartridge or prefilled pen that you are using in the refrigerator.
- Keep cartridges and prefilled pens away from direct heat or light.
- A cartridge used in the D-Tron1 or D-Tronplus1 pump may be used for up to 7 days.
- Throw away a used cartridge or prefilled pen after 28 days, even if there is insulin left in the cartridge or the pen.
General Information about HUMALOG
-
HUMALOG in the pump reservoir and the complete external pump infusion set:
- When HUMALOG is used in pumps, use only pumps that are recommended by your healthcare provider.
- The infusion set and infusion site should be changed at least every 3 days.
- The insulin in the reservoir should be changed at least every 7 days even if you have not used all of the insulin.
- Change the infusion set and infusion site more often than every 3 days if you have high blood sugar (hyperglycemia), the pump alarms sounds, or the insulin flow is blocked (occlusion).
- Do not use HUMALOG for a condition for which it was not prescribed. Do not give or share HUMALOG with another person, even if they also have diabetes. It may harm them.
- This leaflet summarizes the most important information about HUMALOG. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider for information about HUMALOG that is written for healthcare providers. For more information about HUMALOG, call 1-800-LillyRx (1-800-545-5979) or visit www.humalog.com.
What are the ingredients in HUMALOG?
insulin lispro, glycerin, dibasic sodium phosphate, metacresol, zinc oxide (zinc ion), trace amounts of phenol and water for injection.
Helpful information for people with diabetes is published by the American Diabetes Association, 1660 Duke Street, Alexandria, VA 22314 and on www.diabetes.org.
__________
1 D-Tron®, D-Tronplus® are registered trademarks of Roche Diagnostics GmbH.
Humalog® and Humalog® KwikPen™ are registered trademarks of Eli Lilly and Company.
Patient Information revised May 23, 2011
Marketed by: Lilly USA, LLC, Indianapolis, IN 46285, USA
www.humalog.com
Copyright © 2007, 2011, Eli Lilly and Company. All rights reserved.
PV 5564 AMP
-
PATIENT PACKAGE INSERT
Humalog® KwikPen™
insulin lispro injection, USP (rDNA origin)Disposable Insulin Delivery Device
User Manual________________________________________________________________________________________

Introduction
Humalog® KwikPen™ (“Pen”) is designed for ease of use. It is a disposable insulin delivery device (“insulin Pen”) containing 3 mL (300 units) of U-100 Humalog® [insulin lispro injection, USP (rDNA origin)] insulin. You can inject from 1 to 60 units of Humalog in one injection. You can dial your dose one unit at a time. If you dial too many units, you can dial backwards to correct the dose without wasting any insulin.
Before using Humalog KwikPen, read the entire manual completely and follow the directions carefully. If you do not follow these directions completely, you may get too much or too little insulin.
Do not share your Humalog KwikPen or needles with anyone else. You may give an infection to them or get an infection from them.
DO NOT USE your KwikPen if any part appears broken or damaged. Contact Lilly at 1-800-Lilly-Rx (1-800-545-5979) or your healthcare professional for a replacement Pen. Always carry an extra Pen in case yours is lost or damaged.
This Pen is not recommended for use by the blind or visually impaired persons without the assistance of a person trained in the proper use of the product.Preparing Humalog KwikPen
Important Notes
- Read and follow the directions provided in the Patient Information Leaflet.
- Check the label on your Pen before each injection for the expiration date and to make sure you are using the correct type of insulin.
- Your healthcare professional has prescribed the best type of insulin for you. Any changes in insulin therapy should be made only under medical supervision.
- KwikPen is recommended for use with Becton, Dickinson and Company pen needles.
- Be sure the needle is completely attached to the Pen before use.
- Do not share your Pen or needles.
- Keep these directions for future reference.
Frequently Asked Questions about Preparing Humalog KwikPen
- What should my insulin look like? Humalog is clear and colorless. If your Humalog is cloudy, colored, or has solid particles or clumps in it, return it to your pharmacy for a replacement. Be sure to refer to your Patient Information Leaflet for the appearance of your specific insulin.
- Why should I use a new needle for each injection? This will help ensure sterility. If needles are reused, you may get the wrong amount of insulin, a clogged needle or a jammed Pen.
- What should I do if I am not sure how much insulin remains in my cartridge? Hold the Pen with the needle end pointing down. The scale on the clear Cartridge Holder shows an estimate of the number of units remaining. These numbers should NOT be used for measuring an insulin dose.
Priming Humalog KwikPen
Important Notes
- Prime every time. The Pen must be primed to a stream of insulin before each injection to make sure the Pen is ready to dose.
- If you do not prime, you may get too much or too little insulin.
Frequently Asked Questions about Priming
-
Why should I prime my KwikPen before each dose?
- Ensures that the Pen is ready to dose.
- Confirms that a stream of insulin comes out of the tip of the needle when you push the Dose Knob in.
- Removes air that may collect in the needle or insulin cartridge during normal use.
-
What should I do if I cannot completely push in the Dose Knob when priming the KwikPen?
- Attach a new needle.
- Prime the Pen.
- What should I do if I see an air bubble in the cartridge? You need to prime the Pen. Remember, do not store the Pen with the needle attached as this may cause air bubbles to collect in the insulin cartridge. A small air bubble will not affect your dose and you can continue to take your dose as usual.
Injecting Your Dose
Important Notes
- Follow the instructions for sanitary injection technique recommended by your healthcare professional.
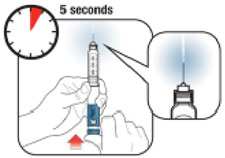
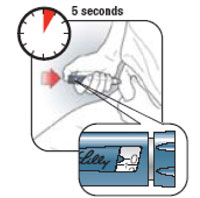
- Make sure you receive your complete dose by pushing and holding the dose knob in and count to 5 slowly before removing the needle. If insulin is leaking from the Pen you may not have held it in your skin long enough.
- The Pen will not allow you to dial more than the number of units left in the Pen.
- If your dose is greater than the number of units left in the Pen, you may either inject the amount remaining in your current Pen and then use a new Pen to complete your dose OR inject the full dose with a new Pen.
- Do not attempt to inject your insulin by turning the Dose Knob. You will NOT receive your insulin by turning the Dose Knob. You must PUSH the Dose Knob straight in for the dose to be delivered.
- Do not attempt to change the dose while injecting.
- The directions regarding needle handling are not intended to replace local, healthcare professional or institutional policies.
- Remove the needle after completing each injection.
Frequently Asked Questions about Injecting Your Dose
-
Why is it difficult to push the Dose Knob when I try to inject?
- Your needle may be clogged. Try attaching a new needle. When you do this you may see insulin come out of the needle. Then prime the Pen.
- Pressing the Dose Knob quickly may make the Dose Knob harder to push. Pressing the Dose Knob more slowly may make it easier.
- Using a larger diameter needle will make it easier to push the Dose Knob during your injection. See your healthcare professional to determine which needle size is best for you.
- If the Dose Knob continues to be difficult to push after following the steps above, try the steps below under “What should I do if my KwikPen is jammed?”.
-
What should I do if my KwikPen is jammed? Your Pen may be jammed if it is difficult to inject a dose or dial a dose. To clear the jam:
- Attach a new needle. When you do this you may see insulin come out of the needle.
- Prime the Pen.
- Dial your dose and inject.
- If the Dose Knob is still difficult to push, contact Lilly at 1-800-Lilly-Rx
(1-800-545-5979).
-
Why is insulin leaking from the needle after I finished injecting my dose? You may have removed the needle from your skin too quickly.
- Make sure you see a 0 in the Dose Window to confirm you received the complete dose.
- For the next dose, push and hold the Dose Knob in and count to 5 slowly before removing the needle.
-
What should I do if my dose is dialed and the Dose Knob is accidentally pushed in without a needle attached?
- Dial back to zero.
- Attach a new needle. When you do this you may see insulin come out of the needle.
- Prime the Pen.
- Dial your dose and inject.
- What should I do if I dial a wrong dose (too high or too low)? Turn the Dose Knob backward or forward to correct the dose before injecting.
- What should I do if I see insulin leaking from the KwikPen needle while dialing the dose or correcting the dose? Do not inject the dose because you may not get your complete dose. Dial the Pen down to zero and prime the Pen again (see “Priming Humalog KwikPen” steps 2 B-D). Dial your dose and inject.
-
What should I do if my full dose cannot be dialed? The Pen will not allow you to dial a dose greater than the number of insulin units remaining in the cartridge. For example, if you need 31 units and only 25 units remain in the cartridge you will not be able to dial past 25. Do not attempt to dial past this point. You may either:
- Inject the partial dose and then inject the remaining dose using a new Pen.
or
- Inject the full dose with a new Pen.
- Inject the partial dose and then inject the remaining dose using a new Pen.
- Why can I not dial the dose to use the small amount of insulin that remains in my cartridge? The Pen is designed to deliver at least 300 units of insulin. The Pen design prevents the cartridge from being completely emptied because the small amount of insulin that remains in the cartridge cannot be delivered.
Storage and Disposal
Important Notes
- Refer to the Patient Information Leaflet for complete insulin storage instructions.
- Pens that have not been used should be stored in a refrigerator but not in a freezer. Do not use a Pen if it has been frozen.
- Do not store the Pen with the needle attached. If the needle remains attached, insulin may leak from the Pen, insulin may dry inside the needle causing the needle to clog, or air bubbles may form inside the cartridge.
- The Pen you are currently using should be kept at room temperature and away from heat and light.
- Keep the Pen out of the reach of children.
- Dispose of used needles in a puncture-resistant container or as directed by your healthcare professional.
- Dispose of used Pens as instructed by your healthcare professional and without the needle attached.
Use the space below to keep track of how long you should use each Pen in the carton. Once you start using a KwikPen it must be thrown out after the number of days listed in your Patient Information Leaflet, even if there is insulin remaining in the Pen. Record the date you start using a Pen, find the number of days that KwikPen should be used in the Patient Information Leaflet and determine the date the Pen should be thrown out. Record the dates in the space provided below.
Example:
Pen 1 - First used on _______ + Number of days you should = Throw out on ______ Date use KwikPen (from Patient Date Information Leaflet) Pen 1 - First used on _______ Throw out on _______ Date Date Pen 2 - First used on _______ Throw out on _______ Date Date Pen 3 - First used on _______ Throw out on _______ Date Date Pen 4 - First used on _______ Throw out on _______ Date Date Pen 5 - First used on _______ Throw out on _______ Date Date If you have any questions or problems with your Humalog KwikPen, contact Lilly at 1-800-Lilly-Rx (1-800-545-5979) or your healthcare professional for assistance.
For more information on Humalog KwikPen and insulin, please visit our website at www.humalog.com
Humalog® and Humalog® KwikPen™ are trademarks of Eli Lilly and Company.
Marketed by: Lilly USA, LLC
Indianapolis, IN 46285, USACopyright © 2007, 2011, Eli Lilly and Company. All rights reserved.
Humalog KwikPen meets the current dose accuracy and functional requirements of ISO 11608-1:2000. Getting Ready Make sure you have the following items: - □
- Humalog® KwikPen™
- □
- New Pen Needle
- □
- Alcohol Swab
Pen Parts KwikPen, and Needle* Assembly *sold separately Literature revised October 28, 2011
PV 5592 AMP
-
PRINCIPAL DISPLAY PANEL
PACKAGE LABELING
PACKAGE CARTON – HUMALOG Vial 10 mL 1ct
NDC 54868-5108-0
10 mL
VL-7510
100 units per mL
Humalog®
insulin lispro injection, USP
(rDNA origin)
For subcutaneous use.
Rx only
U-100
PACKAGE LABELING
PACKAGE CARTON – HUMALOG Prefilled Pen 5 x 3mL
NDC 54868-5899-0
15 mL
VL-8725
100 units per mL
Humalog®
insulin lispro injection, USP
(rDNA origin)
For subcutaneous use.
Rx only
U-100
PACKAGE LABELING
PACKAGE CARTON – HUMALOG Cartridge 5 x 3 mL
NDC 54868-5836-0
15 mL
VL-7516
100 units per mL
Humalog®
insulin lispro injection, USP
(rDNA origin)
For subcutaneous use.
Rx only
U-100
-
INGREDIENTS AND APPEARANCE
HUMALOG
insulin lispro injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-5108(NDC:0002-7510) Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Insulin lispro (UNII: GFX7QIS1II) (Insulin lispro - UNII:GFX7QIS1II) Insulin lispro 100 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength Glycerin (UNII: PDC6A3C0OX) 16 mg in 1 mL Sodium Phosphate, Dibasic (UNII: GR686LBA74) 1.88 mg in 1 mL Metacresol (UNII: GGO4Y809LO) 3.15 mg in 1 mL Zinc (UNII: J41CSQ7QDS) .0197 mg in 1 mL Phenol (UNII: 339NCG44TV) Water (UNII: 059QF0KO0R) Hydrochloric acid (UNII: QTT17582CB) Sodium hydroxide (UNII: 55X04QC32I) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-5108-0 1 in 1 CARTON 1 10 mL in 1 VIAL Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA020563 05/02/2005 HUMALOG PEN
insulin lispro injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-5899(NDC:0002-8725) Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Insulin lispro (UNII: GFX7QIS1II) (Insulin lispro - UNII:GFX7QIS1II) Insulin lispro 100 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength Glycerin (UNII: PDC6A3C0OX) 16 mg in 1 mL Sodium Phosphate, Dibasic (UNII: GR686LBA74) 1.88 mg in 1 mL Metacresol (UNII: GGO4Y809LO) 3.15 mg in 1 mL Zinc (UNII: J41CSQ7QDS) .0197 mg in 1 mL Phenol (UNII: 339NCG44TV) Water (UNII: 059QF0KO0R) Hydrochloric acid (UNII: QTT17582CB) Sodium hydroxide (UNII: 55X04QC32I) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-5899-0 5 in 1 CARTON 1 3 mL in 1 SYRINGE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA020563 05/12/2008 HUMALOG CARTRIDGE
insulin lispro injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-5836(NDC:0002-7516) Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Insulin lispro (UNII: GFX7QIS1II) (Insulin lispro - UNII:GFX7QIS1II) Insulin lispro 100 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength Glycerin (UNII: PDC6A3C0OX) 16 mg in 1 mL Sodium Phosphate, Dibasic (UNII: GR686LBA74) 1.88 mg in 1 mL Metacresol (UNII: GGO4Y809LO) 3.15 mg in 1 mL Zinc (UNII: J41CSQ7QDS) .0197 mg in 1 mL Phenol (UNII: 339NCG44TV) Water (UNII: 059QF0KO0R) Hydrochloric acid (UNII: QTT17582CB) Sodium hydroxide (UNII: 55X04QC32I) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-5836-0 5 in 1 CARTON 1 3 mL in 1 CARTRIDGE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA020563 12/03/2007 Labeler - Physicians Total Care, Inc. (194123980) Establishment Name Address ID/FEI Business Operations Physicians Total Care, Inc. 194123980 relabel