Label: CLINOLIPID- olive oil and soybean oil injection, emulsion

-
NDC Code(s):
0338-9540-01,
0338-9540-02,
0338-9540-03,
0338-9540-04, view more0338-9540-05, 0338-9540-06, 0338-9540-07, 0338-9540-08
- Packager: Baxter Healthcare Corporation
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated May 17, 2023
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use CLINOLIPID safely and effectively. See full prescribing information for CLINOLIPID.
CLINOLIPID (lipid injectable emulsion), for intravenous use
Initial U.S. Approval: 1975RECENT MAJOR CHANGES
INDICATIONS AND USAGE
CLINOLIPID is indicated in adults for parenteral nutrition providing a source of calories and essential fatty acids when oral or enteral nutrition is not possible, insufficient, or contraindicated. (1)
Limitations of Use:
- •
- CLINOLIPID is not indicated for use in pediatric patients because there is insufficient data to demonstrate that CLINOLIPID provides sufficient amounts of essential fatty acids in this population. (1, 8.4)
- •
- The omega-3: omega-6 fatty acid ratio in CLINOLIPID has not been shown to improve clinical outcomes compared to other intravenous lipid emulsions. (1)
DOSAGE AND ADMINISTRATION
- •
- Use a 1.2 micron in-line filter when administering to a patient. (2.1)
- •
- For infusion into a central or peripheral vein. (2.2)
- •
- See full prescribing information for administration and admixing instructions. (2.2, 2.3)
- •
- CLINOLIPID Pharmacy Bulk Package is only indicated for use in pharmacy admixture programs for the preparation of three-in-one or total nutrition admixtures. (2.2)
- •
- The recommended dose depends on energy expenditure, clinical status, body weight, tolerance, ability to metabolize and consideration of additional energy given to the patient. The usual daily lipid dosage in adults is 1 to 1.5 g/kg/day and should not exceed 2.5 g/kg/day. (2.4)
DOSAGE FORMS AND STRENGTHS
Injectable emulsion:
- •
- 20% (20 g/100 mL) (0.2 g/mL) of lipid in 100 mL single-dose flexible container (3)
- •
- 20% (50 g/250 mL) (0.2 g/mL) of lipid in 250 mL single-dose flexible container (3)
- •
- 20% (100 g/500 mL) (0.2 g/mL) of lipid in 500 mL single-dose flexible container (3)
- •
- 20% (200 g/1,000 mL) (0.2 g/mL) of lipid in 1,000 mL Pharmacy Bulk Package (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- •
- Clinical Decompensation with Rapid Infusion of Intravenous Lipid Emulsion in Neonates and Infants: Acute respiratory distress, metabolic acidosis, and death after rapid infusion of intravenous lipid emulsions have been reported. (5.1, 8.4)
- •
- Parenteral Nutrition-Associated Liver Disease: Increased risk in patients who receive parenteral nutrition for greater than 2 weeks, especially preterm neonates. Monitor liver tests; if abnormalities occur, consider discontinuation or dosage reduction. (5.2, 8.4)
- •
- Hypersensitivity Reactions: Monitor for signs or symptoms. Discontinue infusion if reactions occur. (5.3)
- •
- Risk of Infections, Fat Overload Syndrome, Refeeding Syndrome, Hypertriglyceridemia, and Essential Fatty Acid Deficiency: Monitor for signs and symptoms; monitor laboratory parameters. (5.4, 5.5, 5.6, 5.7, 5.9)
- •
- Aluminum Toxicity: Increased risk in patients with renal impairment, including preterm neonates. (5.8, 8.4)
ADVERSE REACTIONS
The most common (5%) adverse drug reactions from clinical trials were nausea and vomiting, hyperlipidemia, hyperglycemia, hypoproteinemia and abnormal liver function tests. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Baxter Healthcare at 1-866-888-2472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
The anticoagulant activity of coumarin derivatives, including warfarin, may be counteracted. (7)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Use of an Inline Filter When Administering CLINOLIPID to a Patient
2.2 Important Administration Instructions
2.3 Admixing Guidelines
2.4 Dosing Considerations
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Clinical Decompensation with Rapid Infusion of Intravenous Lipid Emulsion in Neonates and Infants
5.2 Parenteral Nutrition-Associated Liver Disease and Other Hepatobiliary Disorders
5.3 Hypersensitivity Reactions
5.4 Infections
5.5 Fat Overload Syndrome
5.6 Refeeding Syndrome
5.7 Hypertriglyceridemia
5.8 Aluminum Toxicity
5.9 Monitoring/Laboratory Tests
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
CLINOLIPID is indicated in adults for providing a source of calories and essential fatty acids for parenteral nutrition when oral or enteral nutrition is not possible, insufficient, or contraindicated.
Limitations of Use
CLINOLIPID is not indicated for use in pediatric patients because there is insufficient data to demonstrate that CLINOLIPID provides sufficient amounts of essential fatty acids in this population. [See Use in Specific Populations (8.4)]
The omega-3: omega-6 fatty acid ratio in CLINOLIPID has not been shown to improve clinical outcomes compared to other intravenous lipid emulsions. [See Clinical Studies (14)]
-
2 DOSAGE AND ADMINISTRATION
2.1 Use of an Inline Filter When Administering CLINOLIPID to a Patient
Fragments of the administration port membrane could be dislodged into the bag after spiking. Use a 1.2 micron in-line filter during administration of CLINOLIPID (alone or as part of an admixture) to remove particulate matter or micro-precipitate contamination during administration of a lipid injection (alone or as part of an admixture). Particulate matter greater than 5 microns has the capability of obstructing blood flow through capillaries, which could lead to embolism and vascular occlusion. Do not use filters of less than 1.2 micron pore size with lipid emulsions.
2.2 Important Administration Instructions
Before opening the overwrap, check the color of the oxygen indicator. Compare color of the indicator to the reference color printed next to the OK symbol depicted in the printed area of the indicator label. Do not use the product if the color of the oxygen absorber/indicator does not correspond to the reference color printed next to the OK symbol.
After opening the bag, use the contents immediately and discard unused portion.
Visually inspect that the emulsion is a homogeneous liquid with a milky appearance. Inspect for particulate matter and discoloration prior to administration, whenever solution and container permit.
Do not exceed the recommended maximum infusion rate in Table 1 [see Dosage and Administration (2.4) and Warnings and Precautions (5.1)].
When Administering CLINOLIPID to a Patient:
Do not connect flexible bags in series to avoid air embolism due to possible residual gas contained in the primary bag.
Air embolism can result if residual gas in the bag is not fully evacuated prior to administration if the flexible bag is pressurized to increase flow rates.
Do not use vented administration sets with the vent in the open position. This can result in air embolism.
If CLINOLIPID is mixed with dextrose and/or amino acid solutions, check the compatibility before administration by inspecting the mixture closely for the presence of precipitates. Formation of precipitates could result in vascular occlusion.
CLINOLIPID can be administered via central or peripheral vein. When administered with dextrose and amino acids, the choice of a central or peripheral venous route should depending on the osmolarity of the final infusate.
Do not use administration sets and lines that contain di-2-ethylhexyl phthalate (DEHP).
Use only a 1.2 micron pore size in-line filter to administer CLINOLIPID. DO NOT use any size less than 1.2 micron pore size in-line filter [see Dosage and Administration (2.1)].
CLINOLIPID 100 mL, 250 mL and 500 mL single-dose Flexible Containers:
- •
- After removing the overpouch, infuse immediately. If not used immediately, the product should be stored for no longer than 24 hours at no more than 25°C (77°F).
CLINOLIPID 1,000 mL Pharmacy Bulk Package:
- •
- For admixing use only and not for direct intravenous infusion. Prior to administration, transfer to a separate PN container for individual patient use.
- •
- Transfer the contents through the infusion port using a suitable sterile transfer device or dispensing set. Discard any unused contents. Discard any unused portion.
- •
- Use the Pharmacy Bulk Package immediately for admixing after removal from overpouch. If not used immediately, the product should be stored for no longer than 24 hours at no more than 25°C (77°F).
- •
- Once the closure is penetrated use Pharmacy Bulk Package contents within 4 hours.
2.3 Admixing Guidelines
When Admixing CLINOLIPID in the Pharmacy:
Prepare the admixture using strict aseptic techniques to avoid microbial contamination.
Do not add additives directly to CLINOLIPID. Do not add CLINOLIPID to the total parenteral nutrition container first; destabilization of the lipid may occur from such an admixture.
Do not use the EXACTAMIX Inlet REF 173 (H938173) with an EXACTAMIX compounder to transfer CLINOLIPID. This inlet spike has been associated with dislodgement of the administration port membrane into the CLINOLIPID bag. Use of EXACTAMIX Inlet REF 174 (H938174) is recommended.
The following proper mixing sequence must be followed to minimize pH related problems by ensuring that typically acidic Dextrose Injections are not mixed with lipid emulsions alone:
- 1.
- Transfer Dextrose Injection to the Total Parenteral Nutrition Admixture Container
- 2.
- Transfer Amino Acid Injection
- 3.
- Transfer Lipid Emulsion
Amino Acid Injection, Dextrose Injection and Lipid Emulsions may be simultaneously transferred to the admixture container. Use gentle agitation during admixing to minimize localized concentration effects; shake bags gently after each addition.
The prime destabilizers of emulsions are excessive acidity (such as a pH below 5) and inappropriate electrolyte content. Give careful consideration to additions of divalent cations (Ca++ and Mg++), which have been shown to cause emulsion instability. Amino acid solutions exert buffering effects that protect the emulsion.
Inspect the admixture closely for separation of the emulsion. This can be visibly identified by a yellowish streaking or the accumulation of yellowish droplets in the admixed emulsion. The admixture should also be examined for particulates. Discard the admixture if any of the above is observed.
Protect the admixed parenteral nutrition solution from light.
2.4 Dosing Considerations
The recommended nutritional requirements of lipid and recommended dosages of CLINOLIPID to be administered to meet those requirements for adult patients are provided in Table 1, along with recommendations for the initial and maximum infusion rates. For complete parenteral nutrition, concomitant supplementation with amino acids, carbohydrates, electrolytes, vitamins, and trace elements is necessary.
Prior to administration of CLINOLIPID, correct severe water and electrolyte disorders, severe fluid overload states, and severe metabolic disorders. Before starting the infusion, obtain serum triglyceride levels to establish the baseline value. In patients with elevated triglyceride levels, initiate CLINOLIPID injection at a lower dose, and advance in smaller increments, checking the triglyceride levels prior to each adjustment.
Adjust the administration flow rate by taking into account the dose being administered, the daily volume intake, and the duration of the infusion [see Overdosage (10)].
The recommended duration of infusion for a parenteral nutrition bag is between 12 and 24 hours, depending on the clinical situation. Treatment with parenteral nutrition may be continued for as long as is required by the patient’s condition.
The maximum daily dose of CLINOLIPID should be based on individual total nutritional requirements and patient tolerance (Table 1).
Table 1: Recommended Adult Dosage and Infusion Rate - *
- Clinolipid 20% Pharmacy Bulk Package is not intended for direct intravenous administration.
- †
- Daily dosage should also not exceed a maximum of 60% of total energy requirements [see Overdosage (10)].
Nutritional Requirements
Direct Infusion Rate*
Recommended Initial Dosage and Maximum Dosage
Initial
Maximum
1 to 1.5 g/kg/day not to exceed 2.5 g/kg/day†
0.5 mL/min for the first 15 to 30 minutes;
if tolerated, gradually increase to the required rate after 30 minutes0.5 mL/kg/hour
-
3 DOSAGE FORMS AND STRENGTHS
CLINOLIPID is a sterile, homogenous, white, milky, lipid injectable emulsion supplied as:
- •
- 20% (20 g/100 mL)(0.2g/mL) of lipid in 100 mL single-dose Flexible Container
- •
- 20% (50 g/250 mL)(0.2g/mL) of lipid in 250 mL single-dose Flexible Container
- •
- 20% (100 g/500 mL)(0.2g/mL) of lipid in 500 mL single-dose Flexible Container
- •
- 20% (200 g/1,000 mL)(0.2g/mL) of lipid in 1,000 mL Pharmacy Bulk Package
-
4 CONTRAINDICATIONS
The use of CLINOLIPID is contraindicated in patients with the following:
- •
- Known hypersensitivity to egg, soybean, peanut or to any of the active or inactive ingredients in CLINOLIPID [see Warnings and Precautions (5.3)].
- •
- Severe disorders of lipid metabolism characterized by hypertriglyceridemia (serum triglyceride >1,000 mg/dL) [see Warnings and Precautions (5.7)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Clinical Decompensation with Rapid Infusion of Intravenous Lipid Emulsion in Neonates and Infants
In the postmarketing setting, serious adverse reactions including acute respiratory distress, metabolic acidosis, and death have been reported in neonates and infants after rapid infusion of intravenous lipid emulsions. Hypertriglyceridemia was commonly reported.
Preterm and small for gestational age infants have poor clearance of intravenous lipid emulsion and increased free fatty acid plasma levels following lipid emulsion infusion.
5.2 Parenteral Nutrition-Associated Liver Disease and Other Hepatobiliary Disorders
Risk of Parenteral Nutrition-Associated Liver Disease
Parenteral nutrition-associated liver disease (PNALD), also referred to as intestinal failure-associated liver disease (IFALD), can present as cholestasis or hepatic steatosis, and may progress to steatohepatitis with fibrosis and cirrhosis (possibly leading to chronic hepatic failure). The etiology of PNALD is multifactorial; however, intravenously administered phytosterols (plant sterols) contained in plant-derived lipid emulsions, including CLINOLIPID, have been associated with development of PNALD.
Monitor liver tests in patients treated with CLINOLIPID and consider discontinuation or dosage reduction if abnormalities occur.
Other Hepatobiliary Disorders
Hepatobiliary disorders including cholecystitis and cholelithiasis have developed in some PN-treated patients without preexisting liver disease.
Monitor liver tests when administering CLINOLIPID. Patients developing signs of hepatobiliary disorders should be assessed early to determine whether these conditions are related to CLINOLIPID use.
5.3 Hypersensitivity Reactions
CLINOLIPID contains soybean oil and egg phospholipids, which may cause hypersensitivity reactions. Cross reactions have been observed between soybean and peanut. CLINOLIPID is contraindicated in patients with known hypersensitivity to egg, soybean, peanut or any of the active or inactive ingredients in CLINOLIPID. If a hypersensitivity reaction occurs, stop infusion of CLINOLIPID immediately and initiate appropriate treatment and supportive measures.
5.4 Infections
Lipid emulsions, such as CLINOLIPID, can support microbial growth and are an independent risk factor for the development of catheter-related bloodstream infections. To decrease the risk of infectious complications, ensure aseptic techniques are used for catheter placement, catheter maintenance, and preparation and administration of CLINOLIPID.
Monitor for signs and symptoms of infection including fever and chills, as well as laboratory test results that might indicate infection (including leukocytosis and hyperglycemia). Perform frequent checks of the intravenous catheter insertion site for edema, redness, and discharge.
5.5 Fat Overload Syndrome
Fat overload syndrome is a rare condition that has been reported with intravenous lipid formulations and is characterized by a sudden deterioration in the patient's condition (e.g., fever, anemia, leukopenia, thrombocytopenia, coagulation disorders, hyperlipidemia, hepatomegaly, deteriorating liver function, and central nervous system manifestations such as coma). A reduced or limited ability to metabolize lipids, accompanied by prolonged plasma clearance (resulting in higher lipid levels), may result in this syndrome. Although fat overload syndrome has been most frequently observed when the recommended lipid dose or infusion rate was exceeded, cases have also been described when the lipid formulation was administered according to instructions.
If signs or symptoms of fat overload syndrome occur, stop CLINOLIPID. The syndrome is usually reversible when the infusion of the lipid emulsion is stopped.
5.6 Refeeding Syndrome
Administering PN to severely undernourished patients may result in the refeeding syndrome, which is characterized by intracellular shift of potassium, phosphorus, and magnesium as the patients become anabolic. Thiamine deficiency and fluid retention may also develop. To prevent these complications, closely monitor severely malnourished patients and slowly increase their nutrient intake.
5.7 Hypertriglyceridemia
The use of CLINOLIPID is contraindicated in patients with hypertriglyceridemia with serum triglyceride concentrations >1,000 mg/dL.
Patients with conditions such as inherited lipid disorders, obesity, diabetes mellitus, or metabolic syndromes have a higher risk of developing hypertriglyceridemia with the use of CLINOLIPID. In addition, patients with hypertriglyceridemia may have worsening of their hypertriglyceridemia with administration of CLINOLIPID. Excessive dextrose administration may further increase such risk.
Evaluate patients’ capacity to metabolize and eliminate the infused lipid emulsion by measuring serum triglycerides before the start of infusion (baseline value) and regularly throughout treatment. If triglyceride levels are above 400 mg/dL in adults, stop the CLINOLIPID infusion and monitor serum triglyceride levels to avoid clinical consequences of hypertriglyceridemia such as pancreatitis.
To minimize the risk of new or worsening of hypertriglyceridemia, assess high-risk patients for their overall energy intake including other sources of lipids and dextrose, as well as concomitant drugs that may affect lipid and dextrose metabolism.
5.8 Aluminum Toxicity
CLINOLIPID contains no more than 25 mcg/L of aluminum.
The aluminum contained in CLINOLIPID may reach toxic levels with prolonged administration in patients with impaired kidney function. Preterm infants are at greater risk because their kidneys are immature, and they require large amounts of calcium and phosphate solutions that contain aluminum.
Patients with impaired kidney function, including preterm infants, who receive parenteral levels of aluminum at greater than 4 to 5 mcg/kg/day, accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration of total parenteral nutrition products.
5.9 Monitoring/Laboratory Tests
Routine Monitoring
Monitor fluid status closely in patients with pulmonary edema or heart failure.
Throughout treatment, monitor serum triglycerides [see Warnings and Precautions (5.7)], fluid and electrolyte status, serum osmolarity, blood glucose, liver and kidney function, blood count (including platelets), and coagulation parameters.
The lipids contained in CLINOLIPID 20% may interfere with the results of some laboratory tests (e.g., hemoglobin, lactate dehydrogenase, bilirubin, oxygen saturation) if the blood is sampled before the lipids have cleared from the bloodstream. Conduct these tests at least 6 hours after stopping the infusion.
CLINOLIPID 20% contains Vitamin K that may counteract anticoagulant activity [see Drug Interactions (7)].
Essential Fatty Acids
Monitoring patients for signs and symptoms of essential fatty acid deficiency (EFAD) is recommended. Laboratory tests are available to determine serum fatty acids levels. Reference values should be consulted to help determine adequacy of essential fatty acid status. Increasing essential fatty acid intake (enterally or parenterally) is effective in treating and preventing EFAD.
In CLINOLIPID injection, the mean composition of linoleic acid (an omega-6 essential fatty acid) is 35.8 mg/mL (range 27.6 to 44.0 mg/mL) and α-linolenic acid (an omega-3 essential fatty acid) is 4.7 mg/mL (range 1.0 to 8.4 mg/mL). There are insufficient long-term data to determine whether CLINOLIPID 20% can supply essential fatty acids in adequate amounts in patients who may have increased requirements.
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- •
- Clinical Decompensation with Rapid Infusion of Intravenous Lipid Emulsion in Neonates and Infants [see Warnings and Precautions (5.1)]
- •
- Parenteral Nutrition-Associated Liver Disease and Other Hepatobiliary Disorders [see Warnings and Precautions (5.2)]
- •
- Hypersensitivity reactions [see Warnings and Precautions (5.3)]
- •
- Risk of infections [see Warnings and Precautions (5.4)]
- •
- Fat overload syndrome [see Warnings and Precautions (5.5)]
- •
- Refeeding syndrome [see Warnings and Precautions (5.6)]
- •
- Hypertriglyceridemia [see Warnings and Precautions (5.7)]
- •
- Aluminum toxicity [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The CLINOLIPID trials had small sample sizes and patients had a variety of underlying medical conditions both between different trials and within the individual trials. Patients had gastrointestinal diseases/dysfunction or were recovering from gastrointestinal or other surgeries, trauma, burns, or were afflicted by other chronic illness. The largest trial (Study 1, 48 subjects) enrolled patients with many different underlying diagnoses. The rates of treatment emergent adverse reactions can therefore not be directly compared to rates observed in the clinical trials of other related products and may not reflect the rates observed in clinical practice.
Commonly observed adverse reactions in 261 adult patients who received CLINOLIPID were nausea and vomiting, hyperlipidemia, hyperglycemia, hypoproteinemia and abnormal liver function tests and occurred in 2 to 10 % of patients. In Study 1 the most common adverse reactions were infectious complications (urinary tract infection, septicemia, and fever of unknown origin), treatment emergent abnormalities on liver/gallbladder ultrasound and abnormalities of serum chemistries, principally, hepatic function tests. Adverse reactions in Study 2 were similar.
Adverse reactions reported with other intravenous lipid emulsions include hyperlipidemia, hypercoagulability, thrombophlebitis, and thrombocytopenia.
Adverse reactions reported in long-term use with other intravenous lipid emulsions include hepatomegaly, jaundice due to central lobular cholestasis, splenomegaly, thrombocytopenia, leukopenia, abnormalities in liver function tests, brown pigmentation of the liver and overloading syndrome (focal seizures, fever, leukocytosis, hepatomegaly, splenomegaly and shock).
6.2 Postmarketing Experience
The following adverse reactions have been identified during use of CLINOLIPID. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Gastrointestinal Disorders: Diarrhea
Skin and Subcutaneous Tissue Disorders: Pruritus
Immune System Disorders: Hypersensitivity with the manifestations of rash and dyspnea
Investigations: International normalized ratio (INR) decreased in anticoagulated patients [see Drug Interactions (7)]
- 7 DRUG INTERACTIONS
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The limited available data on the use of CLINOLIPID in pregnant women are not sufficient to inform a drug-associated risk. However, there are clinical considerations if CLINOLIPID is used in pregnant women [see Clinical Considerations]. Animal reproduction studies have not been conducted with lipid injectable emulsion.
The estimated background risk of major birth defects and miscarriage for the indicated population are unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and15 to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo-Fetal Risk:
Severe malnutrition in a pregnant woman is associated with preterm delivery, low birth weight, intrauterine growth restriction, congenital malformations and perinatal mortality. Parenteral nutrition should be considered if a pregnant woman’s nutritional requirements cannot be fulfilled by oral or enteral intake. It is not known whether the administration of CLINOLIPID to pregnant women provides adequate essential fatty acids to the developing fetus.8.2 Lactation
Risk Summary
There are no data available to assess the presence of CLINOLIPID and/or its active metabolite(s) in human milk, the effects on the breastfed child or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for CLINOLIPID and any potential adverse effects on the breastfed child from CLINOLIPID or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of CLINOLIPID have not been established in pediatric patients. CLINOLIPID is not indicated for use in pediatric patients. Pediatric studies did not establish that CLINOLIPID provides sufficient amounts of essential fatty acids (EFA) in pediatric patients. Pediatric patients may be particularly vulnerable to neurologic complications due to EFA deficiency if adequate amounts of EFA are not provided.
In the postmarketing setting, clinical decompensation with rapid infusion of intravenous lipid emulsion in neonates and infants, sometimes fatal has been reported [see Warnings and Precautions (5.1)]. Patients, particularly preterm infants, are at risk for aluminum toxicity [see Warnings and Precautions (5.8)]. Patients, including pediatric patients, may be at risk for PNALD [see Warnings and Precautions (5.2)]. In clinical trials of a pure soybean oil based intravenous lipid emulsion product, thrombocytopenia in neonates occurred (less than 1%).
8.5 Geriatric Use
Of the total number of subjects in clinical studies of CLINOLIPID, 21% were 65 and over, while 10% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
-
10 OVERDOSAGE
In the event of overdose, serious adverse reactions may result [see Warnings and Precautions (5.1, 5.5)]. Stop the infusion to allow lipids to clear from serum. The effects are usually reversible after the lipid infusion is stopped. If medically appropriate, further intervention may be indicated. The lipid administered and fatty acids produced are not dialyzable.
-
11 DESCRIPTION
CLINOLIPID lipid injectable emulsion, USP is a sterile, non-pyrogenic, homogenous, white, milky lipid emulsion for intravenous infusion. The lipid content of CLINOLIPID is 0.2 g/mL and comprises a mixture of refined olive oil and refined soybean oil in an approximate ratio of 4:1 (olive:soy). The mean concentration of linoleic acid (an omega-6 essential fatty acid) is 35.8 mg/mL (range 27.6 to 44.0 mg/mL) and α-linolenic acid (an omega-3 essential fatty acid) is 4.7 mg/mL (range 1.0 to 8.4 mg/mL). The phospholipids provide 470 milligrams or 15 mmol of phosphorus per liter.
The total energy content, including fat, phospholipids and glycerin is 2000 kcal/L.
Each 100 mL of CLINOLIPID 20% contains approximately 16 g of Olive Oil NF and 4 g of Soybean Oil USP, 1.2 g Egg Phospholipids NF, 2.25 g Glycerin USP, 0.03 g Sodium Oleate, and Water for Injection USP. Sodium Hydroxide NF for pH adjustment, pH: 6.0 to 9.0.
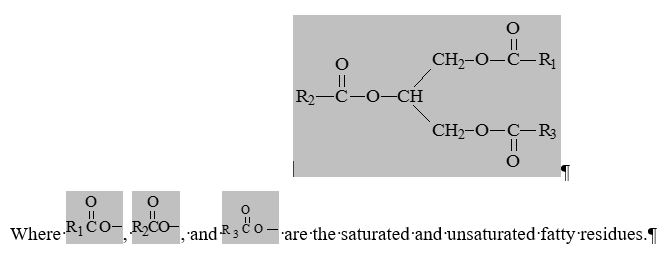
The olive and soybean oils are refined natural products consisting of a mixture of neutral triglycerides of predominantly unsaturated fatty acids with the following structure:
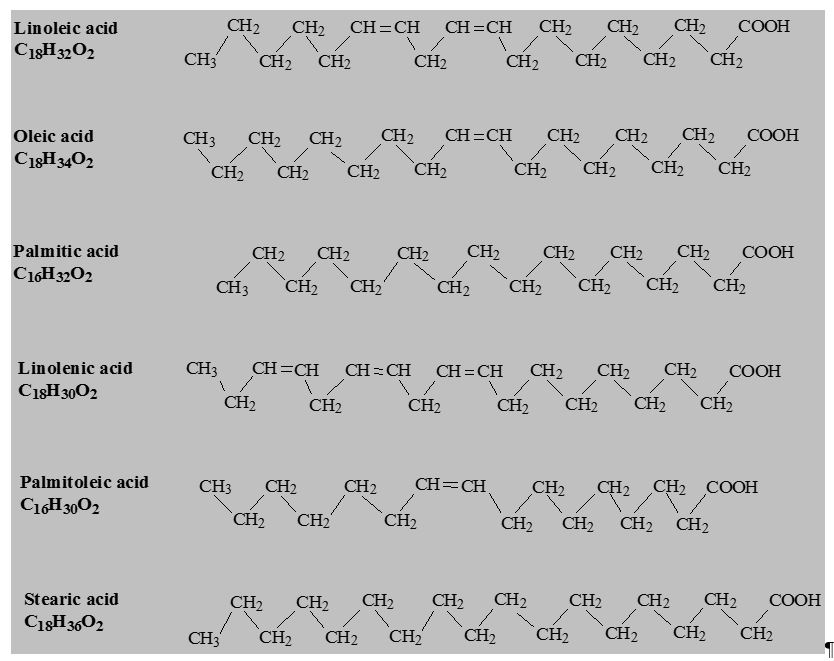
The major component fatty acids are linoleic (13.8 to 22.0%), oleic (44.3 to 79.5%), palmitic (7.6 to 19.3%), linolenic (0.5 to 4.2%), palmitoleic (0.0 to 3.2%) and stearic (0.7 to 5.0%). These fatty acids have the following chemical and structural formulas:
CLINOLIPID has an osmolality of approximately 340 mOsmol/kg water (which represents an osmolarity of 260 mOsmol/liter of emulsion).
CLINOLIPID contains no more than 25 mcg/L of aluminum.
-
12 CLINICAL PHARMACOLOGY
CLINOLIPID administered intravenously provides biologically utilizable source of calories and essential fatty acids.
12.1 Mechanism of Action
Fatty acids serve as an important substrate for energy production. The most common mechanism of action for energy production derived from fatty acid metabolism is beta oxidation. Fatty acids are important for membrane structure and function, precursors for bioactive molecules (such as prostaglandins), and as regulators of gene expression.
12.2 Pharmacodynamics
Infused essential fatty acids are synthesized into higher derivative fatty acids. Olive oil contains significant amounts of alpha-tocopherol that contributes to Vitamin E status.
12.3 Pharmacokinetics
Metabolism and Excretion
The fatty acids, phospholipids, and glycerol found in lipid emulsions are metabolized by cells to carbon dioxide and water. The metabolism of these substances results in the generation of energy in the form of adenosine triphosphate (ATP). Some fatty acids are stored in the body in fat tissue, cell membranes, or as intracellular triglycerides. There is constant turn-over of these tissues, with the result that the lipid components are eventually metabolized to carbon dioxide and water. Carbon dioxide is expired through the lungs. Water is excreted through the kidneys or lost through evaporation/expiration through the skin, lungs, and other tissue surfaces. Some lipids (i.e., phospholipids, cholesterol, and bile acids) are excreted through the biliary system.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies with CLINOLIPID have not been performed to evaluate the carcinogenic potential, mutagenic potential, or effects on fertility.
13.2 Animal Toxicology and/or Pharmacology
CLINOLIPID was evaluated in toxicity studies conducted in rats and dogs for up to 3 months. The principle signs of toxicity noted in the 3-month studies were:
- •
- Slight hemolytic anemia at 12 g/kg/day in rats and at 6 g/kg/day in dogs. These doses in rats and dogs are 4.8 and 2.4 times higher, respectively, than the recommended adult dose (2.5 g/kg/day) of CLINOLIPID.
- •
- Dose-dependent decrease in urea levels in rats at 6 and 12 g/kg/day dose levels and in dogs at 3, 4.5 and 6 g/kg/day dose levels associated with decreased feed consumption.
- •
- Hypercholesterolemia in dogs at 3, 4.5 and 6 g/kg/day dose levels.
- •
- Hepatic pathology of lipid and pigmentary overload in male and female rats at 3, 6 and 12 g/kg/day dose levels and brownish-yellow pigmentation in vacuolated Kupffer cells in male and female dogs at 3, 4.5 and 6 g/kg/day dose levels with hepatocyte vacuolation in male dogs at 6 g/kg/day and female dogs at 4.5 and 6 g/kg/day dose levels.
- •
- Splenic pigmentation and vacuolization in rats at 3, 6 and 12 g/kg/day dose levels, and dogs in 4.5 and 6 g/kg/day dose levels.
At doses of 3 g/kg/day, slight lipid and pigmentary overload of the liver and vacuolization of Kupffer cells were observed in rats and dogs. At a dose of 12 g/kg/day in rats, hepatocellular vacuolation, granulomatous inflammation of the liver, hepatocellular necrosis and hemosiderosis of the liver and lipid deposits and splenic hemosiderosis, were observed. In dogs, at a dose of 6 g/kg/day, brownish-yellow pigmentation in the Kupffer cells of liver and spleen, hyperplasia of vacuolated Kupffer cells, hepatocyte vacuolization, a slight increase in the number of lipid storage cells (Ito cells) in the liver and macrophage vacuolization of the spleen were observed.
-
14 CLINICAL STUDIES
Two clinical trials (Study 1 and Study 2) in adults compared CLINOLIPID to a pure soybean oil based intravenous lipid emulsion. Although Study 1 and Study 2 were not adequately designed to demonstrate noninferiority of CLINOLIPID to the soybean oil comparator, they support CLINOLIPID injection as a source of calories and essential fatty acids in adults. The lipid dosage was variable in Studies 1 and 2 and adjusted to the patient’s nutritional requirements.
Study 1 was a randomized, open-label, multicenter study. Forty eight (48) patients, aged 17 to 75 years, requiring ≥15 days (mean 22 days) exclusive parenteral nutrition (TPN) were enrolled and randomized to either CLINOLIPID or a pure soybean oil based intravenous lipid emulsion. Nutritional efficacy was assessed by anthropometric indices (body weight, arm circumference, skin-fold thickness), biomarkers of protein metabolism (total protein, albumin) and lipid metabolism. Anthropometric criteria (body weight, arm circumference, and skin fold thickness) were comparable for both groups. Mean total serum protein and albumin increased similarly in both groups.
Study 2 was a randomized, open label multicenter study that enrolled 22 patients aged 32-81 years who required long-term parenteral nutrition. Twelve patients received CLINOLIPID for a mean of 202 days (range 24 to 408 days) and 10 patients received the comparator lipid for a mean of 145 days (range 29-394 days). The two groups had similar outcomes for weight, weight loss, mid-arm circumference and triceps skinfold thickness.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
CLINOLIPID is a sterile, white, homogenous lipid injectable emulsion supplied in CLARITY polyolefin Flexible Containers as follows:
- Strengths
- Container
Size
- Product Code
- NDC Number
(1 Bag)
- NDC Number (Shelf Pack)
- 20% (20 g/100 mL) (0.2 g/mL)
- 100 mL
- EADB9520
- 0338-9540-01 (single-dose Flexible Container)
- 0338-9540-05
(15 pack)
- 20% (50 g/250 mL) (0.2 g/mL)
- 250 mL
- EADB9521
- 0338-9540-02 (single-dose Flexible Container)
- 0338-9540-06 (10 pack)
- 20% (100 g/500 mL) (0.2 g/mL)
- 500 mL
- EADB9523
- 0338-9540-03 (single-dose Flexible Container)
- 0338-9540-07 (12 pack)
- 20% (200 g/1,000 mL) (0.2 g/mL)
- 1,000 mL
- EADB9524
- 0338-9540-04 (Pharmacy Bulk Package bag)
- 0338-9540-08 (6 pack)
The CLARITY Container is a lipid-compatible plastic container (PL 2401-1). The bag is packaged in an oxygen barrier overpouch, which contains an oxygen absorber / oxygen indicator sachet.
CLINOLIPID should be stored at 20°C to 25°C (68°F to 77°F). Excursion permitted between 15°C to 30 °C (59°F to 86°F). See USP Controlled Room Temperature. Protect from freezing. Avoid excessive heat. Store in overpouch until ready to use.
CLINOLIPID 100 mL, 250 mL and 500 mL single-dose Flexible Containers:
After removing the overpouch, infuse immediately. If not used immediately, the product should be stored for no longer than 24 hours at not more than 25°C (77°F) [See Dosage and Administration (2.2)].CLINOLIPID 1,000 mL Pharmacy Bulk Package:
Use the pharmacy bulk package immediately for admixing after removal from overpouch. If not used immediately, the product should be stored for no longer than 24 hours at not more than 25°C (77°F) [see Dosage and Administration (2.2)]. -
17 PATIENT COUNSELING INFORMATION
When initiating CLINOLIPID administration, discuss the following information with the patient or caregiver:
Parenteral Nutrition-Associated Liver Disease and Other Hepatobiliary Disorders
Inform patients and caregivers that use of parenteral nutrition may result in parenteral nutrition-associated liver disease and/or other hepatobiliary disorders [see Warnings and Precautions (5.2)].
Hypersensitivity Reactions
Inform patients and caregivers that CLINOLIPID may cause hypersensitivity reactions. If CLINOLIPID is infused at home, instruct patients or caregivers to stop the infusion of CLINOLIPID immediately and seek medical attention if a hypersensitivity reaction occurs [see Warnings and Precautions (5.3)].
Infections
Inform patients and caregivers that patients who receive CLINOLIPID are at risk of infection. If CLINOLIPID is infused at home, instruct patients or caregivers to ensure aseptic techniques are used for the preparation and administration of CLINOLIPID and to monitor for signs and symptoms of infection [see Warnings and Precautions (5.4)].
Fat Overload Syndrome
Inform patients and caregivers that fat overload syndrome has been reported with the use of intravenous lipid emulsions. If CLINOLIPID is infused at home, instruct patients or caregivers to stop CLINOLIPID if signs or symptoms of fat overload syndrome occur [see Warnings and Precautions (5.5)].
Refeeding Syndrome
If the patient is severely malnourished, inform patients and caregivers that administering parenteral nutrition including CLINOLIPID may result in refeeding syndrome [see Warnings and Precautions (5.6)].
Hypertriglyceridemia
Inform patients and caregivers about the risks of hypertriglyceridemia with CLINOLIPID use [see Warnings and Precautions (5.7)].
Aluminum Toxicity
Inform patients and caregivers that prolonged PN administration in patients with renal impairment, including preterm neonates, may result in aluminum reaching toxic levels associated with central nervous system and bone toxicity [see Warnings and Precautions (5.8)].
Preparation and Administration Instructions
If it is acceptable for a patient or caregiver to administer CLINOLIPID at home, then provide recommendations on how to prepare, add compatible additives (when appropriate), administer, and store CLINOLIPID [see Dosage and Administration (2.1, 2.2)].
- SPL UNCLASSIFIED SECTION
-
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
1000 mL
EADB9524 NDC 0338-9540-04
Baxter Logo
Clinolipid
(Lipid Injectable Emulsion, USP) 20%
200 g/1000 mL (0.2 g/mL)Intravenous use only
1000 mL sterile single dose container
Energy Content 2000 kcal/LEach 100 mL contains approximately 16 g of Olive Oil NF
and 4 g of Soybean Oil USP, 1.2 g Egg Phospholipids NF,
2.25 g Glycerin USP, 0.03 g Sodium Oleate, Water for
Injection USP and Sodium Hydroxide NF for pH
adjustment pH 6.0–9.0 Osmolarity 260 mOsmol/L (calc)Cautions Use only if the color of the oxygen indicator is
within allowable range Do not use unless emulsion has
homogeneous milky appearanceDo not add supplemental medications Must not be used
in series connectionsUsual Dosage See package insert
Store at 20 to 25 °C (68 to 77 °F)
Excursion permitted between 15 to 30 °C
(59 to 86 °F)
See USP Controlled Room Temperature
Protect from freezing
Do not use beyond 24 hours once opened;
discard unused portion after 24 hours
Rx OnlyBaxter Healthcare Corporation
BE-35-02-746
EXP LOT
1000
750
500
250
100
-
INGREDIENTS AND APPEARANCE
CLINOLIPID
olive oil and soybean oil injection, emulsionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0338-9540 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength OLIVE OIL (UNII: 6UYK2W1W1E) (OLIVE OIL - UNII:6UYK2W1W1E) OLIVE OIL 16 g in 100 mL SOYBEAN OIL (UNII: 241ATL177A) (SOYBEAN OIL - UNII:241ATL177A) SOYBEAN OIL 4 g in 100 mL Inactive Ingredients Ingredient Name Strength EGG PHOSPHOLIPIDS (UNII: 1Z74184RGV) 1.20 g in 100 mL GLYCERIN (UNII: PDC6A3C0OX) 2.25 g in 100 mL SODIUM OLEATE (UNII: 399SL044HN) 0.03 g in 100 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0338-9540-08 6 in 1 CARTON 01/01/2016 1 NDC:0338-9540-04 1000 mL in 1 BAG; Type 0: Not a Combination Product 2 NDC:0338-9540-07 12 in 1 CARTON 01/01/2016 2 NDC:0338-9540-03 500 mL in 1 BAG; Type 0: Not a Combination Product 3 NDC:0338-9540-06 10 in 1 CARTON 01/01/2016 3 NDC:0338-9540-02 250 mL in 1 BAG; Type 0: Not a Combination Product 4 NDC:0338-9540-05 15 in 1 CARTON 01/01/2016 4 NDC:0338-9540-01 100 mL in 1 BAG; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA204508 01/01/2016 Labeler - Baxter Healthcare Corporation (005083209) Establishment Name Address ID/FEI Business Operations Baxter SA 370353835 MANUFACTURE(0338-9540) , PACK(0338-9540) , ANALYSIS(0338-9540) , STERILIZE(0338-9540) , LABEL(0338-9540) Establishment Name Address ID/FEI Business Operations Baxter R&D Europe SPRL 400409112 ANALYSIS(0338-9540)