OLANZAPINE- olanzapine tablet, film coated
REMEDYREPACK INC.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONHIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use olanzapine tablets USP safely and effectively. See full prescribing information for olanzapine tablets USP. OLANZAPINE tablets USP for oral use. Initial U.S. Approval: 1996
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
|
| Schizophrenia in adults (2.1) | Oral: Start at 5 to 10 mg once daily;
Target 10 mg/day within several days | Bipolar I Disorder (manic or mixed episodes) in adults (2.2) | Oral: Start at 10 or 15 mg once daily | Bipolar I Disorder (manic or mixed episodes) with lithium or valproate in adults (2.2) | Oral: Start at 10 mg once daily | Depressive Episodes associated with Bipolar I Disorder in adults (2.5) | Oral in combination with fluoxetine: Start at 5 mg or oral olanzapine and 20 mg of fluoxetine once daily |
(3)
(3)
(3)
(3)
(3)
(3)
(3)
- Lower starting dose recommended in debilitated or pharmacodynamically sensitive patients or patients with predisposition to hypotensive reactions, or with potential for slowed metabolism (2.1)
- Olanzapine may be given without regard to meals (2.1)
Olanzapine and Fluoxetine in Combination: (3)
(3)
(3)
- Dosage adjustments, if indicated, should be made with the individual components according to efficacy and tolerability. (2.5)
- Olanzapine monotherapy is not indicated for the treatment of depressive episodes associated with bipolar I disorder. (2.5)
- Safety of coadministration of doses above 18 mg olanzapine with 75 mg fluoxetine has not been evaluated. (2.5)
(3)
(3)
DOSAGE FORMS AND STRENGTHS
DOSAGE FORMS AND STRENGTHS (4)
- Tablets (not scored): 2.5, 5, 7.5, 10, 15 mg (3)
CONTRAINDICATIONS
CONTRAINDICATIONS (5)
- None with olanzapine monotherapy
- When using olanzapine and fluoxetine in combination, also refer to the Contraindications section of the package insert for olanzapine and fluoxetine in combination.
- When using olanzapine in combination with lithium or valproate, refer to the Contraindications section of the package inserts for those products (4)
WARNINGS AND PRECAUTIONS
WARNINGS AND PRECAUTIONS (6)
- Elderly Patients with Dementia-Related Psychosis: Increased risk of death and increased incidence of cerebrovascular adverse events (e.g., stroke, transient, ischemic attack) (5.1)
- Suicide: The possibility of a suicide attempt is inherent in Schizophrenia and in Bipolar I Disorder, and close supervision of high-risk patients should accompany drug therapy; when using in combination with fluoxetine, also refer to the Boxed Warning and Warnings and Precautions sections of the package insert for olanzapine and fluoxetine in combination. (5.2).
- Neuroleptic Malignant Syndrome: manage with immediate discontinuation and close monitoring (5.3)
- Hyperglycemia: In some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients taking olanzapine. Patients taking olanzapine should be monitored for symptoms of hyperglycemia and undergo fasting blood glucose testing at the beginning of, and periodically during, treatment (5.4)Hyperlipidemia: Undesirbale alterations in lipids have been observed. Appropriate clinical monitoring is recommended, including fasting blood lipid testing at the beginning of, and periodically during, treatment (5.5)
- Weight Gain: Potential consequences of weight gain should be considered. Patients should receive regular monitor of weight (5.6)
- Tardive Dyskinesia: Discontinue if clinically appropriate (5.7)
- Orthostatic Hypotension: Orthostatic hypotension associated with dizziness, tachycardia, bradycardia and, in some patients, syncope, may occur especially during initial dose titration. Use caution in patients with cardiovascular disease, cerebrovascular disease, and those conditions that could affect hemodynamic responses (5.8)
- Leukopenia, Neutropenia, and Agranulocytosis : Has been reported with antipsychotics, including olanzapine. Patients with a history of a clinically significant low white blood cell count (WBC) or drug induced leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and discontinuation of planzapine should be considered at the first sign of a clinically significant decline in WBC in the absence of other causative factors (5.9)
- Seizures: Use cautiously in patients with history of seizures or with conditions that potentially lower the seizure threshold (5.11)
- Potential for Cognitive and Motor Impairment: has potential to impair judgement, thinking, and motor skills. Use caution when operating machinery (5.12)
- Hyperprolactinemia: may elevate prolactin levels (5.1)
- Use in Combination of Fluoxetine, Lithium or Valproate: Also refer to the package inserts of olanzapine and fluoxetine in combination, lithium or valporate (5.16)
- Laboratory Tests: Monitor fasting blood glucose and lipid profiles at the beginning of, and periodically during, treatment (5.17)
ADVERSE REACTIONS
ADVERSE REACTIONS (7)
(7)
(7)
Most common adverse reactions (greater than less than 5% and at least twice of placebo) associated with: Oral Olanzapine Monotherapy (7)
(7)
(7)
- Schizophrenia (Adults)- postural hypotension, constipation, weight gain, dizziness, personality disorder, akathisia (6.1)
- Schizophrenia (Adolescents)- sedation, weight increased, headache, increased appetitie, dizziness, abdominal pain, pain in extermity, fatigue, dry mouth (6.1)
Manic or Mixed Episodes, Bipolar I Disorder (Adults) (7)
- asthenia, dry mouth, weight gain, increased appetite, dizziness, back pain, constipation, speech disorder, increased salication, amnesia, parethesia (6.1) Olanzapine and Fluozetine in Combination: Also refer to the Adverse refer to the Adverse reactions section of the package insert for olanzapine and fluoxetine in combination (6) (7)
(7)
(7)
To report SUSPECTED ADVERSE REACTIONS, contact Teva USA, Pharmacovigilance at 1-888-838-2872 x6351 or drug.safety@tevausa.com; or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch (7)
(7)
(7)
DRUG INTERACTIONS
- Diazepam: May potentiate or orthostatic hypotension (7.1, 7.2)
- Alcohol: May potentiate orthostatic hypotension (7.1)
- Carboamazepine: Increased clearance of olanzapine (7.1)
- Fluvoxamine: May increase olanzapine levels (7.1)
- Olanzapine and Fluoxetine in Combination: Also refer to the Drug Interactions section of the package insert of olanzapine and fluoxetine in combination (7.1)
- CNS Acting Drugs: Caution should be used with taken in combination with other centrally acting drugs and alcohol (7.2)
- Antihypertensive Agents: Enhanced antihypertensive effect (7.2)
- Levodopa and Dopamine Agonists: May antagonize levodopa/dopamine agonists (7.2)
- Other Concomittant Drug Therapy: When using olanzapine in combination with lithium or valporate, refer to the Drug Interactions sections of the package insert for those products (7.2.)
USE IN SPECIFIC POPULATIONS
Enter highlights text here (9)
See 17 for PATIENT COUNSELING INFORMATION, PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 1/2013
FULL PRESCRIBING INFORMATION: CONTENTS*FULL PRESCRIBING INFORMATION
|
FULL PRESCRIBING INFORMATION
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
1.1 Schizophrenia
1.2 Bipolar I Disorder (Manic or Mixed Episodes)
1.3 Special Considerations in Treating Pediatric Schizophrenia and Bipolar I Disorder
1.5 Olanzapine and Fluoxetine in Combination: Depressive Episodes Associated with Bipolar I Disorder
2 DOSAGE AND ADMINISTRATION
2.1 Schizophrenia
2.2 Bipolar I Disorder (Manic or Mixed Episodes)
2.5 Olanzapine and Fluoxetine in Combination: Depressive Episodes Associated with Bipolar I Disorder
2.7 Olanzapine and Fluoxetine in Combination: Dosing in Special Population
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Elderly Patients with Dementia-Related Psychosis
5.2 Suicide
5.3 Neuroleptic Malignant Syndrome (NMS)
5.4 Hyperglycemia
5.5 Hyperlipidemia
5.6 Weight Gain
5.7 Tardive Dyskinesia
5.8 Orthostatic Hypotension
5.9 Leukopenia, Neutropenia, and Agranulocytosis
5.10 Dysphagia
5.11 Seizures
5.12 Potential for Cognitive and Motor Impairment
5.13 Body Temperature Regulation
5.14 Use in Patients with Concomitant Illness
5.15 Hyperprolactinemia
5.16 Use in Combination with Fluoxetine, Lithium or Valproate
5.17 Laboratory Tests
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Vital Signs and Laboratory Studies
6.3 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Potential for Other Drugs to Affect Olanzapine
7.2 Potential for Olanzapine to Affect Other Drugs
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Labor and Delivery
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
9 DRUG ABUSE AND DEPENDENCE
9.3 Dependence
10 OVERDOSAGE
10.1 Human Experience
10.2 Management of Overdose
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Schizophrenia
14.2 Bipolar I Disorder (Manic or Mixed Episodes)
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION
17.1 Information on Medication Guide
17.2 Elderly Patients with Dementia-Related Psychosis: Increased Mortality and Cerebrovascular Adverse Events (CVAE), Including Stroke
17.3 Neuroleptic Malignant Syndrome (NMS)
17.4 Hyperglycemia
17.5 Hyperlipidemia
17.6 Weight Gain
17.7 Orthostatic Hypotension
17.8 Potential for Cognitive and Motor Impairment
17.9 Body Temperature Regulation
17.10 Concomitant Medication
17.11 Alcohol
17.13 Use in Specific Populations
17.14 Need for Comprehensive Treatment Program in Pediatric Patients
Medication guide
PRINCIPAL DISPLAY PANEL
Olanzapine Tablets USP 2.5mg 30s Label Text
PRINCIPAL DISPLAY PANEL
Olanzapine Tablets USP 5mg 30s Label Text
PRINCIPAL DISPLAY PANEL
Olanzapine Tablets USP 7.5mg 30s Label Text
PRINCIPAL DISPLAY PANEL
Olanzapine Tablets USP 10mg 30s Label Text
PRINCIPAL DISPLAY PANEL
Olanzapine Tablets USP 15mg 30s Label Text
WARNING
INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analyses of seventeen placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. Olanzapine is not approved for the treatment of patients with dementia-related psychosis. [See Warnings and Precautions (
5.1
,
5.14
) and Patient Counseling Information (
17.2
)]. When using olanzapine and fluoxetine in combination, also refer to the Boxed Warning of the package insert for olanzapine and fluoxetine in combination.
DRUG ABUSE AND DEPENDENCE
9.3 Dependence
In studies prospectively designed to assess abuse and dependence potential, olanzapine was shown to have acute depressive CNS effects but little or no potential of abuse or physical dependence in rats administered oral doses up to 15 times the maximum recommended human daily dose (20 mg) and rhesus monkeys administered oral doses up to 8 times the maximum recommended human daily dose on a mg/m2 basis.
Olanzapine has not been systematically studied in humans for its potential for abuse, tolerance, or physical dependence. While the clinical trials did not reveal any tendency for any drug-seeking behavior, these observations were not systematic, and it is not possible to predict on the basis of this limited experience the extent to which a CNS-active drug will be misused, diverted, and/or abused once marketed. Consequently, patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of misuse or abuse of olanzapine (e.g., development of tolerance, increases in dose, drug-seeking behavior).
OVERDOSAGE
10.1 Human Experience
In premarketing trials involving more than 3100 patients and/or normal subjects, accidental or intentional acute overdosage of olanzapine was identified in 67 patients. In the patient taking the largest identified amount, 300 mg, the only symptoms reported were drowsiness and slurred speech. In the limited number of patients who were evaluated in hospitals, including the patient taking 300 mg, there were no observations indicating an adverse change in laboratory analytes or ECG. Vital signs were usually within normal limits following overdoses.
In postmarketing reports of overdose with olanzapine alone, symptoms have been reported in the majority of cases. In symptomatic patients, symptoms with greater than or equal to 10% incidence included agitation/aggressiveness, dysarthria, tacyhcardia, various extrapryramidal symptoms, and reduced level of consciousness ranging from sedation to coma. Among less commonly reported symptoms were the following potentially medically serious reactions: aspiration, cardiopulmonary arrest, cardiac arryhthmias 9such as supraventricular tachycardia and 1 patient experiencing sinus pause with spontaneious resumption of normal rhythm), delirium, possible neuroleptic malignant syndrom, respiratory depression/arrest, conculsion, hypertension, and hypotension. Eli Lilly and Company has received reports of fatality in association with overdose of onlazapine alone. In 1 case of death, the amount of acutely ingested olanzapine was reported to be possible as low as 450 mg of otal olanzapine; however, in aother case, a patient was reported to survive an acute olanzapine ingestion of approximately 2 g of oral olanzapine.
10.2 Management of Overdose
The possibility of multiple drug involvement should be considered. In case of acute overdosage, establish and maintain an airway and ensure adequate oxygenation and ventilation, which may include intubation. Gastric lavage (after intubation, if patient is unconscious) and administration of activated charcoal together with a laxative should be considered. The administration of activated charcoal (1 g) reduced the Cmax and AUC of oral olanzapine by about 60%. As peak olanzapine levels are not typically obtained until about 6 hours after dosing, charcoal may be a useful treatment for olanzapine overdose.
The possibility of obtundation, seizures, or dystonic reaction of the head and neck following overdose may create a risk of aspiration with induced emesis. Cardiovascular monitoring should commence immediately and should include continuous electrocardiographic monitoring to detect possible arrhythmias.
There is no specific antidote to olanzapine. Therefore, appropriate supportive measures should be initiated. Hypotension and circulatory collapse should be treated with appropriate measures such as intravenous fluids and/or sympathomimetic agents. (Do not use epinephrine, dopamine, or other sympathomimetics with beta-agonist activity, since beta stimulation may worsen hypotension in the setting of olanzapine-induced alpha blockade.) Close medical supervision and monitoring should continue until the patient recovers.
For specific information about overdosage with lithium or valproate, refer to the Overdosage section of the package inserts for these products.
DESCRIPTION
Olanzapine USP is an atypical psychotropic agent that belongs to the thienobenzodiazepine class. The chemical designation is 2-methyl-4-(4-methyl-1-piperazinyl)-10H-thieno[2,3-b] [1,5]benzodiazepine and has the following chemical structure:
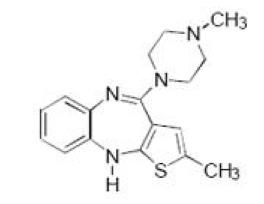
C17H20N4S M.W. 312.44
Olanzapine USP is a yellow crystalline solid, which is practically insoluble in water. Each tablet, for oral administration, contains olanzapine equivalent to 2.5 mg (8 micromol), 5 mg (16 micromol), 7.5 mg (24 micromol), 10 mg (32 micromol) or 15 mg (48 micromol) and has the following inactive ingredients: anhydrous lactose, carrageenan, crospovidone, magnesium stearate, microcrystalline cellulose, and polyethylene glycol. In addition, the 2.5 mg, 5 mg, 7.5 mg and 10 mg tablets contain titanium dioxide, and the 15 mg tablets contain FD&C blue #2 aluminum lake.
CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The mechanism of action of olanzapine, as with other drugs having efficacy in Schizophrenia, is unknown. However, it has been proposed that this drug's efficacy in Schizophrenia is mediated through a combination of dopamine and serotonin type 2 (5HT2) antagonism. The mechanism of action of olanzapine in the treatment of acute manic or mixed episodes associated with Bipolar I Disorder is unknown.
12.2 Pharmacodynamics
Olanzapine binds with high affinity to the following receptors: serotonin 5HT2A/2C, 5HT6 (Ki = 4, 11, and 5 nM, respectively), dopamine D1-4 (Ki=11-31 nM), histamine H1 (Ki = 7 nM), and adrenergicreceptors (Ki = 19 nM). Olanzapine is an antagonist with moderate affinity binding for serotonin 5HT3 (Ki = 57 nM) and muscarinic M1-5 (Ki = 73, 96, 132, 32, and 48 nM, respectively). Olanzapine binds weakly to GABAA, BZD, andreceptors (Ki >10
Antagonism at receptors other than dopamine and 5HT2 may explain some of the other therapeutic and side effects of olanzapine. Olanzapineantagonism of muscarinic M1-5 receptors may explain its anticholinergic-like effects. Olanzapineantagonism of histamine H1 receptors may explain the somnolence observed with this drug. Olanzapineantagonism of adrenergicreceptors may explain the orthostatic hypotension observed with this drug
12.3 Pharmacokinetics
Oral Administration, Monotherapy
Olanzapine is well absorbed and reaches peak concentrations in approximately 6 hours following an oral dose. It is eliminated extensively by first pass metabolism, with approximately 40% of the dose metabolized before reaching the systemic circulation. Food does not affect the rate or extent of olanzapine absorption. Pharmacokinetic studies showed that olanzapine tablets and olanzapine orally disintegrating tablets dosage forms of olanzapine are bioequivalent.
Olanzapine displaces linear kinetics over the clinical dosing range. its half-life ranges from 21 to 54 hours (5th to 95th percentile; mean of 30 hr), and apparent plasma clearance ranges from 12 to 47 L/hr (5th to 95th percentile; mean of 25 L/hr).
Administration of olanzapine once daily leads to steady-state concentrations in about 1 week that are approximately twice the concentrations after single doses. Plasma concentrations, half-life, and clearance of olanzapine may vary between individuals on the basis of smoking status, gender, and age [see Clinical Pharmacology (
12.3)].
Olanzapine is extensively distributed throughout the body, with a volume of distribution of approximately 1000 L. It is 93% bound to plasma proteins over the concentration range of 7 to 1100 ng per mL, binding primarily to albumin and a1-glycoprotein.
Metabolism and Elimination
Following a single oral dose of 14C labeled olanzapine, 7% of the dose of olanzapine was recovered in the urine as unchanged drug, indicating that olanzapine is highly metabolized. Approximately 57% and 30% of the dose was recovered in the urine and feces, respectively. In the plasma, olanzapine accounted for only 12% of the AUC for total radioactivity, indicating significant exposure to metabolites. After multiple dosing, the major circulating metabolites were the 10-N-glucuronide, present at steady state at 44% of the concentration of olanzapine, and 4'-N-desmethyl olanzapine, present at steady state at 31% of the concentration of olanzapine. Both metabolites lack pharmacological activity at the concentrations observed.
Direct glucuronidation and cytochrome P450 (CYP) mediated oxidation are the primary metabolic pathways for olanzapine. In vitro studies suggest that CYPs 1A2 and 2D6, and the flavin-containing monooxygenase system are involved in olanzapine oxidation. CYP2D6 mediated oxidation appears to be a minor metabolic pathway in vivo, because the clearance of olanzapine is not reduced in subjects who are deficient in this enzyme.
Specific Populations
Renal Impairment
Because olanzapine is highly metabolized before excretion and only 7% of the drug is excreted unchanged, renal dysfunction alone is unlikely to have a major impact on the pharmacokinetics of olanzapine. The pharmacokinetic characteristics of olanzapine were similar in patients with severe renal impairment and normal subjects, indicating that dosage adjustment based upon the degree of renal impairment is not required. In addition, olanzapine is not removed by dialysis. The effect of renal impairment on metabolite elimination has not been studied.
Hepatic Impairment
Although the presence of hepatic impairment may be expected to reduce the clearance of olanzapine, a study of the effect of impaired liver function in subjects (n = 6) with clinically significant (Childs Pugh Classification A and B) cirrhosis revealed little effect on the pharmacokinetics of olanzapine
Geriatric
In a study involving 24 healthy subjects, the mean elimination half-life of olanzapine was about 1.5 times greater in elderly (65 years) than in non-elderly subjects (< 65 years). Caution should be used in dosing the elderly, especially if there are other factors that might additively influence drug metabolism and/or pharmacodynamic sensitivity [see Dosage and Administration (
2)].
Gender
Clearance of olanzapine is approximately 30% lower in women than in men. There were, however, no apparent differences between men and women in effectiveness or adverse effects. Dosage modifications based on gender should not be needed.
Smoking Status
Olanzapine clearance is about 40% higher in smokers than in nonsmokers, although dosage modifications are not routinely recommended.
Race
In vivo studies have shown that exposures are similar among Japanese, Chinese and Caucasians, especially after normalization for body weight differences. Dosage modifications for race are, therefore, not recommended.
Combined Effects
The combined effects of age, smoking, and gender could lead to substantial pharmacokinetic differences in populations. The clearance in young smoking males, for example, may be 3 times higher than that in elderly nonsmoking females. Dosing modification may be necessary in patients who exhibit a combination of factors that may result in slower metabolism of olanzapine [see Dosage and Administration (
2)].
Adolescents (ages 13 to 17 years)
Pharmacokinetic information in pediatric patients is approved for Eli Lilly and Company's olanzapine drug product labeling. However, due to Eli Lilly and Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information
NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Oral carcinogenicity studies were conducted in mice and rats. Olazapine was administed to mice in two 78 week studies at doses of 3, 10, 30/20 mg/kg./day (equivalent to 0.8 to 5 times the maximum recommended human daily oral dose on a mg/m2 basis) and 0.25,2,8 mg/kg/day )(equivalent to 0.06 to 2 times the maximum recommended human daily oral dose on a mg/m2 basis). Rats were dosed for 2 years at doses of 0.25, 1, 2.5, 4 mg/kg/day (males) and 0.25, 1,4,8, mg/kg/day (females) (equivalent to 0.13 to 2 and o.13 to 4 times the maximum recommended human daily oral dose on a mg/m2 basis, respectively). The incidence of liver hemangiomas and hemangiosarcomas was significantly increased in 1 mouse study in female mice dosed at 8 mg/kg/day (2 times the maximum recommended human daily oral dose on a mg/m2 basis). These tumors were nt increased in another mouse study in females dosed at 10 or 30/20/mg/kg/day (2 to 5 times the maximum recommended human daily oral dose on a mg/m2 basis); in this study, there was a high incidence of early mortalities in males of the 30/20 mg/kg/day group. The incidence of mammary gland adenomas and adenocarcinomas was signifacntly increased in female mice dosed at greater than or equal to 2 mg/kg/day and in female rats dosed at greater than or equal to 4 mg/kg/day (0.5 and 2 times the maximum recommended human daily dose on a mg/m2 basis, recpectively). Antipsycholtic drugs have been shown to chronically elevate prolactin levels in rodents. Serum prolactin levels were not measured during the olanzapine carcinogencity studies; however, measurements during subchronic toxicity studies showed that olanzapine elevated serum prolactin levels up to 4 fold in rats at the same doses used in the carcinogenicity study. An increase in mammary gland neoplasms has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be prolactin mediated. The relevance for himan risk of the findig of prolactin mediated endocrine tumors in rodents is unknown [see Warnings and Precautions
5.15)].
Mutagenesis
No evidence of genotoxic potential for olanzapine was found in the Ames reverse mutation test, in vivo micronucleus test in mice, the chromosomal aberration test in Chinese hamster ovary cells, unscheduled DNA synthesis test in rat hepatocytes, induction of forward mutation test in mouse lymphoma cells, or in vivo sister chromatid exchange test in bone marrow of Chinese hamsters.
Impairment of Fertility
In am oral fertility and repoductive performance study in rats, male mating performance, but not fertility, was impaired at a dose of 22.4 mg/kg/day and female fertility was decreased at a dose of 3 mg/kg/day (11 and 1.5 times the maximum recommended human daily oral dose on mg/m2 basis respectively). Discontinuance of olazapine treatment reversed the effects on male mating performance. In female rats, the precoital period was increased and the mating index reduced at 5 mg/kg/day (2.5 times the maximum recommended human daily oral dose on a mg/m2 basis). Diestrous was prolonged and estrous delayed at 1.1 mg/kg/day (0.6 times the maximum recommended human daily oral dose on a mg/m2 basis); therefore olanzapine may produce a delay in ovulation.
13.2 Animal Toxicology and/or Pharmacology
In animal studies with olanzapine, the principal hematologic findings were reversible peripheral cytopenias in individual dogs dosed at 10 mg/kg (17 times the maximum recommended human daily oral dose on a mg/m2 basis), dose-related decreases in lymphocytes and neutrophils in mice, and lymphopenia in rats. A few dogs treated with 10 mg/kg developed reversible neutropenia and/or reversible hemolytic anemia between 1 and 10 months of treatment. Dose-related decreases in lymphocytes and neutrophils were seen in mice given doses of 10 mg/kg (equal to 2 times the maximum recommended human daily oral dose on a mg/m2 basis) in studies of 3 monthsduration. Nonspecific lymphopenia, consistent with decreased body weight gain, occurred in rats receiving
22.5 mg/kg (11 times the maximum recommended human daily oral dose on a mg/m2 basis) for 3 months or 16 mg/kg (8 times the maximum recommended human daily oral dose on a mg/m2 basis) for 6 or 12 months. No evidence of bone marrow cytotoxicity was found in any of the species examined. Bone marrows were normocellular or hypercellular, indicating that the reductions in circulating blood cells were probably due to peripheral (non-marrow) factors.
CLINICAL STUDIES
When using olanzapine and fluoxetine in combination, also refer to the Clinical Studies section of the package insert for olanzapine and fluoxetine in combination.
14.1 Schizophrenia
Adults
The efficacy of oral olanzapine in the treatment of Schizophrenia was established in 2 short-term (6 week) controlled trials of adult inpatients who met DSM III-R criteria for Schizophrenia. A single haloperidol arm was included as a comparative treatment in 1 of the 2 trials, but this trial did not compare these 2 drugs on the full range of clinically relevant doses for both.
Several instruments were used for assessing psychiatric signs and symptoms in these studies, among them the Brief Psychiatric Rating Scale (BPRS), a multi-item inventory of general psycholpathology traditionally used to evaluate the effects of drug treatment in Schizophrenia. The BPRS psychosis cluster (conceptual disorganization, halluniatory behavior, suspiciousness, and unusual thought content) is considered a particularly useful subset for assessing actively psychotic schizophrenic patients. A second traditional assessment, the Clinical Global Impression (CGI), reflects the impression of a skilled observer, fully familiar with the manifestations of Schizohrenia, about the overall clinical state of the patient. In addition, 2 more recently developed scales were employed; these included the 30-item Positive and Negative Symptoms Scale (PANSS), in which are embedded the 18 items of the BPRS, and the Scale for Assessing Negative Symptoms (SANS). The trial summaries below focus on the following outcomes: PANSS total and/or BPRS total; BPRS psychosis cluster; PANSS negative subscale or SANS; and CGI Severity. The results of the trials follow:
(1) In a 6 week, placebo-controlled trial (n = 149) involving 2 fixed olanzapine doses of 1 and 10 mg/day (once daily schedule), olanzapine, at 10 mg/day (but not at 1 mg/day), was superior to placebo on the PANSS total score (also on the extracted BPRS total), on the BPRS psychosis cluster, on the PANSS Negative subscale, and on CGI Severity.
(2) In a 6 week, placebo-controlled trial (n = 253) involving 3 fixed dose ranges of olanzapine (5 (+/-)2.5 mg/day, 10 (+/-) 2.5 mg/day, and 15 (+/-) 2.5 mg/day) on a once daily schedule, the 2 highest olanzapine dose groups (actual man doses of 12 and 16 mg/day, respectively) were superior to placebo on BPRS total score, BPRS psychosis cluster, and CGI severity score; the highest olanzapine dose group was superior to placebo on the SANS. There was no clear advantage for the high-dose group over the medium-dose group.
(3) In a longer-term trial, adult outpatients (n = 326) who predominantly met DSM-IV criteria for Schizophrenia and who remained stable on olanzapine during open-label treatment for at least 8 weeks were randomized to continuation on their current olanzapine doses (ranging from 10 to 20 mg/day) or to placebo. The follow-up period to observe patients for relapse, defined in terms of increases in BPRS positive symptoms or hospitalization, was planned for 12 months, however, criteria were met for stopping the trial early due to an excess of placebo relapses compared to olanzapine relapses, and olanzapine was superior to placebo on time to relapse, the primary outcome for this study. Thus, olanzapine was more effective than placebo at maintaining efficacy in patients stabilized for approximately 8 weeks and followed for an observation period of up to 8 months.
Examination of population subsets (race and gender) did not reveal any differential responsiveness on the basis of these subgroupings.
Adolescents
Clinical trial information in pediatric patients with schizophrenia is approved for Eli Lilly and Company's olanzapine drug product labeling. However, due to Eli Lilly and Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
14.2 Bipolar I Disorder (Manic or Mixed Episodes)
Adults
Monotherapy
The efficacy of oral olanzapine in the treatment of acute manic or mixed episodes was established in 2 short-term (one 3 week and one 4 week) placebo-controlled trials in adult patients who met the DSM-IV criteria for Bipolar I Disorder with manic or mixed episodes. These trials included patients with or without psychotic features and with or without a rapid-cycling course.
The primary rating instrument used for assessing manic symptoms in these trials was the Young Mania Rating Scale (Y-MRS), an 11-item clinician-rated scale traditionally used to assess the degree of manic symptomatology (irritability, disruptive/aggressive behavior, sleep, elevated mood, speech, increased activity, sexual interest, language/thought disorder, thought content, appearance, and insight) in a range from 0 (no manic features) to 60 (maximum score). The primary outcome in these trials was change from baseline in the Y-MRS total score. The results of the trials follow:
(1) In one 3 week placebo-controlled trial (n = 67) which involved a dose range of olanzapine (5 to 20 mg/day, once daily, starting at 10 mg/day), olanzapine was superior to placebo in the reduction of Y-MRS total score. In an identically designed trial conducted simultaneously with the first trial, olanzapine demonstrated a similar treatment difference, but possibly due to sample size and site variability, was not shown to be superior to placebo on this outcome.
(2) In a 4 week placebo-controlled trial (n = 115) which involved a dose range of olanzapine (5 to 20 mg/day, once daily, starting at 15 mg/day), olanzapine was superior to placebo in the reduction of Y-MRS total score.
(3) In another trial, 361 patients meeting DSM-IV criteria for a manic or mixed episode of Bipolar I Disorder who had responded during an initial open-label treatment phase for about 2 weeks, on average, to olanzapine 5 to 20 mg/day were randomized to either continuation of olanzapine at their same dose (n = 225) or to placebo (n = 136), for observation of relapse. Approximately 50% of the patients had discontinued from the olanzapine group by day 59 and 50% of the placebo group had discontinued by day 23 of double-blind treatment. Response during the open-label phase was defined by having a decrease of the Y-MRS total score to less than or equal to 12 and HAM-D 21 to less than or equal to 8. Relapse during the double-blind phase was defined as an increase of the Y-MRS or HAM-D 21 total score to greater than or equal to 15, or being hospitalized for either mania or depression. In the randomized phase, patients receiving continued olanzapine experienced a significantly longer time to relapse.
Adjunct to Lithium or Valproate
The efficacy of oral olanzapine with concomitant lithium or valproate in the treatment of acute manic or mixed episodes was established in 2 controlled trials in patients who met the DSM-IV criteria for Bipolar I Disorder with manic or mixed episodes. These trials included patients with or without psychotic features and with or without a rapid-cycling course. The results of the trials follow:
(1) In one 6 week placebo-controlled combination trial, 175 outpatients on lithium or valproate therapy with inadequately controlled manic or mixed symptoms (Y-MRSgreater than or equal to 16) were randomized to receive either olanzapine or placebo, in combination with their original therapy. Olanzapine (in a dose range of 5 to 20 mg/day, once daily, starting at 10 mg/day) combined with lithium or valproate (in a therapeutic range of 0.6 mEq/L to 1.2 mEq/L or 50 ug per mL to 125 ug per mL, respectively) was superior to lithium or valproate alone in the reduction of Y-MRS total score.
(2) In a second 6-week placebo-controlled combination trial, 169 outpatients on lithium or valproate therapy with inadequately controlled manic or mixed symptoms (Y-MRS greater than or equal to 16) were randomized to receive either olanzapine or placebo, in combination with their original therapy. Olanzapine (in a dose range of 5 to 20 mg/day, once daily, starting at 10 mg/day) combined with lithium or valproate (in a therapeutic range of 0.6 mEq/L to 1.2 mEq/L or 50 ug per mL to 125 ug per mL, respectively) was superior to lithium or valproate alone in the reduction of Y-MRS total score.
Adolescents
Clinical trial information in pediatric patients with bipolar I disorder is approved for Eli Lilly and Company's olanzapine drug product labeling. However, due to Eli Lilly and Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
PATIENT COUNSELING INFORMATION
See the FDA-approved Medication Guide for the oral formulations.
Patients should be advised of the following issues and asked to alert their prescriber if these occur while taking olanzapine. If you do not think you are getting better or have any concerns about your condition while taking olanzapine, call your doctor. When using olanzapine and fluoxetine in combination, also refer to the Patient Counseling Information section of the package insert for olanzapine and fluoxetine in combination.
17.1 Information on Medication Guide
Prescribers or other health professionals should inform patients, their families, and their caregivers about the potential benefits and potential risks associated with treatment with olanzapine, and should counsel them in its appropriate use. A patient Medication Guide is available for olanzapine. Prescribers or other health professionals should instruct patients, their families, and their caregivers to read the Medication Guide and should assist them in understanding its contents. Patients should be given the opportunity to discuss the contents of the Medication Guide and to obtain answers to any questions they may have. When using olanzapine and fluoxetine in combination, also refer to the Medication Guide for olanzapine and fluoxetine in combination.
17.2 Elderly Patients with Dementia-Related Psychosis: Increased Mortality and Cerebrovascular Adverse Events (CVAE), Including Stroke Patients and caregivers should be advised that elderly patients with dementia-related psychosis treated with antipsychotic drugs are at increased risk of death. Patients and caregivers should be advised that elderly patients with dementia-related psychosis treated with olanzapine had a significantly higher incidence of cerebrovascular adverse events (e.g., stroke, transient ischemic attack) compared with placebo.
Olanzapine is not approved for elderly patients with dementia-related psychosis [see Boxed Warning and Warnings and Precautions (
5.1)].
17.3 Neuroleptic Malignant Syndrome (NMS)
Patients and caregivers should be counseled that a potentially fatal symptom complex sometimes referred to as NMS has been reported in association with administration of antipsychotic drugs, including olanzapine. Signs and symptoms of NMS include hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia) [see Warnings and Precautions (
5.3)].
17.4 Hyperglycemia
Patients should be advised of the potential risk of hyperglycemia-related adverse reactions. Patients should be monitored regularly for worsening of glucose control. Patients who have diabetes should follow their doctorinstructions about how often to check their blood sugar while taking olanzapine [see Warnings and Precautions (
5.4)].
17.5 Hyperlipidemia
Patients should be counseled that hyperlipidemia has occurred during treatment with olanzapine. Patients should have their lipid profile monitored regularly [see Warnings and Precautions (
5.5)].
17.6 Weight Gain
Patients should be counseled that weight gain has occurred during treatment with olanzapine. Patients should have their weight monitored regularly [see Warnings and Precautions (
5.6)].
17.7 Orthostatic Hypotension
Patients should be advised of the risk of orthostatic hypotension, especially during the period of initial dose titration and in association with the use of concomitant drugs that may potentiate the orthostatic effect of olanzapine, e.g., diazepam or alcohol [see Warnings and Precautions (
5.8) and Drug Interactions (7). Patients should be advised to change positions carefully to help prevent orthostatic hypotension, and to lie down if they feel dizzy or faint, until they feel better. Patients should be advised to call their doctor if they experience any of the following signs and symptoms associated with orthostatic hypotension: dizziness, fast or slow heart beat, or fainting.
17.8 Potential for Cognitive and Motor Impairment
Because olanzapine has the potential to impair judgment, thinking, or motor skills, patients should be cautioned about operating hazardous machinery, including automobiles, until they are reasonably certain that olanzapine therapy does not affect them adversely [see Warnings and Precautions (
5.12)].
17.9 Body Temperature Regulation
Patients should be advised regarding appropriate care in avoiding overheating and dehydration. Patients should be advised to call their doctor right away if they become severely ill and have some or all of these symptoms of dehydration: sweating too much or not at all, dry mouth, feeling very hot, feeling thirsty, not able to produce urine [see Warnings and Precautions (
5.13)].
Patients should be advised to inform their physicians if they are taking, or plan to take, olanzapine and fluoxetine in combination. Patients should also be advised to inform their physicians if they are taking, plan to take, or have stopped taking any prescription or over-the-counter drugs, including herbal supplements, since there is a potential for interactions [see Drug Interactions (
7)].
17.11 Alcohol
Patients should be advised to avoid alcohol while taking olanzapine [see Drug Interactions (
7)].
17.13 Use in Specific Populations
Pregnancy
Patients should be advised to notify their physician if they become pregnant or intend to become pregnant during therapy with olanzapine [see Use in Specific Populations
8.1)].
Nursing Mothers
Patients should be advised not to breast-feed an infant if they are taking olanzapine [see Use in Specific Populations (
8.3)].
Pediatric Use
Compared to patients from adult clinical trials, adolescents were likely to gain more weight, experience increased sedation, and have greater increases in total cholesterol, triglycerides, LDL cholesterol, prolactin and hepatic transaminase levels. Safety and effectiveness of olanzapine in patients under 13 years of age have not been established. Safety and effectiveness of olanzapine and fluoxetine in combination in patients < 18 years of age have not been established [see Warnings and Precautions (
5.5, 5.6) and Use in Specific Populations ( 8.4).
Pediatric use information in pediatric patients with schizophrenia and bipolar I disorder is approved for Eli Lilly and Companyolanzapine drug product labeling. However, due to Eli Lilly and Companymarketing exclusivity rights, this drug product is not labeled with that pediatric information.
17.14 Need for Comprehensive Treatment Program in Pediatric Patients
Pediatric use information in pediatric patients with schizophrenia and bipolar I disorder is approved for Eli Lilly and Company's olanzapine drug product labeling. However, due to Eli Lilly and Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
Medication Guide
Olanzapine Tablets USP
Read the Medication Guide that comes with olanzapine before you start taking it and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your doctor about your medical condition or treatment. Talk with your doctor or pharmacist if there is something you do not understand or you want to learn more about olanzapine.
What is the most important information I should know about olanzapine
Olanzapine may cause serious side effects, including:
1. Increased risk of death in elderly people who are confused, have memory loss and have lost touch with reality (dementia-related psychosis).
2. High blood sugar (hyperglycemia).
3. High fat levels in your blood (increased cholesterol and triglycerides), especially in teenagers age 13 to 17.
4. Weight gain, especially in teenagers age 13 to 17.
These serious side effects are described below.
1. Increased risk of death in elderly people who are confused, have memory loss and have lost touch with reality (dementia-related psychosis).Olanzapine is not approved for treating psychosis in elderly people with dementia.
2. High blood sugar (hyperglycemia).High blood sugar can happen if you have diabetes already or if you have never had diabetes. High blood sugar could lead to:
a build up of acid in your blood due to ketones (ketoacidosis)
coma
death
If you have diabetes, follow your doctorinstructions about how often to check your blood sugar while taking olanzapine.
Call your doctorif you have any of these symptoms of high blood sugar (hyperglycemia) while taking olanzapine:
feel very thirsty
need to urinate more than usual
feel very hungry
feel weak or tired
feel sick to your stomach
feel confused, or your breath smells fruity.
3. High fat levels in your blood (cholesterol and triglycerides).High fat levels may happen in people treated with olanzapine, especially in teenagers (13 to 17 years old). You may not have any symptoms, so your doctor should do blood tests to check your cholesterol and triglyceride levels before you start taking olanzapine and during treatment.
4. Weight gain.Weight gain is very common in people who take olanzapine. Teenagers (13 to 17 years old) are more likely to gain weight and to gain more weight than adults. Some people may gain a lot of weight while taking olanzapine, so you and your doctor should check your weight regularly. Talk to your doctor about ways to control weight gain, such as eating a healthy, balanced diet, and exercising.
What is olanzapine?
Olanzapine is a prescription medicine used to treat:
schizophrenia.
bipolar disorder, including:
manic or mixed episodes that happen with bipolar I disorder.
manic or mixed episodes that happen with bipolar I disorder, when used with the medicine lithium or valproate, in adults.
long-term treatment of bipolar I disorder in adults.
episodes of depression that happen with bipolar I disorder, when used with the medicine fluoxetine, in adults
Olanzapine has not been approved for use in children under 13 years of age.
The symptoms of schizophrenia include hearing voices, seeing things that are not there, having beliefs that are not true, and being suspicious or withdrawn.
The symptoms of bipolar I disorder include alternating periods of depression and high or irritable mood, increased activity and restlessness, racing thoughts, talking fast, impulsive behavior, and a decreased need for sleep.
Some of your symptoms may improve with treatment. If you do not think you are getting better, call your doctor.
Pediatric use information is approved for Eli Lilly and Companyolanzapine drug listing product labeling. However, due to Eli Lilly and Companymarketing exclusivity rights, this drug product is not labeled with that pediatric information.
What should I tell my doctor before taking olanzapine?
Olanzapine may not be right for you. Before starting olanzapine, tell your doctor if you have or had:
heart problems
seizures
diabetes or high blood sugar levels (hyperglycemia)
high cholesterol or triglyceride levels in your blood
liver problems
low or high blood pressure
strokes oralso called transient ischemic attacks (TIAs)
Alzheimerdisease
narrow-angle glaucoma
enlarged prostate in men
bowel obstruction
breast cancer
thoughts of suicide or hurting yourself
any other medical condition
are pregnant or plan to become pregnant. It is not known if olanzapine will harm your unborn baby.
are breast-feeding or plan to breast-feed. Olanzapine can pass into your breast milk and may harm your baby. You should not breast-feed while taking olanzapine. Talk to your doctor about the best way to feed your baby if you take olanzapine.
Tell your doctor if you exercise a lot or are in hot places often.
The symptoms of Bipolar I Disorder, treatment resistant depression, or schizophrenia may include
thoughts of suicideor of hurting yourself or others. If you have these thoughts at any time, tell your doctor or go to an emergency room right away.
Tell your doctor about all the medicines that you take, including prescription and non-prescription medicines, vitamins, and herbal supplements. Olanzapine and some medicines may interact with each other and may not work as well, or cause possible serious side effects. Your doctor can tell you if it is safe to take olanzapine with your other medicines. Do not start or stop any medicine while taking olanzapine without talking to your doctor first.
How should I take olanzapine?
Take olanzapine exactly as prescribed. Your doctor may need to change (adjust) the dose of olanzapine until it is right for you.
If you miss a dose of olanzapine, take the missed dose as soon as you remember. If it is almost time for the next dose, just skip the missed dose and take your next dose at the regular time. Do not take two doses of olanzapine at the same time.
To prevent serious side effects, do not stop taking olanzapine suddenly. If you need to stop taking olanzapine, your doctor can tell you how to safely stop taking it.
If you take too much olanzapine, call your doctor or poison control center right away at 1-800-222-1222, or get emergency treatment.
Olanzapine can be taken with or without food.
Olanzapine is usually taken one time each day.
Call your doctor if you do not think you are getting better or have any concerns about your condition while taking olanzapine.
What should I avoid while taking olanzapine?
Olanzapine can cause sleepiness and may affect your ability to make decisions, think clearly, or react quickly. You should not drive, operate heavy machinery, or do other dangerous activities until you know how olanzapine affects you.
Avoid drinking alcohol while taking olanzapine. Drinking alcohol while you take olanzapine may make you sleepier than if you take olanzapine alone.
What are the possible side effects of olanzapine?
Serious side effects may happen when you take olanzapine, including:
Seeis the most important information I should know about olanzapine?which describes the increased risk of death in elderly people with dementia-related psychosis and the risks of high blood sugar, high cholesterol and triglyceride levels, and weight gain.
Increased incidence of stroke orcalled transient ischemic attacks (TIAs) in elderly people with dementia-related psychosis(elderly people who have lost touch with reality due to confusion and memory loss). Olanzapine is not approved for these patients.
Neuroleptic Malignant Syndrome (NMS):NMS is a rare but very serious condition that can happen in people who take antipsychotic medicines, including olanzapine. NMS can cause death and must be treated in a hospital. Call your doctor right away if you become severely ill and have any of these symptoms:
high fever
excessive sweating
rigid muscles
confusion
changes in your breathing, heartbeat, and blood pressure
Tardive Dyskinesia:This condition causes body movements that keep happening and that you cannot control. These movements usually affect the face and tongue. Tardive dyskinesia may not go away, even if you stop taking olanzapine. It may also start after you stop taking olanzapine. Tell your doctor if you get any body movements that you cannot control.
Decreased blood pressure when you change positions, with symptoms of dizziness, fast or slow heart beat, or fainting.
Difficulty swallowing, that can cause food or liquid to get into your lungs.
Seizures: Tell your doctor if you have a seizure during treatment with olanzapine.
Problems with control of body temperature:You could become very hot, for instance when you exercise a lot or stay in an area that is very hot. It is important for you to drink water to avoid dehydration. Call your doctor right away if you become severely ill and have some or all of these symptoms of dehydration:
sweating too much or not at all
dry mouth
feeling very hot
feeling thirsty
not able to produce urine
Common possible side effects of olanzapine include:lack of energy, dry mouth, increased appetite, sleepiness, tremor (shakes), having hard or infrequent stools, dizziness, changes in behavior, or restlessness.
Other common side effects in teenagers (13 to 17 years old) include:headache, stomach-area (abdominal) pain, pain in your arms or legs, or tiredness. Teenagers experienced greater increases in prolactin, liver enzymes, and sleepiness, as compared with adults.
Tell your doctor about any side effect that bothers you or that does not go away.
These are not all the possible side effects with olanzapine. For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store olanzapine?
Store olanzapine at room temperature, between 68 F to 77 F(20 C to 25 C).
Keep olanzapine away from light.
Keep olanzapine dry and away from moisture.
Keep olanzapine and all medicines out of the reach of children.
General information about olanzapine
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use olanzapine for a condition for which it was not prescribed. Do not give olanzapine to other people, even if they have the same condition. It may harm them.
This Medication Guide summarizes the most important information about olanzapine. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist for information about olanzapine that was written for healthcare professionals. For more information about olanzapine call Teva Pharmaceuticals Medical Affairs at 1-888-838-2872.
What are the ingredients in olanzapine tablets USP?
Active ingredient:olanzapine USP
Inactive ingredients:anhydrous lactose, carrageenan, crospovidone, magnesium stearate, microcrystalline cellulose, and polyethylene glycol. In addition, the 2.5 mg, 5 mg, 7.5 mg and 10 mg tablets contain titanium dioxide, and the 15 mg tablets contain FD&C blue #2 aluminum lake.
This Medication Guide has been approved by the U.S. Food and Drug Administration.

| OLANZAPINE
olanzapine tablet, film coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - REMEDYREPACK INC. (829572556) |