LISINOPRIL
-
lisinopril tablet, film coated
NCS HealthCare of KY, Inc dba Vangard Labs
----------
BOXED WARNING
USE IN PREGNANCY
When used in pregnancy during the second and third trimesters, ACE inhibitors can cause
injury and even death to the developing fetus. When pregnancy is detected, Lisinopril tablet should
When pregnancy is detected, Lisinopril tablet should
be discontinued as soon as possible. See WARNINGS, Fetal/Neonatal Morbidity and Mortality.
DESCRIPTION
Lisinopril is an oral long-acting angiotensin converting enzyme inhibitor. Lisinopril, a synthetic peptide
derivative, is chemically described as (S)-1-[N2-(1-carboxy-3- phenylpropyl)-L-lysyl]-L-proline dihydrate.
Its empirical formula is C21H31N3O5.2H2O and its structural formula is:
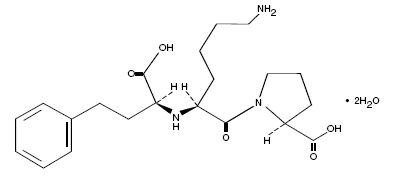
Lisinopril is a white to off-white, crystalline powder, with a molecular weight of 441.53. It is soluble in
water and sparingly soluble in methanol and practically insoluble in ethanol.
Lisinopril tablet is supplied as 2.5 mg, 5 mg, 10 mg, 20 mg, 30 mg and 40 mg tablets for oral
administration.
Inactive Ingredients:
2.5 mg, 5 mg, 10 mg tablets – dibasic calcium phosphate dihydrate, povidone, pregelatinized starch,
mannitol, colloidal silicon dioxide, corn starch, magnesium stearate.
20 mg, 30 mg, 40 mg tablets - dibasic calcium phosphate dihydrate, povidone, pregelatinized starch,
mannitol, colloidal silicon dioxide, corn starch, magnesium stearate, ferric oxide yellow (for 20 mg),
ferric oxide red (for 30 mg) and ferric oxide brown (for 40 mg).
CLINICAL PHARMACOLOGY
MECHANISM OF ACTION
Lisinopril inhibits angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a
peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance,
angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. The
beneficial effects of lisinopril in hypertension and heart failure appear to result primarily from
suppression of the reninangiotensin- aldosterone system. Inhibition of ACE results in decreased
plasma angiotensin II which leads to decreased vasopressor activity and to decreased aldosterone
secretion. The latter decrease may result in a small increase of serum potassium. In hypertensive
patients with normal renal function treated with Lisinopril tablet alone for up to 24 weeks, the mean
increase in serum potassium was approximately 0.1 mEq/L; however, approximately 15% of patients
had increases greater than 0.5 mEq/L and approximately 6% had a decrease greater than 0.5 mEq/L.
In the same study, patients treated with Lisinopril tablet and hydrochlorothiazide for up to 24 weeks
had a mean decrease in serum potassium of 0.1 mEq/L; approximately 4% of patients had increases
greater than 0.5 mEq/L and approximately 12% had a decrease greater than 0.5 mEq/L. (See
PRECAUTIONS.) Removal of angiotensin II negative feedback on renin secretion leads to increased
plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of
bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of Lisinopril tablet
remains to be elucidated.
While the mechanism through which Lisinopril tablet lowers blood pressure is believed to be primarily
suppression of the reninangiotensin-aldosterone system, Lisinopril tablet is antihypertensive even in
patients with low-renin hypertension. Although Lisinopril tablet was antihypertensive in all races
studied, Black hypertensive patients (usually a low-renin hypertensive population) had a smaller
average response to monotherapy than non-Black patients.
Concomitant administration of Lisinopril tablet and hydrochlorothiazide further reduced blood pressure
in Black and non-Black patients and any racial differences in blood pressure response were no longer
evident.
Pharmacodynamics
Pharmacodynamics and Clinical Effects
Hypertension
Adult Patients: Administration of Lisinopril tablet to patients with hypertension results in a reduction of
Administration of Lisinopril tablet to patients with hypertension results in a reduction of
both supine and standing blood pressure to about the same extent with no compensatory tachycardia.
Symptomatic postural hypotension is usually not observed although it can occur and should be
anticipated in volume and/or salt-depleted patients. (See WARNINGS.) When given together with
thiazide-type diuretics, the blood pressure lowering effects of the two drugs are approximately additive.
In most patients studied, onset of antihypertensive activity was seen at one hour after oral
administration of an individual dose of Lisinopril tablet, with peak reduction of blood pressure achieved
by 6 hours. Although an antihypertensive effect was observed 24 hours after dosing with
recommended single daily doses, the effect was more consistent and the mean effect was
considerably larger in some studies with doses of 20 mg or more than with lower doses. However, at
all doses studied, the mean antihypertensive effect was substantially smaller 24 hours after dosing
than it was 6 hours after dosing.
In some patients achievement of optimal blood pressure reduction may require two to four weeks of
therapy.
The antihypertensive effects of Lisinopril tablet are maintained during long-term therapy. Abrupt
withdrawal of Lisinopril tablet has not been associated with a rapid increase in blood pressure, or a
significant increase in blood pressure compared to pretreatment levels.
Two dose-response studies utilizing a once-daily regimen were conducted in 438 mild to moderate
hypertensive patients not on a diuretic. Blood pressure was measured 24 hours after dosing. An
antihypertensive effect of Lisinopril tablet was seen with 5 mg in some patients. However, in both
studies blood pressure reduction occurred sooner and was greater in patients treated with 10, 20 or 80
mg of Lisinopril tablet. In controlled clinical studies, Lisinopril tablet 20-80 mg has been compared in
patients with mild to moderate hypertension to hydrochlorothiazide 12.5-50 mg and with atenolol 50-
200 mg; and in patients with moderate to severe hypertension to metoprolol 100-200 mg. It was
superior to hydrochlorothiazide in effects on systolic and diastolic pressure in a population that was 3/4
Caucasian. Lisinopril tablet was approximately equivalent to atenolol and metoprolol in effects on
diastolic blood pressure, and had somewhat greater effects on systolic blood pressure.
Lisinopril tablet had similar effectiveness and adverse effects in younger and older (>65 years)
patients. It was less effective in Blacks than in Caucasians.
In hemodynamic studies in patients with essential hypertension, blood pressure reduction was
accompanied by a reduction in peripheral arterial resistance with little or no change in cardiac output
and in heart rate. In a study in nine hypertensive patients, following administration of Lisinopril tablet,
there was an increase in mean renal blood flow that was not significant. Data from several small
studies are inconsistent with respect to the effect of lisinopril on glomerular filtration rate in
hypertensive patients with normal renal function, but suggest that changes, if any, are not large.
In patients with renovascular hypertension Lisinopril tablet has been shown to be well tolerated and
effective in controlling blood pressure. (See PRECAUTIONS.)
Pediatric Patients: In a clinical study involving 115 hypertensive pediatric patients 6 to 16 years of age,
In a clinical study involving 115 hypertensive pediatric patients 6 to 16 years of age,
patients who weighed <50 kg received either 0.625, 2.5 or 20 mg of lisinopril daily and patients who
weighed ≥50 kg received either 1.25, 5, or 40 mg of lisinopril daily. At the end of 2 weeks, lisinopril
administered once daily lowered trough blood pressure in a dose-dependent manner with consistent
antihypertensive efficacy demonstrated at doses >1.25 mg (0.02 mg/kg). This effect was confirmed in
a withdrawal phase, where the diastolic pressure rose by about 9 mmHg more in patients randomized
to placebo than it did in patients who were randomized to remain on the middle and high doses of
lisinopril. The dose-dependent antihypertensive effect of lisinopril was consistent across several
demographic subgroups: age, Tanner stage, gender, and race. In this study, lisinopril was generally
well tolerated.
In the above pediatric studies, lisinopril was given either as tablets or in a suspension for those
children and infants who were unable to swallow tablets or who required a lower dose than is available
in tablet form (see DOSAGE AND ADMINISTRATION, Preparation of Suspension).
Heart Failure: During baseline-controlled clinical trials, in patients receiving digitalis and diuretics,
During baseline-controlled clinical trials, in patients receiving digitalis and diuretics,
single doses of Lisinopril tablet resulted in decreases in pulmonary capillary wedge pressure, systemic
vascular resistance and blood pressure accompanied by an increase in cardiac output and no change
in heart rate.
In two placebo controlled, 12-week clinical studies using doses of Lisinopril tablet up to 20 mg,
Lisinopril tablet as adjunctive therapy to digitalis and diuretics improved the following signs and
symptoms due to congestive heart failure: edema, rales, paroxysmal nocturnal dyspnea and jugular
venous distention. In one of the studies, beneficial response was also noted for: orthopnea, presence
of third heart sound and the number of patients classified as NYHA Class III and IV. Exercise tolerance
was also improved in this study. The once-daily dosing for the treatment of congestive heart failure
was the only dosage regimen used during clinical trial development and was determined by the
measurement of hemodynamic response. A large (over 3000 patients) survival study, the ATLAS Trial,
comparing 2.5 and 35 mg of lisinopril in patients with heart failure, showed that the higher dose of
lisinopril had outcomes at least as favorable as the lower dose.
Acute Myocardial Infarction: The Gruppo Italiano per lo Studio della Sopravvienza nell’Infarto
The Gruppo Italiano per lo Studio della Sopravvienza nell’Infarto
Miocardico (GISSI-3) study was a multicenter, controlled, randomized, unblended clinical trial
conducted in 19,394 patients with acute myocardial infarction admitted to a coronary care unit. It was
designed to examine the effects of short-term (6 week) treatment with lisinopril, nitrates, their
combination, or no therapy on short-term (6 week) mortality and on long term death and markedly
impaired cardiac function. Patients presenting within 24 hours of the onset of symptoms who were
hemodynamically stable were randomized, in a 2 x 2 factorial design, to six weeks of either 1) Lisinopril
tablet alone (n=4841), 2) nitrates alone (n=4869), 3) Lisinopril tablet plus nitrates (n=4841), or 4) open
control (n=4843). All patients received routine therapies, including thrombolytics (72%), aspirin (84%),
and a beta-blocker (31%), as appropriate, normally utilized in acute myocardial infarction (MI) patients.
The protocol excluded patients with hypotension (systolic blood pressure ≤100 mmHg), severe heart
failure, cardiogenic shock, and renal dysfunction (serum creatinine >2 mg/dL and/or proteinuria >500
mg/24 h). Doses of Lisinopril tablet were adjusted as necessary according to protocol (see DOSAGE
AND ADMINISTRATION).
Study treatment was withdrawn at six weeks except where clinical conditions indicated continuation of
treatment.
The primary outcomes of the trial were the overall mortality at 6 weeks and a combined end point at 6
months after the myocardial infarction, consisting of the number of patients who died, had late (day 4)
clinical congestive heart failure, or had extensive left ventricular damage defined as ejection fraction
≤35% or an akinetic-dyskinetic [A-D] score ≥45%. Patients receiving Lisinopril tablet (n=9646), alone or
with nitrates, had an 11% lower risk of death (2p [two tailed] = 0.04) compared to patients receiving no
Lisinopril tablet (n=9672) (6.4% vs. 7.2%, respectively) at six weeks. Although patients randomized to
receive Lisinopril tablet for up to six weeks also fared numerically better on the combined end point at
6 months, the open nature of the assessment of heart failure, substantial loss to follow-up
echocardiography, and substantial excess use of lisinopril between 6 weeks and 6 months in the group
randomized to 6 weeks of lisinopril, preclude any conclusion about this end point.
Patients with acute myocardial infarction, treated with Lisinopril tablet, had a higher (9.0% versus
3.7%) incidence of persistent hypotension (systolic blood pressure <90 mmHg for more than 1 hour)
and renal dysfunction (2.4% versus 1.1%) in-hospital and at six weeks (increasing creatinine
concentration to over 3 mg/dL or a doubling or more of the baseline serum creatinine concentration).
See ADVERSE REACTIONS - Acute Myocardial Infarction.
Pharmacokinetics
Pharmacokinetics and Metabolism
Adult Patients: Following oral administration of Lisinopril tablet, peak serum concentrations of lisinopril
Following oral administration of Lisinopril tablet, peak serum concentrations of lisinopril
occur within about 7 hours, although there was a trend to a small delay in time taken to reach peak
serum concentrations in acute myocardial infarction patients. Declining serum concentrations exhibit a
prolonged terminal phase which does not contribute to drug accumulation. This terminal phase
probably represents saturable binding to ACE and is not proportional to dose.
Lisinopril does not appear to be bound to other serum proteins. Lisinopril does not undergo metabolism
and is excreted unchanged entirely in the urine. Based on urinary recovery, the mean extent of
absorption of lisinopril is approximately 25%, with large intersubject variability (6%-60%) at all doses
tested (5-80 mg). Lisinopril absorption is not influenced by the presence of food in the gastrointestinal
tract. The absolute bioavailability of lisinopril is reduced to 16% in patients with stable NYHA Class IIIV
congestive heart failure, and the volume of distribution appears to be slightly smaller than that in
normal subjects. The oral bioavailability of lisinopril in patients with acute myocardial infarction is
similar to that in healthy volunteers.
Upon multiple dosing, lisinopril exhibits an effective half-life of accumulation of 12 hours.
Impaired renal function decreases elimination of lisinopril, which is excreted principally through the
kidneys, but this decrease becomes clinically important only when the glomerular filtration rate is below
30 mL/min. Above this glomerular filtration rate, the elimination half-life is little changed. With greater
impairment, however, peak and trough lisinopril levels increase, time to peak concentration increases
and time to attain steady state is prolonged. Older patients, on average, have (approximately doubled)
higher blood levels and area under the plasma concentration time curve (AUC) than younger patients.
(See DOSAGE AND ADMINISTRATION.) Lisinopril can be removed by hemodialysis.
Studies in rats indicate that lisinopril crosses the blood-brain barrier poorly. Multiple doses of lisinopril
in rats do not result in accumulation in any tissues. Milk of lactating rats contains radioactivity following
administration of 14C lisinopril. By whole body autoradiography, radioactivity was found in the placenta
following administration of labeled drug to pregnant rats, but none was found in the fetuses.
Pediatric Patients: The pharmacokinetics of lisinopril were studied in 29 pediatric hypertensive patients
The pharmacokinetics of lisinopril were studied in 29 pediatric hypertensive patients
between 6 years and 16 years with glomerular filtration rate >30 mL/min/1.73 m2. After doses of 0.1 to
0.2 mg/kg, steady state peak plasma concentrations of lisinopril occurred within 6 hours and the extent
of absorption based on urinary recovery was about 28%. These values are similar to those obtained
previously in adults. The typical value of lisinopril oral clearance (systemic clearance/absolute
bioavailability) in a child weighing 30 kg is 10 L/h, which increases in proportion to renal function.
INDICATIONS AND USAGE
Hypertension
Lisinopril tablet is indicated for the treatment of hypertension. It may be used alone as initial therapy or
concomitantly with other classes of antihypertensive agents.
Heart Failure
Lisinopril tablet is indicated as adjunctive therapy in the management of heart failure in patients who
are not responding adequately to diuretics and digitalis.
Acute Myocardial Infarction
Lisinopril tablet is indicated for the treatment of hemodynamically stable patients within 24 hours of
acute myocardial infarction, to improve survival. Patients should receive, as appropriate, the standard
recommended treatments such as thrombolytics, aspirin and beta blockers.
In using Lisinopril tablet, consideration should be given to the fact that another angiotensin-converting
enzyme inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment
or collagen vascular disease, and that available data are insufficient to show that Lisinopril tablet does
not have a similar risk. (See WARNINGS.)
In considering the use of Lisinopril tablet, it should be noted that in controlled clinical trials ACE
inhibitors have an effect on blood pressure that is less in Black patients than in non-Blacks. In addition,
ACE inhibitors have been associated with a higher rate of angioedema in Black than in non-Black
patients (see WARNINGS, Anaphylactoid and Possibly Related Reactions).
CONTRAINDICATIONS
Lisinopril tablet is contraindicated in patients who are hypersensitive to this product and in patients with
a history of angioedema related to previous treatment with an angiotensin converting enzyme inhibitor
and in patients with hereditary or idiopathic angioedema.
WARNINGS
Anaphylactoid and Possibly Related Reactions
Presumably because angiotensin-converting enzyme inhibitors affect the metabolism of eicosanoids
and polypeptides, including endogenous bradykinin, patients receiving ACE inhibitors (including
Lisinopril tablet) may be subject to a variety of adverse reactions, some of them serious.
Head and Neck Angioedema: Angioedema of the face, extremities, lips, tongue, glottis and/or larynx
Angioedema of the face, extremities, lips, tongue, glottis and/or larynx
has been reported in patients treated with angiotensin converting enzyme inhibitors, including Lisinopril
tablet. This may occur at any time during treatment. ACE inhibitors have been associated with a higher
rate of angioedema in Black than in non-Black patients. Lisinopril tablet should be promptly
discontinued and appropriate therapy and monitoring should be provided until complete and sustained
resolution of signs and symptoms has occurred. Even in those instances where swelling of only the
tongue is involved, without respiratory distress, patients may require prolonged observation since
treatment with antihistamines and corticosteroids may not be sufficient. Very rarely, fatalities have
been reported due to angioedema associated with laryngeal edema or tongue edema. Patients with
involvement of the tongue, glottis or larynx are likely to experience airway obstruction, especially those
with a history of airway surgery. Where there is involvement of the tongue, glottis or larynx, likely
to cause airway obstruction, appropriate therapy, e.g., subcutaneous epinephrine solution
1:1000 (0.3 mL to 0.5 mL) and/or measures necessary to ensure a patent airway should be
promptly provided. (See ADVERSE REACTIONS.)
Intestinal angioedema: Intestinal angioedema has been reported in patients treated with ACE
to cause airway obstruction, appropriate therapy, e.g., subcutaneous epinephrine solution
1:1000 (0.3 mL to 0.5 mL) and/or measures necessary to ensure a patent airway should be
promptly provided. (See ADVERSE REACTIONS.)
Intestinal angioedema: Intestinal angioedema has been reported in patients treated with ACE
inhibitors. These patients presented with abdominal pain (with or without nausea or vomiting); in some
cases there was no prior history of facial angioedema and C-1 esterase levels were normal. The
angioedema was diagnosed by procedures including abdominal CT scan or ultrasound, or at surgery,
and symptoms resolved after stopping the ACE inhibitor. Intestinal angioedema should be included in
the differential diagnosis of patients on ACE inhibitors presenting with abdominal pain.
Patients with a history of angioedema unrelated to ACE inhibitor therapy may be at increased risk of
angioedema while receiving an ACE inhibitor (see also INDICATIONS AND USAGE and
CONTRAINDICATIONS).
Anaphylactoid Reactions During Desensitization: Two patients undergoing desensitizing treatment
Two patients undergoing desensitizing treatment
with hymenoptera venom while receiving ACE inhibitors sustained life threatening anaphylactoid
reactions. In the same patients, these reactions were avoided when ACE inhibitors were temporarily
withheld, but they reappeared upon inadvertent rechallenge.
Anaphylactoid Reactions During Membrane Exposure: Sudden and potentially life threatening
Sudden and potentially life threatening
anaphylactoid reactions have been reported in some patients dialyzed with high-flux membranes (e.g.,
AN69®*) and treated concomitantly with an ACE inhibitor. In such patients, dialysis must be stopped
immediately, and aggressive therapy for anaphylactoid reactions must be initiated. Symptoms have not
been relieved by antihistamines in these situations. In these patients, consideration should be given to
using a different type of dialysis membrane or a different class of antihypertensive agent.
Anaphylactoid reactions have also been reported in patients undergoing low-density lipoprotein
apheresis with dextran sulfate absorption.
Hypotension
Excessive hypotension is rare in patients with uncomplicated hypertension treated with Lisinopril tablet
alone.
Patients with heart failure given Lisinopril tablet commonly have some reduction in blood pressure, with
peak blood pressure reduction occurring 6 to 8 hours post dose. Evidence from the two-dose ATLAS
trial suggested that incidence of hypotension may increase with dose of lisinopril in heart failure
patients. Discontinuation of therapy because of continuing symptomatic hypotension usually is not
necessary when dosing instructions are followed; caution should be observed when initiating therapy.
(See DOSAGE AND ADMINISTRATION.)
Patients at risk of excessive hypotension, sometimes associated with oliguria and/or progressive
azotemia, and rarely with acute renal failure and/or death, include those with the following conditions or
characteristics: heart failure with systolic blood pressure below 100 mmHg, hyponatremia, high dose
diuretic therapy, recent intensive diuresis or increase in diuretic dose, renal dialysis, or severe volume
and/or salt depletion of any etiology. It may be advisable to eliminate the diuretic (except in patients
with heart failure), reduce the diuretic dose or increase salt intake cautiously before initiating therapy
with Lisinopril tablet in patients at risk for excessive hypotension who are able to tolerate such
adjustments. (See PRECAUTIONS, Drug Interactions and ADVERSE REACTIONS.)
Patients with acute myocardial infarction in the GISSI-3 trial had a higher (9.0% versus 3.7%)
incidence of persistent hypotension (systolic blood pressure <90 mmHg for more than 1 hour) when
treated with Lisinopril tablet. Treatment with Lisinopril tablet must not be initiated in acute myocardial
infarction patients at risk of further serious hemodynamic deterioration after treatment with a
vasodilator (e.g., systolic blood pressure of 100 mmHg or lower) or cardiogenic shock.
In patients at risk of excessive hypotension, therapy should be started under very close medical
supervision and such patients should be followed closely for the first two weeks of treatment and
whenever the dose of Lisinopril tablet and/or diuretic is increased. Similar considerations may apply to
patients with ischemic heart or cerebrovascular disease, or in patients with acute myocardial infarction,
in whom an excessive fall in blood pressure could result in a myocardial infarction or cerebrovascular
accident.
If excessive hypotension occurs, the patient should be placed in the supine position and, if necessary,
receive an intravenous infusion of normal saline. A transient hypotensive response is not a
contraindication to further doses of Lisinopril tablet which usually can be given without difficulty once
the blood pressure has stabilized. If symptomatic hypotension develops, a dose reduction or
discontinuation of Lisinopril tablet or concomitant diuretic may be necessary.
Leukopenia/Neutropenia/Agranulocytosis
Another angiotensin converting enzyme inhibitor, captopril, has been shown to cause agranulocytosis
and bone marrow depression, rarely in uncomplicated patients but more frequently in patients with
renal impairment especially if they also have a collagen vascular disease. Available data from clinical
trials of Lisinopril tablet are insufficient to show that Lisinopril tablet does not cause agranulocytosis at
similar rates. Marketing experience has revealed rare cases of leukopenia/neutropenia and bone
marrow depression in which a causal relationship to lisinopril cannot be excluded. Periodic monitoring
of white blood cell counts in patients with collagen vascular disease and renal disease should be
considered.
Hepatic Failure
Rarely, ACE inhibitors have been associated with a syndrome that starts with cholestatic jaundice or
hepatitis and progresses to fulminant hepatic necrosis and (sometimes) death. The mechanism of this
syndrome is not understood. Patients receiving ACE inhibitors who develop jaundice or marked
elevations of hepatic enzymes should discontinue the ACE inhibitor and receive appropriate medical
follow-up.
Fetal/Neonatal Morbidity and Mortality
ACE inhibitors can cause fetal and neonatal morbidity and death when administered to pregnant
women. Several dozen cases have been reported in the world literature. When pregnancy is detected,
ACE inhibitors should be discontinued as soon as possible.
In a published retrospective epidemiological study, infants whose mothers had taken an ACE inhibitor
drug during their first trimester of pregnancy appeared to have an increased risk of major congenital
malformations compared with infants whose mothers had not undergone first trimester exposure to
ACE inhibitor drugs. The number of cases of birth defects is small and the findings of this study have
not yet been repeated.
The use of ACE inhibitors during the second and third trimesters of pregnancy has been associated
with fetal and neonatal injury, including hypotension, neonatal skull hypoplasia, anuria, reversible or
irreversible renal failure, and death. Oligohydramnios has also been reported, presumably resulting
from decreased fetal renal function; oligohydramnios in this setting has been associated with fetal limb
contractures, craniofacial deformation, and hypoplastic lung development. Prematurity, intrauterine
growth retardation, and patent ductus arteriosus have also been reported, although it is not clear
whether these occurrences were due to the ACE-inhibitor exposure.
These adverse effects do not appear to have resulted from intrauterine ACE-inhibitor exposure that
has been limited to the first trimester. Mothers whose embryos and fetuses are exposed to ACE
inhibitors only during the first trimester should be so informed. Nonetheless, when patients become
pregnant, physicians should make every effort to discontinue the use of Lisinopril tablet as soon as
possible.
Rarely (probably less often than once in every thousand pregnancies), no alternative to ACE inhibitors
will be found. In these rare cases, the mothers should be apprised of the potential hazards to their
fetuses, and serial ultrasound examinations should be performed to assess the intraamniotic
environment.
If oligohydramnios is observed, Lisinopril tablet should be discontinued unless it is considered
lifesaving for the mother. Contraction stress testing (CST), a nonstress test (NST), or biophysical
profiling (BPP) may be appropriate, depending upon the week of pregnancy. Patients and physicians
should be aware, however, that oligohydramnios may not appear until after the fetus has sustained
irreversible injury.
Infants with histories of in utero exposure to ACE inhibitors should be closely observed for
hypotension, oliguria, and hyperkalemia. If oliguria occurs, attention should be directed toward support
of blood pressure and renal perfusion. Exchange transfusion or dialysis may be required as means of
reversing hypotension and/or substituting for disordered renal function. Lisinopril, which crosses the
placenta, has been removed from neonatal circulation by peritoneal dialysis with some clinical benefit,
and theoretically may be removed by exchange transfusion, although there is no experience with the
latter procedure.
No teratogenic effects of lisinopril were seen in studies of pregnant rats, mice, and rabbits. On a mg/kg
basis, the doses used were up to 625 times (in mice), 188 times (in rats), and 0.6 times (in rabbits) the
maximum recommended human dose.
WARNINGS
Anaphylactoid and Possibly Related Reactions
Presumably because angiotensin-converting enzyme inhibitors affect the metabolism of eicosanoids
and polypeptides, including endogenous bradykinin, patients receiving ACE inhibitors (including
Lisinopril tablet) may be subject to a variety of adverse reactions, some of them serious.
Head and Neck Angioedema: Angioedema of the face, extremities, lips, tongue, glottis and/or larynx
Angioedema of the face, extremities, lips, tongue, glottis and/or larynx
has been reported in patients treated with angiotensin converting enzyme inhibitors, including Lisinopril
tablet. This may occur at any time during treatment. ACE inhibitors have been associated with a higher
rate of angioedema in Black than in non-Black patients. Lisinopril tablet should be promptly
discontinued and appropriate therapy and monitoring should be provided until complete and sustained
resolution of signs and symptoms has occurred. Even in those instances where swelling of only the
tongue is involved, without respiratory distress, patients may require prolonged observation since
treatment with antihistamines and corticosteroids may not be sufficient. Very rarely, fatalities have
been reported due to angioedema associated with laryngeal edema or tongue edema. Patients with
involvement of the tongue, glottis or larynx are likely to experience airway obstruction, especially those
with a history of airway surgery. Where there is involvement of the tongue, glottis or larynx, likely
to cause airway obstruction, appropriate therapy, e.g., subcutaneous epinephrine solution
1:1000 (0.3 mL to 0.5 mL) and/or measures necessary to ensure a patent airway should be
promptly provided. (See ADVERSE REACTIONS.)
Intestinal angioedema: Intestinal angioedema has been reported in patients treated with ACE
to cause airway obstruction, appropriate therapy, e.g., subcutaneous epinephrine solution
1:1000 (0.3 mL to 0.5 mL) and/or measures necessary to ensure a patent airway should be
promptly provided. (See ADVERSE REACTIONS.)
Intestinal angioedema: Intestinal angioedema has been reported in patients treated with ACE
inhibitors. These patients presented with abdominal pain (with or without nausea or vomiting); in some
cases there was no prior history of facial angioedema and C-1 esterase levels were normal. The
angioedema was diagnosed by procedures including abdominal CT scan or ultrasound, or at surgery,
and symptoms resolved after stopping the ACE inhibitor. Intestinal angioedema should be included in
the differential diagnosis of patients on ACE inhibitors presenting with abdominal pain.
Patients with a history of angioedema unrelated to ACE inhibitor therapy may be at increased risk of
angioedema while receiving an ACE inhibitor (see also INDICATIONS AND USAGE and
CONTRAINDICATIONS).
Anaphylactoid Reactions During Desensitization: Two patients undergoing desensitizing treatment
Two patients undergoing desensitizing treatment
with hymenoptera venom while receiving ACE inhibitors sustained life threatening anaphylactoid
reactions. In the same patients, these reactions were avoided when ACE inhibitors were temporarily
withheld, but they reappeared upon inadvertent rechallenge.
Anaphylactoid Reactions During Membrane Exposure: Sudden and potentially life threatening
Sudden and potentially life threatening
anaphylactoid reactions have been reported in some patients dialyzed with high-flux membranes (e.g.,
AN69®*) and treated concomitantly with an ACE inhibitor. In such patients, dialysis must be stopped
immediately, and aggressive therapy for anaphylactoid reactions must be initiated. Symptoms have not
been relieved by antihistamines in these situations. In these patients, consideration should be given to
using a different type of dialysis membrane or a different class of antihypertensive agent.
Anaphylactoid reactions have also been reported in patients undergoing low-density lipoprotein
apheresis with dextran sulfate absorption.
Hypotension
Excessive hypotension is rare in patients with uncomplicated hypertension treated with Lisinopril tablet
alone.
Patients with heart failure given Lisinopril tablet commonly have some reduction in blood pressure, with
peak blood pressure reduction occurring 6 to 8 hours post dose. Evidence from the two-dose ATLAS
trial suggested that incidence of hypotension may increase with dose of lisinopril in heart failure
patients. Discontinuation of therapy because of continuing symptomatic hypotension usually is not
necessary when dosing instructions are followed; caution should be observed when initiating therapy.
(See DOSAGE AND ADMINISTRATION.)
Patients at risk of excessive hypotension, sometimes associated with oliguria and/or progressive
azotemia, and rarely with acute renal failure and/or death, include those with the following conditions or
characteristics: heart failure with systolic blood pressure below 100 mmHg, hyponatremia, high dose
diuretic therapy, recent intensive diuresis or increase in diuretic dose, renal dialysis, or severe volume
and/or salt depletion of any etiology. It may be advisable to eliminate the diuretic (except in patients
with heart failure), reduce the diuretic dose or increase salt intake cautiously before initiating therapy
with Lisinopril tablet in patients at risk for excessive hypotension who are able to tolerate such
adjustments. (See PRECAUTIONS, Drug Interactions and ADVERSE REACTIONS.)
Patients with acute myocardial infarction in the GISSI-3 trial had a higher (9.0% versus 3.7%)
incidence of persistent hypotension (systolic blood pressure <90 mmHg for more than 1 hour) when
treated with Lisinopril tablet. Treatment with Lisinopril tablet must not be initiated in acute myocardial
infarction patients at risk of further serious hemodynamic deterioration after treatment with a
vasodilator (e.g., systolic blood pressure of 100 mmHg or lower) or cardiogenic shock.
In patients at risk of excessive hypotension, therapy should be started under very close medical
supervision and such patients should be followed closely for the first two weeks of treatment and
whenever the dose of Lisinopril tablet and/or diuretic is increased. Similar considerations may apply to
patients with ischemic heart or cerebrovascular disease, or in patients with acute myocardial infarction,
in whom an excessive fall in blood pressure could result in a myocardial infarction or cerebrovascular
accident.
If excessive hypotension occurs, the patient should be placed in the supine position and, if necessary,
receive an intravenous infusion of normal saline. A transient hypotensive response is not a
contraindication to further doses of Lisinopril tablet which usually can be given without difficulty once
the blood pressure has stabilized. If symptomatic hypotension develops, a dose reduction or
discontinuation of Lisinopril tablet or concomitant diuretic may be necessary.
Leukopenia/Neutropenia/Agranulocytosis
Another angiotensin converting enzyme inhibitor, captopril, has been shown to cause agranulocytosis
and bone marrow depression, rarely in uncomplicated patients but more frequently in patients with
renal impairment especially if they also have a collagen vascular disease. Available data from clinical
trials of Lisinopril tablet are insufficient to show that Lisinopril tablet does not cause agranulocytosis at
similar rates. Marketing experience has revealed rare cases of leukopenia/neutropenia and bone
marrow depression in which a causal relationship to lisinopril cannot be excluded. Periodic monitoring
of white blood cell counts in patients with collagen vascular disease and renal disease should be
considered.
Hepatic Failure
Rarely, ACE inhibitors have been associated with a syndrome that starts with cholestatic jaundice or
hepatitis and progresses to fulminant hepatic necrosis and (sometimes) death. The mechanism of this
syndrome is not understood. Patients receiving ACE inhibitors who develop jaundice or marked
elevations of hepatic enzymes should discontinue the ACE inhibitor and receive appropriate medical
follow-up.
Fetal/Neonatal Morbidity and Mortality
ACE inhibitors can cause fetal and neonatal morbidity and death when administered to pregnant
women. Several dozen cases have been reported in the world literature. When pregnancy is detected,
ACE inhibitors should be discontinued as soon as possible.
In a published retrospective epidemiological study, infants whose mothers had taken an ACE inhibitor
drug during their first trimester of pregnancy appeared to have an increased risk of major congenital
malformations compared with infants whose mothers had not undergone first trimester exposure to
ACE inhibitor drugs. The number of cases of birth defects is small and the findings of this study have
not yet been repeated.
The use of ACE inhibitors during the second and third trimesters of pregnancy has been associated
with fetal and neonatal injury, including hypotension, neonatal skull hypoplasia, anuria, reversible
or irreversible renal failure, and death. Oligohydramnios has also been reported, presumably resulting
from decreased fetal renal function; oligohydramnios in this setting has been associated with fetal limb
contractures, craniofacial deformation, and hypoplastic lung development. Prematurity, intrauterine
growth retardation, and patent ductus arteriosus have also been reported, although it is not clear
whether these occurrences were due to the ACE-inhibitor exposure.
These adverse effects do not appear to have resulted from intrauterine ACE-inhibitor exposure that
has been limited to the first trimester. Mothers whose embryos and fetuses are exposed to ACE
inhibitors only during the first trimester should be so informed. Nonetheless, when patients become
pregnant, physicians should make every effort to discontinue the use of Lisinopril tablet as soon as
possible.
Rarely (probably less often than once in every thousand pregnancies), no alternative to ACE inhibitors
will be found. In these rare cases, the mothers should be apprised of the potential hazards to their
fetuses, and serial ultrasound examinations should be performed to assess the intraamniotic
environment.
If oligohydramnios is observed, Lisinopril tablet should be discontinued unless it is considered
lifesaving for the mother. Contraction stress testing (CST), a nonstress test (NST), or biophysical
profiling (BPP) may be appropriate, depending upon the week of pregnancy. Patients and physicians
should be aware, however, that oligohydramnios may not appear until after the fetus has sustained
irreversible injury.
Infants with histories of in utero exposure to ACE inhibitors should be closely observed for
hypotension, oliguria, and hyperkalemia. If oliguria occurs, attention should be directed toward support
of blood pressure and renal perfusion. Exchange transfusion or dialysis may be required as means of
reversing hypotension and/or substituting for disordered renal function. Lisinopril, which crosses the
placenta, has been removed from neonatal circulation by peritoneal dialysis with some clinical benefit,
and theoretically may be removed by exchange transfusion, although there is no experience with the
latter procedure.
No teratogenic effects of lisinopril were seen in studies of pregnant rats, mice, and rabbits. On a mg/kg
basis, the doses used were up to 625 times (in mice), 188 times (in rats), and 0.6 times (in rabbits) the
maximum recommended human dose.
PRECAUTIONS
General
Aortic Stenosis/Hypertrophic Cardiomyopathy: As with all vasodilators, lisinopril should be given
As with all vasodilators, lisinopril should be given
with caution to patients with obstruction in the outflow tract of the left ventricle.
Impaired Renal Function: As a consequence of inhibiting the renin-angiotensin-aldosterone system,
As a consequence of inhibiting the renin-angiotensin-aldosterone system,
changes in renal function may be anticipated in susceptible individuals. In patients with severe
congestive heart failure whose renal function may depend on the activity of the renin-angiotensinaldosterone
system, treatment with angiotensin converting enzyme inhibitors, including Lisinopril
tablet, may be associated with oliguria and/or progressive azotemia and rarely with acute renal failure
and/or death.
In hypertensive patients with unilateral or bilateral renal artery stenosis, increases in blood urea
nitrogen and serum creatinine may occur. Experience with another angiotensin-converting enzyme
inhibitor suggests that these increases are usually reversible upon discontinuation of Lisinopril tablet
and/or diuretic therapy. In such patients, renal function should be monitored during the first few weeks
of therapy.
Some patients with hypertension or heart failure with no apparent pre-existing renal vascular disease
have developed increases in blood urea nitrogen and serum creatinine, usually minor and transient,
especially when Lisinopril tablet has been given concomitantly with a diuretic. This is more likely to
occur in patients with pre-existing renal impairment. Dosage reduction and/or discontinuation of the
diuretic and/or Lisinopril tablet may be required.
Patients with acute myocardial infarction in the GISSI-3 trial treated with Lisinopril tablet had a higher
(2.4% versus 1.1%) incidence of renal dysfunction in-hospital and at six weeks (increasing creatinine
concentration to over 3 mg/dL or a doubling or more of the baseline serum creatinine concentration). In
acute myocardial infarction, treatment with Lisinopril tablet should be initiated with caution in patients
with evidence of renal dysfunction, defined as serum creatinine concentration exceeding 2 mg/dL. If
renal dysfunction develops during treatment with Lisinopril tablet (serum creatinine concentration
exceeding 3 mg/dL or a doubling from the pre-treatment value) then the physician should consider
withdrawal of Lisinopril tablet.
Evaluation of patients with hypertension, heart failure, or myocardial infarction should always
include assessment of renal function. (See DOSAGE AND ADMINISTRATION.)
Hyperkalemia: In clinical trials hyperkalemia (serum potassium greater than 5.7 mEq/L) occurred in
In clinical trials hyperkalemia (serum potassium greater than 5.7 mEq/L) occurred in
approximately 2.2% of hypertensive patients and 4.8% of patients with heart failure. In most cases
these were isolated values which resolved despite continued therapy. Hyperkalemia was a cause of
discontinuation of therapy in approximately 0.1% of hypertensive patients; 0.6% of patients with heart
failure and 0.1% of patients with myocardial infarction. Risk factors for the development of
hyperkalemia include renal insufficiency, diabetes mellitus, and the concomitant use of potassiumsparing
diuretics, potassium supplements and/or potassium-containing salt substitutes. Hyperkalemia
can cause serious, sometimes fatal, arrhythmias. Lisinopril tablet should be used cautiously, if at all,
with these agents and with frequent monitoring of serum potassium. (See Drug Interactions.)
Hypoglycemia: Diabetic patients treated with oral antidiabetic agents or insulin starting an ACE
Diabetic patients treated with oral antidiabetic agents or insulin starting an ACE
inhibitor should be told to closely monitor for hypoglycemia, especially during the first month of
combined use. (See PRECAUTIONS, Drug Interactions.)
Antidiabetics: Epidemiological studies have suggested that concomitant administration of ACE
Epidemiological studies have suggested that concomitant administration of ACE
inhibitors and antidiabetic medicines (insulins, oral hypoglycemic agents) may cause an increased
blood-glucose-lowering effect with risk of hypoglycemia. This phenomenon appeared to be more likely
to occur during the first weeks of combined treatment and in patients with renal impairment. In diabetic
patients treated with oral antidiabetic agents or insulin, glycemic control should be closely monitored
for hypoglycemia, especially during the first month of treatment with an ACE inhibitor.
Cough: Presumably due to the inhibition of the degradation of endogenous bradykinin, persistent
Presumably due to the inhibition of the degradation of endogenous bradykinin, persistent
nonproductive cough has been reported with all ACE inhibitors, almost always resolving after
discontinuation of therapy. ACE inhibitor induced cough should be considered in the differential
diagnosis of cough.
Surgery/Anesthesia: In patients undergoing major surgery or during anesthesia with agents that
In patients undergoing major surgery or during anesthesia with agents that
produce hypotension, Lisinopril tablet may block angiotensin II formation secondary to compensatory
renin release. If hypotension occurs and is considered to be due to this mechanism, it can be corrected
by volume expansion.
Information for Patients
Angioedema: Angioedema, including laryngeal edema, may occur at any time during treatment with
Angioedema, including laryngeal edema, may occur at any time during treatment with
angiotensin-converting enzyme inhibitors, including Lisinopril tablet. Patients should be so advised and
told to report immediately any signs or symptoms suggesting angioedema (swelling of face,
extremities, eyes, lips, tongue, difficulty in swallowing or breathing) and to take no more drug until they
have consulted with the prescribing physician.
Symptomatic Hypotension: Patients should be cautioned to report lightheadedness especially during
Patients should be cautioned to report lightheadedness especially during
the first few days of therapy. If actual syncope occurs, the patient should be told to discontinue the
drug until they have consulted with the prescribing physician.
All patients should be cautioned that excessive perspiration and dehydration may lead to an excessive
fall in blood pressure because of reduction in fluid volume. Other causes of volume depletion such as
vomiting or diarrhea may also lead to a fall in blood pressure; patients should be advised to consult
with their physician.
Hyperkalemia: Patients should be told not to use salt substitutes containing potassium without
Patients should be told not to use salt substitutes containing potassium without
consulting their physician.
Leukopenia/Neutropenia: Patients should be told to report promptly any indication of infection (e.g.,
Patients should be told to report promptly any indication of infection (e.g.,
sore throat, fever) which may be a sign of leukopenia/neutropenia.
Pregnancy: Female patients of childbearing age should be told about the consequences of exposure
Female patients of childbearing age should be told about the consequences of exposure
to ACE inhibitors during pregnancy. These patients should be asked to report pregnancies to their
physicians as soon as possible.
NOTE: As with many other drugs, certain advice to patients being treated with Lisinopril tablet is
As with many other drugs, certain advice to patients being treated with Lisinopril tablet is
warranted. This information is intended to aid in the safe and effective use of this medication. It is not a
disclosure of all possible adverse or intended effects.
Information for Patients
Information for Patients
Angioedema: Angioedema, including laryngeal edema, may occur at any time during treatment with
Angioedema, including laryngeal edema, may occur at any time during treatment with
angiotensin-converting enzyme inhibitors, including Lisinopril tablet. Patients should be so advised and
told to report immediately any signs or symptoms suggesting angioedema (swelling of face,
extremities, eyes, lips, tongue, difficulty in swallowing or breathing) and to take no more drug until they
have consulted with the prescribing physician.
Symptomatic Hypotension: Patients should be cautioned to report lightheadedness especially during
Patients should be cautioned to report lightheadedness especially during
the first few days of therapy. If actual syncope occurs, the patient should be told to discontinue the
drug until they have consulted with the prescribing physician.
All patients should be cautioned that excessive perspiration and dehydration may lead to an excessive
fall in blood pressure because of reduction in fluid volume. Other causes of volume depletion such as
vomiting or diarrhea may also lead to a fall in blood pressure; patients should be advised to consult
with their physician.
Hyperkalemia: Patients should be told not to use salt substitutes containing potassium without
Patients should be told not to use salt substitutes containing potassium without
consulting their physician.
Leukopenia/Neutropenia: Patients should be told to report promptly any indication of infection (e.g.,
Patients should be told to report promptly any indication of infection (e.g.,
sore throat, fever) which may be a sign of leukopenia/neutropenia.
Pregnancy: Female patients of childbearing age should be told about the consequences of exposure
Female patients of childbearing age should be told about the consequences of exposure
to ACE inhibitors during pregnancy. These patients should be asked to report pregnancies to their
physicians as soon as possible.
NOTE: As with many other drugs, certain advice to patients being treated with Lisinopril tablet is
As with many other drugs, certain advice to patients being treated with Lisinopril tablet is
warranted. This information is intended to aid in the safe and effective use of this medication. It is not a
disclosure of all possible adverse or intended effects.
Drug Interactions
Hypotension - Patients on Diuretic Therapy: Patients on diuretics and especially those in whom
Patients on diuretics and especially those in whom
diuretic therapy was recently instituted, may occasionally experience an excessive reduction of blood
pressure after initiation of therapy with Lisinopril tablet. The possibility of hypotensive effects with
Lisinopril tablet can be minimized by either discontinuing the diuretic or increasing the salt intake prior
to initiation of treatment with Lisinopril tablet. If it is necessary to continue the diuretic, initiate therapy
with Lisinopril tablet at a dose of 5 mg daily, and provide close medical supervision after the initial dose
until blood pressure has stabilized. (See WARNINGS, and DOSAGE AND ADMINISTRATION.) When
a diuretic is added to the therapy of a patient receiving Lisinopril tablet, an additional antihypertensive
effect is usually observed. Studies with ACE inhibitors in combination with diuretics indicate that the
dose of the ACE inhibitor can be reduced when it is given with a diuretic. (See DOSAGE AND
ADMINISTRATION.)
Non-steroidal Anti-inflammatory Agents: In some patients with comprised renal function who are
In some patients with comprised renal function who are
being treated with non-steroidal anti-inflammatory drugs, the co-administration of lisinopril may result in
further deterioration of renal function. These effects are usually reversible. In a study in 36 patients
with mild to moderate hypertension where the antihypertensive effects of Lisinopril tablet alone were
compared to Lisinopril tablet given concomitantly with indomethacin, the use of indomethacin was
associated with a reduced effect, although the difference between the two regimens was not
significant.
Other Agents: Lisinopril tablet has been used concomitantly with nitrates and/or digoxin without
Lisinopril tablet has been used concomitantly with nitrates and/or digoxin without
evidence of clinically significant adverse interactions. This included post myocardial infarction patients
who were receiving intravenous or transdermal nitroglycerin. No clinically important pharmacokinetic
interactions occurred when Lisinopril tablet was used concomitantly with propranolol or
hydrochlorothiazide. The presence of food in the stomach does not alter the bioavailability of Lisinopril
tablet.
Agents Increasing Serum Potassium: Lisinopril tablet attenuates potassium loss caused by thiazidetype
Lisinopril tablet attenuates potassium loss caused by thiazidetype
diuretics. Use of Lisinopril tablet with potassium-sparing diuretics (e.g., spironolactone,
triamterene or amiloride, eplerenone), potassium supplements, or potassium-containing salt
substitutes may lead to significant increases in serum potassium. Therefore, if concomitant use of
these agents is indicated because of demonstrated hypokalemia, they should be used with caution and
with frequent monitoring of serum potassium. Potassium-sparing agents should generally not be used
in patients with heart failure who are receiving Lisinopril tablet.
Lithium: Lithium toxicity has been reported in patients receiving lithium concomitantly with drugs which
Lithium toxicity has been reported in patients receiving lithium concomitantly with drugs which
cause elimination of sodium, including ACE inhibitors. Lithium toxicity was usually reversible upon
discontinuation of lithium and the ACE inhibitor. It is recommended that serum lithium levels be
monitored frequently if Lisinopril tablet is administered concomitantly with lithium.
Gold: Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have
Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have
been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and
concomitant ACE inhibitor therapy including lisinopril.
Carcinogenesis, Mutagenesis, Impairment of Fertility
There was no evidence of a tumorigenic effect when lisinopril was administered for 105 weeks to male
and female rats at doses up to 90 mg/kg/day (about 56 or 9 times* the maximum recommended daily
human dose, based on body weight and body surface area, respectively). There was no evidence of
carcinogenicity when lisinopril was administered for 92 weeks to (male and female) mice at doses up
to 135 mg/kg/day (about 84 times* the maximum recommended daily human dose). This dose was 6.8
times the maximum human dose based on body surface area in mice.
*Calculations assume a human weight of 50 kg and human body surface area of 1.62 m2.
Calculations assume a human weight of 50 kg and human body surface area of 1.62 m2.
Lisinopril was not mutagenic in the Ames microbial mutagen test with or without metabolic activation. It
was also negative in a forward mutation assay using Chinese hamster lung cells. Lisinopril did not
produce single strand DNA breaks in an in vitro alkaline elution rat hepatocyte assay. In addition,
lisinopril did not produce increases in chromosomal aberrations in an in vitro test in Chinese hamster
ovary cells or in an in vivo study in mouse bone marrow.
There were no adverse effects on reproductive performance in male and female rats treated with up to
300 mg/kg/day of lisinopril. This dose is 188 times and 30 times the maximum human dose when
based on mg/kg and mg/m2, respectively.
Pregnancy
Pregnancy Categories C (first trimester) and D (second and third trimesters). See WARNINGS,
See WARNINGS,
Fetal/Neonatal Morbidity and Mortality.
Nursing Mothers
Milk of lactating rats contains radioactivity following administration of 14C lisinopril. It is not known
whether this drug is excreted in human milk. Because many drugs are excreted in human milk and
because of the potential for serious adverse reactions in nursing infants from ACE inhibitors, a decision
should be made whether to discontinue nursing or discontinue Lisinopril tablet, taking into account the
importance of the drug to the mother.
Pediatric Use
Antihypertensive effects of Lisinopril tablet have been established in hypertensive pediatric patients
aged 6 to 16 years.
There are no data on the effect of Lisinopril tablet on blood pressure in pediatric patients under the age
6 or in pediatric patients with glomerular filtration rate <30 mL/min/1.73 m2. (See CLINICAL
PHARMACOLOGY, Pharmacokinetics and Metabolism and Pharmacodynamics and Clinical Effects,
and DOSAGE AND ADMINISTRATION.)
Geriatric Use
Clinical studies of Lisinopril tablet in patients with hypertension did not include sufficient numbers of
subjects aged 65 and over to determine whether they respond differently from younger subjects. Other
clinical experience in this population has not identified differences in responses between the elderly
and younger patients. In general, dose selection for an elderly patient should be cautious, usually
starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic,
renal, or cardiac function, and of concomitant disease or other drug therapy.
In the ATLAS trial of Lisinopril tablet in patients with congestive heart failure, 1,596 (50%) were 65 and
over, while 437 (14%) were 75 and over. In a clinical study of Lisinopril tablet in patients with
myocardial infarctions 4,413 (47%) were 65 and over, while 1,656(18%) were 75 and over. In these
studies, no overall differences in safety or effectiveness were observed between elderly and younger
patients, and other reported clinical experiences has not identified differences in responses between
the elderly and younger patients (see CLINICAL PHARMACOLOGY – Pharmacodynamics and Clinical
Effects – Heart Failure and CLINICAL PHARMACOLOGY – Pharmacodynamics and Clinical Effects –
Acute Myocardial Infarction).
Other reported clinical experience has not identified differences in responses between elderly and
younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Pharmacokinetic studies indicate that maximum blood levels and area under the plasma concentration
time curve (AUC) are doubled in older patients (see CLINICAL PHARMACOLOGY – Pharmacokinetics
and Metabolism).
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this
drug may be greater in patients with impaired renal function. Because elderly patients are more likely
to have decreased renal function, care should be taken in dose selection. Evaluation of patients with
hypertension, congestive heart failure, or myocardial infarction should always include assessment of
renal function (see DOSAGE AND ADMINISTRATION).
ADVERSE REACTIONS
ADVERSE REACTIONS
Lisinopril tablet has been found to be generally well tolerated in controlled clinical trials involving 1969
patients with hypertension or heart failure. For the most part, adverse experiences were mild and
transient.
Hypertension
In clinical trials in patients with hypertension treated with Lisinopril tablet, discontinuation of therapy
due to clinical adverse experiences occurred in 5.7% of patients. The overall frequency of adverse
experiences could not be related to total daily dosage within the recommended therapeutic dosage
range.
For adverse experiences occurring in greater than 1% of patients with hypertension treated with
Lisinopril tablet or Lisinopril tablet plus hydrochlorothiazide in controlled clinical trials, and more
frequently with Lisinopril tablet and/or Lisinopril tablet plus hydrochlorothiazide than placebo,
comparative incidence data are listed in the table below:
PERCENT OF PATIENTS IN CONTROLLED STUDIES
Lisinopril tablet (n=1349) Incidence (discontinuation)
Lisinopril tablet/Hydrochlorothiazide (n=629) Incidence (discontinuation)
PLACEBO
(n=207) Incidence (discontinuation)
Body as a Whole
Fatigue 2.5 (0.3) 4.0 (0.5) 1.0 (0.0)
Asthenia 1.3 (0.5) 2.1 (0.2) 1.0 (0.0)
Orthostatic Effects 1.2 (0.0) 3.5 (0.2) 1.0 (0.0)
Cardiovascular
Hypotension 1.2 (0.5) 1.6 (0.5) 0.5 (0.5)
Digestive
Diarrhea 2.7 (0.2) 2.7 (0.3) 2.4 (0.0)
Nausea 2.0 (0.4) 2.5 (0.2) 2.4 (0.0)
Vomiting 1.1 (0.2) 1.4 (0.1) 0.5 (0.0)
Dyspepsia 0.9 (0.0) 1.9 (0.0) 0.0 (0.0)
Musculoskeletal
Muscle Cramps 0.5 (0.0) 2.9 (0.8) 0.5 (0.0)
Nervous/Psychiatric
Headache 5.7 (0.2) 4.5 (0.5) 1.9 (0.0)
Dizziness 5.4 (0.4) 9.2 (1.0) 1.9 (0.0)
Paresthesia 0.8 (0.1) 2.1 (0.2) 0.0 (0.0)
Decreased Libido 0.4 (0.1) 1.3 (0.1) 0.0 (0.0)
Vertigo 0.2 (0.1) 1.1 (0.2) 0.0 (0.0)
Respiratory
Cough 3.5 (0.7) 4.6 (0.8) 1.0 (0.0)
Upper Respiratory Infection 2.1 (0.1) 2.7 (0.1) 0.0 (0.0)
Common Cold 1.1 (0.1) 1.3 (0.1) 0.0 (0.0)
Nasal Congestion 0.4 (0.1) 1.3 (0.1) 0.0 (0.0)
Influenza 0.3 (0.1) 1.1 (0.1) 0.0 (0.0)
Skin
Rash 1.3 (0.4) 1.6 (0.2) 0.5 (0.5)
Urogenital
Impotence 1.0 (0.4) 1.6 (0.5) 0.0 (0.0)
Chest pain and back pain were also seen, but were more common on placebo than Lisinopril tablet.
Heart Failure
In patients with heart failure treated with Lisinopril tablet for up to four years, discontinuation of therapy
due to clinical adverse experiences occurred in 11.0% of patients. In controlled studies in patients with
heart failure, therapy was discontinued in 8.1% of patients treated with Lisinopril tablet for 12 weeks,
compared to 7.7% of patients treated with placebo for 12 weeks.
The following table lists those adverse experiences which occurred in greater than 1% of patients with
heart failure treated with Lisinopril tablet or placebo for up to 12 weeks in controlled clinical trials, and
more frequently on Lisinopril tablet than placebo.
Controlled Trials
Lisinopril tablet (n=407) Incidence (discontinuation)
12 weeks Placebo (n=155) Incidence (discontinuation)
12 weeks
Body as a Whole
Chest Pain 3.4 (0.2) 1.3 (0.0)
Abdominal Pain 2.2 (0.7) 1.9 (0.0)
Cardiovascular
Hypotension 4.4 (1.7) 0.6 (0.6)
Digestive
Diarrhea 3.7 (0.5) 1.9 (0.0)
Nervous/Psychiatric
Dizziness 11.8 (1.2) 4.5 (1.3)
Headache 4.4 (0.2) 3.9 (0.0)
Respiratory
Upper Respiratory Infection 1.5 (0.0) 1.3 (0.0)
Skin
Rash 1.7 (0.5) 0.6 (0.6)
Also observed at >1% with Lisinopril tablet but more frequent or as frequent on placebo than Lisinopril
tablet in controlled trials were asthenia, angina pectoris, nausea, dyspnea, cough, and pruritus.
Worsening of heart failure, anorexia, increased salivation, muscle cramps, back pain, myalgia,
depression, chest sound abnormalities, and pulmonary edema were also seen in controlled clinical
trials, but were more common on placebo than Lisinopril tablet.
In the two-dose ATLAS trial in heart failure patients, withdrawals due to adverse events were not
different between the low and high groups, either in total number of discontinuation (17-18%) or in rare
specific events (<1%). The following adverse events, mostly related to ACE inhibition, were reported
more commonly in the high dose group:
% of patients Events High Dose (N=1568)
Low dose (N=1596)
Dizziness 18.9 12.1
Hypotension 10.8 6.7
Creatinine increased 9.9 7.0
Hyperkalemia 6.4 3.5
NPN* increased 9.2 6.5
Syncope 7.0 5.1
*NPN = non-protein nitrogen
NPN = non-protein nitrogen
Acute Myocardial Infarction
In the GISSI-3 trial, in patients treated with Lisinopril tablet for six weeks following acute myocardial
infarction, discontinuation of therapy occurred in 17.6% of patients.
Patients treated with Lisinopril tablet had a significantly higher incidence of hypotension and renal
dysfunction compared with patients not taking Lisinopril tablet.
In the GISSI-3 trial, hypotension (9.7%), renal dysfunction (2.0%), cough (0.5%), post infarction angina
(0.3%), skin rash and generalized edema (0.01%), and angioedema (0.01%) resulted in withdrawal of
treatment. In elderly patients treated with Lisinopril tablet, discontinuation due to renal dysfunction was
4.2%.
Other clinical adverse experiences occurring in 0.3% to 1.0% of patients with hypertension or heart
failure treated with Lisinopril tablet in controlled clinical trials and rarer, serious, possibly drug-related
events reported in uncontrolled studies or marketing experience are listed below, and within each
category are in order of decreasing severity:
Body as a Whole: Anaphylactoid reactions (see WARNINGS, Anaphylactoid and Possibly Related
Anaphylactoid reactions (see WARNINGS, Anaphylactoid and Possibly Related
Reactions), syncope, orthostatic effects, chest discomfort, pain, pelvic pain, flank pain, edema, facial
edema, virus infection, fever, chills, malaise.
Cardiovascular: Cardiac arrest; myocardial infarction or cerebrovascular accident possibly secondary
Cardiac arrest; myocardial infarction or cerebrovascular accident possibly secondary
to excessive hypotension in high risk patients (see WARNINGS, Hypotension); pulmonary embolism
and infarction, arrhythmias (including ventricular tachycardia, atrial tachycardia, atrial fibrillation,
bradycardia and premature ventricular contractions), palpitations, transient ischemic attacks,
paroxysmal nocturnal dyspnea, orthostatic hypotension, decreased blood pressure, peripheral edema,
vasculitis.
Digestive: Pancreatitis, hepatitis (hepatocellular or cholestatic jaundice) (see WARNINGS, Hepatic
Pancreatitis, hepatitis (hepatocellular or cholestatic jaundice) (see WARNINGS, Hepatic
Failure), vomiting, gastritis, dyspepsia, heartburn, gastrointestinal cramps, constipation, flatulence, dry
mouth.
Hematologic: Rare cases of bone marrow depression, hemolytic anemia, leukopenia/ neutropenia
Rare cases of bone marrow depression, hemolytic anemia, leukopenia/ neutropenia
and thrombocytopenia.
Endocrine: Diabetes mellitus.
Diabetes mellitus.
Metabolic: Weight loss, dehydration, fluid overload, gout, weight gain. Cases of hypoglycemia in
Weight loss, dehydration, fluid overload, gout, weight gain. Cases of hypoglycemia in
diabetic patients on oral antidiabetic agents or insulin have been reported in post-marketing experience
(See PRECAUTIONS, Drug Interactions).
Musculoskeletal: Arthritis, arthralgia, neck pain, hip pain, low back pain, joint pain, leg pain, knee
Arthritis, arthralgia, neck pain, hip pain, low back pain, joint pain, leg pain, knee
pain, shoulder pain, arm pain, lumbago.
Nervous System/Psychiatric: Stroke, ataxia, memory impairment, tremor, peripheral neuropathy
Stroke, ataxia, memory impairment, tremor, peripheral neuropathy
(e.g., dysesthesia), spasm, paresthesia, confusion, insomnia, somnolence, hypersomnia, irritability and
nervousness.
Respiratory System: Malignant lung neoplasms, hemoptysis, pulmonary infiltrates, bronchospasm,
Malignant lung neoplasms, hemoptysis, pulmonary infiltrates, bronchospasm,
asthma, pleural effusion, pneumonia, eosinophilic pneumonitis, bronchitis, wheezing, orthopnea,
painful respiration, epistaxis, laryngitis, sinusitis, pharyngeal pain, pharyngitis, rhinitis, rhinorrhea.
Skin: Urticaria, alopecia, herpes zoster, photosensitivity, skin lesions, skin infections, pemphigus,
Urticaria, alopecia, herpes zoster, photosensitivity, skin lesions, skin infections, pemphigus,
erythema, flushing, diaphoresis, cutaneous pseudolymphoma. Other severe skin reactions have been
reported rarely, including toxic epidermal necrolysis and Stevens-Johnson syndrome; causal
relationship has not been established.
Special Senses: Visual loss, diplopia, blurred vision, tinnitus, photophobia, taste disturbances.
Visual loss, diplopia, blurred vision, tinnitus, photophobia, taste disturbances.
Urogenital System: Acute renal failure, oliguria, anuria, uremia, progressive azotemia, renal
Acute renal failure, oliguria, anuria, uremia, progressive azotemia, renal
dysfunction (see PRECAUTIONS and DOSAGE AND ADMINISTRATION), pyelonephritis, dysuria,
urinary tract infection, breast pain.
Miscellaneous: A symptom complex has been reported which may include a positive ANA, an
A symptom complex has been reported which may include a positive ANA, an
elevated erythrocyte sedimentation rate, arthralgia/arthritis, myalgia, fever, vasculitis, eosinophilia and
leukocytosis. Rash, photosensitivity or other dermatological manifestations may occur alone or in
combination with these symptoms.
Angioedema: Angioedema has been reported in patients receiving Lisinopril tablet (0.1%) with an
Angioedema has been reported in patients receiving Lisinopril tablet (0.1%) with an
incidence higher in Black than in non-Black patients. Angioedema associated with laryngeal edema
may be fatal. If angioedema of the face, extremities, lips, tongue, glottis and/or larynx occurs,
treatment with Lisinopril tablet should be discontinued and appropriate therapy instituted immediately.
(See WARNINGS.)
In rare cases, intestinal angioedema has been reported in post marketing experience.
Hypotension: In hypertensive patients, hypotension occurred in 1.2% and syncope occurred in 0.1%
In hypertensive patients, hypotension occurred in 1.2% and syncope occurred in 0.1%
of patients with an incidence higher in Black than in non-Black patients. Hypotension or syncope was a
cause of discontinuation of therapy in 0.5% of hypertensive patients. In patients with heart failure,
hypotension occurred in 5.3% and syncope occurred in 1.8% of patients. These adverse experiences
were possibly dose-related (see above data from ATLAS Trial) and caused discontinuation of therapy
in 1.8% of these patients in the symptomatic trials. In patients treated with Lisinopril tablet for six
weeks after acute myocardial infarction, hypotension (systolic blood pressure ≤100 mmHg) resulted in
discontinuation of therapy in 9.7% of the patients. (See WARNINGS.)
Fetal/Neonatal Morbidity and Mortality: See WARNINGS, Fetal/Neonatal Morbidity and Mortality.
See WARNINGS, Fetal/Neonatal Morbidity and Mortality.
Cough: See PRECAUTIONS – Cough
See PRECAUTIONS – Cough
Pediatric Patients: No relevant differences between the adverse experience profile for pediatric
No relevant differences between the adverse experience profile for pediatric
patients and that previously reported for adult patients were identified.
Clinical Laboratory Findings
Serum Electrolytes: Hyperkalemia (See PRECAUTIONS), hyponatremia.
Hyperkalemia (See PRECAUTIONS), hyponatremia.
Creatinine, Blood Urea Nitrogen: Minor increases in blood urea nitrogen and serum creatinine,
Minor increases in blood urea nitrogen and serum creatinine,
reversible upon discontinuation of therapy, were observed in about 2.0% of patients with essential
hypertension treated with Lisinopril tablet alone. Increases were more common in patients receiving
concomitant diuretics and in patients with renal artery stenosis. (See PRECAUTIONS.) Reversible
minor increases in blood urea nitrogen and serum creatinine were observed in approximately 11.6% of
patients with heart failure on concomitant diuretic therapy. Frequently, these abnormalities resolved
when the dosage of the diuretic was decreased.
Hemoglobin and Hematocrit: Small decreases in hemoglobin and hematocrit (mean decreases of
Small decreases in hemoglobin and hematocrit (mean decreases of
approximately 0.4 g% and 1.3 vol%, respectively) occurred frequently in patients treated with Lisinopril
tablet but were rarely of clinical importance in patients without some other cause of anemia. In clinical
trials, less than 0.1% of patients discontinued therapy due to anemia. Hemolytic anemia has been
reported; a causal relationship to lisinopril cannot be excluded.
Liver Function Tests: Rarely, elevations of liver enzymes and/or serum bilirubin have occurred. (See
Rarely, elevations of liver enzymes and/or serum bilirubin have occurred. (See
WARNINGS, Hepatic Failure.)
In hypertensive patients, 2.0% discontinued therapy due to laboratory adverse experiences, principally
elevations in blood urea nitrogen (0.6%), serum creatinine (0.5%) and serum potassium (0.4%).
In the heart failure trials, 3.4% of patients discontinued therapy due to laboratory adverse experiences;
1.8% due to elevations in blood urea nitrogen and/or creatinine and 0.6% due to elevations in serum
potassium.
In the myocardial infarction trial, 2.0% of patients receiving Lisinopril tablet discontinued therapy due to
renal dysfunction (increasing creatinine concentration to over 3 mg/dL or a doubling or more of the
baseline serum creatinine concentration); less than 1.0% of patients discontinued therapy due to other
laboratory adverse experiences: 0.1% with hyperkalemia and less than 0.1% with hepatic enzyme
alterations.
OVERDOSAGE
Following a single oral dose of 20 g/kg no lethality occurred in rats, and death occurred in one of 20
mice receiving the same dose. The most likely manifestation of overdosage would be hypotension, for
which the usual treatment would be intravenous infusion of normal saline solution.
Lisinopril can be removed by hemodialysis. (See WARNINGS, Anaphylactoid Reactions During
Membrane Exposure.)
DOSAGE AND ADMINISTRATION
Hypertension
Initial Therapy: In patients with uncomplicated essential hypertension not on diuretic therapy, the
In patients with uncomplicated essential hypertension not on diuretic therapy, the
recommended initial dose is 10 mg once a day. Dosage should be adjusted according to blood
pressure response. The usual dosage range is 20 to 40 mg per day administered in a single daily
dose. The antihypertensive effect may diminish toward the end of the dosing interval regardless of the
administered dose, but most commonly with a dose of 10 mg daily. This can be evaluated by
measuring blood pressure just prior to dosing to determine whether satisfactory control is being
maintained for 24 hours. If it is not, an increase in dose should be considered. Doses up to 80 mg have
been used but do not appear to give greater effect. If blood pressure is not controlled with Lisinopril
tablet alone, a low dose of a diuretic may be added. Hydrochlorothiazide, 12.5 mg has been shown to
provide an additive effect. After the addition of a diuretic, it may be possible to reduce the dose of
Lisinopril tablet.
Diuretic Treated Patients: In hypertensive patients who are currently being treated with a diuretic,
: In hypertensive patients who are currently being treated with a diuretic,
symptomatic hypotension may occur occasionally following the initial dose of Lisinopril tablet. The
diuretic should be discontinued, if possible, for two to three days before beginning therapy with
Lisinopril tablet to reduce the likelihood of hypotension. (See WARNINGS.) The dosage of Lisinopril
tablet should be adjusted according to blood pressure response. If the patient"s blood pressure is not
controlled with Lisinopril tablet alone, diuretic therapy may be resumed as described above.
If the diuretic cannot be discontinued, an initial dose of 5 mg should be used under medical supervision
for at least two hours and until blood pressure has stabilized for at least an additional hour. (See
WARNINGS and PRECAUTIONS, Drug Interactions.)
Concomitant administration of Lisinopril tablet with potassium supplements, potassium salt substitutes,
or potassium-sparing diuretics may lead to increases of serum potassium. (See PRECAUTIONS.)
Dosage Adjustment in Renal Impairment: The usual dose of Lisinopril tablet (10 mg) is
The usual dose of Lisinopril tablet (10 mg) is
recommended for patients with creatinine clearance >30 mL/min (serum creatinine of up to
approximately 3 mg/dL). For patients with creatinine clearance ≥10 mL/min ≤30 mL/min (serum
creatinine ≥3 mg/dL), the first dose is 5 mg once daily. For patients with creatinine clearance <10
mL/min (usually on hemodialysis) the recommended initial dose is 2.5 mg. The dosage may be titrated
upward until blood pressure is controlled or to a maximum of 40 mg daily.
Renal Status Creatinine Clearance mL/min Initial Dose mg/day Normal Renal Function to
Mild Impairment >30 10
Moderate to Severe Impairment ≥10 ≤30 5
Dialysis Patients* <10 2.5**
* See WARNINGS, Anaphylactoid Reactions During Membrane Exposure.
* See WARNINGS, Anaphylactoid Reactions During Membrane Exposure.
**Dosage or dosing interval should be adjusted depending on the blood pressure response.
Dosage or dosing interval should be adjusted depending on the blood pressure response.
Heart Failure
Lisinopril tablet is indicated as adjunctive therapy with diuretics and (usually) digitalis. The
recommended starting dose is 5 mg once a day. When initiating treatment with lisinopril in patients with
heart failure, the initial dose should be administered under medical observation, especially in those
patients with low blood pressure (systolic blood pressure below 100 mmHg). The mean peak blood
pressure lowering occurs six to eight hours after dosing. Observation should continue until blood
pressure is stable. The concomitant diuretic dose should be reduced, if possible, to help minimize
hypovolemia which may contribute to hypotension. (See WARNINGS and PRECAUTIONS, Drug
Interactions.) The appearance of hypotension after the initial dose of Lisinopril tablet does not preclude
subsequent careful dose titration with the drug, following effective management of the hypotension.
The usual effective dosage range is 5 to 40 mg per day administered as a single daily dose. The dose
of Lisinopril tablet can be increased by increments of no greater than 10 mg, at intervals of no less
than 2 weeks to the highest tolerated dose, up to a maximum of 40 mg daily. Dose adjustment should
be based on the clinical response of individual patients.
Dosage Adjustment in Patients with Heart Failure and Renal Impairment or Hyponatremia: In
In
patients with heart failure who have hyponatremia (serum sodium <130 mEq/L) or moderate to severe
renal impairment (creatinine clearance ≤30 mL/min or serum creatinine >3 mg/dL), therapy with
Lisinopril tablet should be initiated at a dose of 2.5 mg once a day under close medical supervision.
(See WARNINGS and PRECAUTIONS, Drug Interactions.)
Acute Myocardial Infarction
In hemodynamically stable patients within 24 hours of the onset of symptoms of acute myocardial
infarction, the first dose of Lisinopril tablet is 5 mg given orally, followed by 5 mg after 24 hours, 10 mg
after 48 hours and then 10 mg of Lisinopril tablet once daily. Dosing should continue for six weeks.
Patients should receive, as appropriate, the standard recommended treatments such as thrombolytics,
aspirin, and beta-blockers.
Patients with a low systolic blood pressure (≤120 mmHg) when treatment is started or during the first 3
days after the infarct should be given a lower 2.5 mg oral dose of Lisinopril tablet (see WARNINGS). If
hypotension occurs (systolic blood pressure ≤100 mmHg) a daily maintenance dose of 5 mg may be
given with temporary reductions to 2.5 mg if needed. If prolonged hypotension occurs (systolic blood
pressure <90 mmHg for more than 1 hour) Lisinopril tablet should be withdrawn. For patients who
develop symptoms of heart failure, see DOSAGE AND ADMINISTRATION, Heart Failure.
Dosage Adjustment in Patients With Myocardial Infarction with Renal Impairment: In acute
In acute
myocardial infarction, treatment with Lisinopril tablet should be initiated with caution in patients with
evidence of renal dysfunction, defined as serum creatinine concentration exceeding 2 mg/dL. No
evaluation of dosing adjustments in myocardial infarction patients with severe renal impairment has
been performed
Use in Elderly
In general, the clinical response was similar in younger and older patients given similar doses of
Lisinopril tablet. Pharmacokinetic studies, however indicate that maximum blood levels and area under
the plasma concentration time curve (AUC) are doubled in older patients, so that dosage adjustments
should be made with particular caution.
Pediatric Hypertensive Patients ≥6 Years of age
≥6 Years of age
The usual recommended starting dose is 0.07 mg/kg once daily (up to 5 mg total). Dosage should be
adjusted according to blood pressure response. Doses above 0.61 mg/kg (or in excess of 40 mg) have
not been studied in pediatric patients. (See CLINICAL PHARMACOLOGY, Pharmacokinetics and
Metabolism and Pharmacodynamics and Clinical Effects.)
Lisinopril tablet is not recommend in pediatric patients <6 years or in pediatric patients with glomerular
filtration rate <30 mL/min/1.73 min2 (see CLINICAL PHARMACOLOGY, Pharmacokinetics and
Metabolism and Pharmacodynamics and Clinical Effects and PRECAUTIONS).
Preparation of Suspension (for 200 mL of a 1.0 mg/mL suspension): Add 10 mL of Purified Water
Add 10 mL of Purified Water
USP to a polyethylene terephthalate (PET) bottle containing ten 20 mg tablets of Lisinopril tablet and
shake for at least one minute. Add 30 mL of Bicitra®† diluent and 160 mL of Ora Sweet SF™†† to the
concentrate in the PET bottle and gently shake for several seconds to disperse the ingredients. The
suspension should be stored at or below 250C (770F) and can be stored for up to four weeks. Shake
the suspension before each use.
† Registered trademark of Alza Corporation
Registered trademark of Alza Corporation
†† Trademark of Paddock Laboratories, Inc.
Trademark of Paddock Laboratories, Inc.
HOW SUPPLIED
2.5 mg Tablets, white to off-white, round biconvex uncoated tablets debossed with “W” on one side
white to off-white, round biconvex uncoated tablets debossed with “W” on one side
and other side plain.
(NDC 0615-7639-39) Blistercards of 30 tablets
(NDC 0615-7639-31) Blistercards of 31 tablets
5 mg Tablets, white to off-white, round biconvex uncoated tablets debossed with “ ” on one side and
white to off-white, round biconvex uncoated tablets debossed with “ ” on one side and
breakline on other side.
(NDC 0615-7540-39) Blistercards of 30 tablets
(NDC 0615-7540-31) Blistercards of 31 tablets
(NDC 0615-7540-05) Blistercards of 15 tablets
10 mg Tablets, white to off-white, round biconvex uncoated tablets debossed with “ ” on one side
white to off-white, round biconvex uncoated tablets debossed with “ ” on one side
and other side plain.
(NDC 0615-7541-39) Blistercards of 30 tablets
(NDC 0615-7541-31) Blistercards of 31 tablets
(NDC 0615-7541-05) Blistercards of 15 tablets
20 mg Tablets, mottled light yellow, round biconvex uncoated tablets debossed with
mottled light yellow, round biconvex uncoated tablets debossed with
“ ” on one side and other side plain.
(NDC 0615-7642-39) Blistercards of 30 tablets
(NDC 0615-7542-31) Blistercards of 31 tablets
(NDC 0615-7542-05) Blistercards of 15 tablets
30 mg Tablets, mottled light red, round biconvex uncoated tablets debossed with “ ” on one side
mottled light red, round biconvex uncoated tablets debossed with “ ” on one side
and other side plain.
(NDC 0615-7643-39) Bottles of 30 tablets
40 mg Tablets, mottled light brown, round biconvex uncoated tablets debossed with
mottled light brown, round biconvex uncoated tablets debossed with
“ ” on one side and other side plain.
(NDC 0615-7644-39) Blistercards of 30 tablets
(NDC 0615-7644-31) Blistercards of 31 tablets
(NDC 0615-7644-05) Blistercards of 15 tablets
REFERENCES
Storage
Store at controlled room temperature, 20-250C (68-770F) [see USP]. Protect from moisture, freezing
and excessive heat. Dispense in a tight container.
*AN69 is a registered trademark of Hospal Ltd.
AN69 is a registered trademark of Hospal Ltd.
Manufactured by:
Wockhardt Limited
Mumbai, India.
Distributed by:
Wockhardt USA LLC.
20 Waterview Blvd.
Parsippany, NJ 07054
USA.
Iss.080409




| LISINOPRIL
lisinopril tablet, film coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| LISINOPRIL
lisinopril tablet, film coated |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| LISINOPRIL
lisinopril tablet, film coated |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| LISINOPRIL
lisinopril tablet, film coated |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| LISINOPRIL
lisinopril tablet, film coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| LISINOPRIL
lisinopril tablet, film coated |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| ANDA | ANDA078402 | 04/19/2007 | |
| Labeler - NCS HealthCare of KY, Inc dba Vangard Labs (050052943) |
| Establishment | |||
| Name | Address | ID/FEI | Operations |
| NCS HealthCare of KY, Inc dba Vangard Labs | 050052943 | RELABEL, REPACK | |
Revised: 11/2011 NCS HealthCare of KY, Inc dba Vangard Labs