azactam (aztreonam) injection, solution
[Bristol-Myers Squibb Company]
To reduce the development of drug-resistant bacteria and maintain the effectiveness of AZACTAM® and other antibacterial drugs, AZACTAM should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
DESCRIPTION
AZACTAM® (aztreonam injection) contains the active ingredient aztreonam, a monobactam. It was originally isolated from Chromobacterium violaceum. It is a synthetic bactericidal antibiotic.
The monobactams, having a unique monocyclic beta-lactam nucleus, are structurally different from other beta-lactam antibiotics (e.g., penicillins, cephalosporins, cephamycins). The sulfonic acid substituent in the 1-position of the ring activates the beta-lactam moiety; an aminothiazolyl oxime side chain in the 3-position and a methyl group in the 4-position confer the specific antibacterial spectrum and beta-lactamase stability.
Aztreonam is designated chemically as (Z)-2-[[[(2-amino-4-thiazolyl)[[(2S,3S)-2-methyl-4-oxo-1-sulfo-3-azetidinyl]carbamoyl]methylene]amino]oxy]-2-methylpropionic acid. Structural formula:
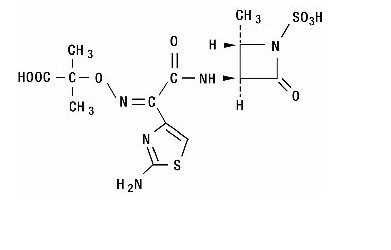
C13H17N5O8S2 MW 435.44
AZACTAM (aztreonam injection) in the Galaxy plastic container (PL 2040) is a frozen, iso-osmotic, sterile, sodium-free, nonpyrogenic intravenous solution. Each 50 mL of solution contains 1 g, or 2 g aztreonam with approximately 1.7 g, or 700 mg dextrose hydrous, USP added to adjust osmolality, and approximately 780 mg, or 1.6 g of arginine added for pH adjustment, respectively. Thawed solutions have a pH in the range of 4.5 to 7.5. The solution is for intravenous administration following thawing at room temperature or under refrigeration.
This Galaxy container is fabricated from a specially designed multilayer plastic (PL 2040). Solutions are in contact with the polyethylene layer of this container and can leach out certain chemical components of the plastic in very small amounts within the expiration period. The suitability of the plastic has been confirmed in tests in animals according to the USP biological tests for plastic containers as well as by tissue culture toxicity studies.
CLINICAL PHARMACOLOGY
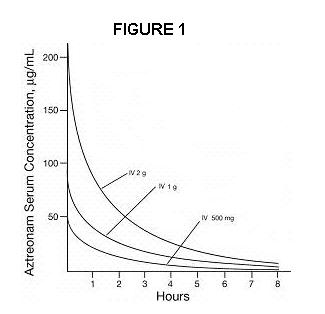
Single 30-minute intravenous infusions of 500-mg, 1-g and 2-g doses of AZACTAM in healthy subjects produced aztreonam peak serum levels of 54, 90 and 204 µg/mL, respectively, immediately after administration; at eight hours, serum levels were 1, 3 and 6 µg/mL, respectively (Figure 1). Single 3-minute intravenous injections of the same doses resulted in serum levels of 58, 125 and 242 µg/mL at five minutes following completion of injection.
Serum concentrations of aztreonam following completion of single intravenous infusions of 500-mg, 1-g, and 2-g doses are depicted in Figure 1.
The serum levels of aztreonam following single 500-mg, 1-g or 2-g intravenous doses of AZACTAM (aztreonam injection) exceed the MIC90 for Neisseria sp., Haemophilus influenzae and most genera of the Enterobacteriaceae for eight hours (for Enterobacter sp., the eight-hour serum levels exceed the MIC for 80 percent of strains). For Pseudomonas aeruginosa, a single 2-g intravenous dose produces serum levels that exceed the MIC90 for approximately four to six hours. All of the above doses of AZACTAM result in average urine levels of aztreonam that exceed the MIC90 for the same pathogens for up to 12 hours.
When aztreonam pharmacokinetics were assessed for adult and pediatric patients, they were found to be comparable (down to 9-months old). The serum half-life of aztreonam averaged 1.7 hours (1.5 to 2.0) in subjects with normal renal function, independent of the dose. In healthy subjects, based on a 70 kg person, the serum clearance was 91 mL/min and renal clearance was 56 mL/min; the apparent mean volume of distribution at steady-state averaged 12.6 liters, approximately equivalent to extracellular fluid volume.
In elderly patients, the mean serum half-life of aztreonam increased and the renal clearance decreased, consistent with the age-related decrease in creatinine clearance.1-4 The dosage of AZACTAM should be adjusted accordingly (see DOSAGE AND ADMINISTRATION: Renal Impairment in Adult Patients).
In patients with impaired renal function, the serum half-life of aztreonam is prolonged. (See DOSAGE AND ADMINISTRATION: Renal Impairment in Adult Patients.) The serum half-life of aztreonam is only slightly prolonged in patients with hepatic impairment since the liver is a minor pathway of excretion.
Average urine concentrations of aztreonam were approximately 1100, 3500 and 6600 µg/mL within the first two hours following single 500-mg, 1-g and 2-g intravenous doses of AZACTAM (30-minute infusions), respectively. The range of average concentrations for aztreonam in the 8- to 12- hour urine specimens in these studies was 25 to 120 µg/mL. In healthy subjects, aztreonam is excreted in the urine about equally by active tubular secretion and glomerular filtration. Approximately 60 to 70 percent of an intravenous dose was recovered in the urine by eight hours. Urinary excretion of a single intravenous dose was essentially complete by 12 hours after injection. About 12 percent of a single intravenous radiolabeled dose was recovered in the feces. Unchanged aztreonam and the inactive beta-lactam ring hydrolysis product of aztreonam were present in feces and urine.
Intravenous administration of a single 500-mg or 1-g dose of AZACTAM every eight hours for seven days to healthy subjects produced no apparent accumulation of aztreonam or modification of its disposition characteristics; serum protein binding averaged 56 percent and was independent of dose.
Renal function was monitored in healthy subjects given aztreonam; standard tests (serum creatinine, creatinine clearance, BUN, urinalysis and total urinary protein excretion) as well as special tests (excretion of N-acetyl-β-glucosaminidase, alanine aminopeptidase and β2-microglobulin) were used. No abnormal results were obtained.
Aztreonam achieves measurable concentrations in the following body fluids and tissues:
|
Fluid or Tissue |
Dose (g) |
Route |
Hours Post-injection | Number of Patients | Mean Concentration (µg/mL or µg/g) |
| 1Tissue penetration is regarded as essential to therapeutic efficacy, but specific tissue levels have not been correlated with specific therapeutic effects. | |||||
| Fluids | |||||
| bile | 1 | IV | 2 | 10 | 39 |
| blister fluid | 1 | IV | 1 | 6 | 20 |
| bronchial secretion | 2 | IV | 4 | 7 | 5 |
| cerebrospinal fluid (inflamed meninges) | 2 | IV | 0.9-4.3 | 16 | 3 |
| pericardial fluid | 2 | IV | 1 | 6 | 33 |
| pleural fluid | 2 | IV | 1.1-3.0 | 3 | 51 |
| synovial fluid | 2 | IV | 0.8-1.9 | 11 | 83 |
| Tissues | |||||
| atrial appendage | 2 | IV | 0.9-1.6 | 12 | 22 |
| endometrium | 2 | IV | 0.7-1.9 | 4 | 9 |
| fallopian tube | 2 | IV | 0.7-1.9 | 8 | 12 |
| fat | 2 | IV | 1.3-2.0 | 10 | 5 |
| femur | 2 | IV | 1.0-2.1 | 15 | 16 |
| gallbladder | 2 | IV | 0.8-1.3 | 4 | 23 |
| kidney | 2 | IV | 2.4-5.6 | 5 | 67 |
| large intestine | 2 | IV | 0.8-1.9 | 9 | 12 |
| liver | 2 | IV | 0.9-2.0 | 6 | 47 |
| lung | 2 | IV | 1.2-2.1 | 6 | 22 |
| myometrium | 2 | IV | 0.7-1.9 | 9 | 11 |
| ovary | 2 | IV | 0.7-1.9 | 7 | 13 |
| skeletal muscle | 2 | IV | 0.3-0.7 | 6 | 16 |
| skin | 2 | IV | 0.0-1.0 | 8 | 25 |
| sternum | 2 | IV | 1 | 6 | 6 |
The concentration of aztreonam in saliva at 30 minutes after a single 1-g intravenous dose (9 patients) was 0.2 µg/mL; in human milk at two hours after a single 1-g intravenous dose (6 patients), 0.2 µg/mL; in amniotic fluid at six to eight hours after a single 1-g intravenous dose (5 patients), 2 µg/mL. The concentration of aztreonam in peritoneal fluid obtained one to six hours after multiple 2-g intravenous doses ranged between 12 and 90 µg/mL in 7 of 8 patients studied.
Aztreonam given intravenously rapidly reaches therapeutic concentrations in peritoneal dialysis fluid; conversely, aztreonam given intraperitoneally in dialysis fluid rapidly produces therapeutic serum levels.
Concomitant administration of probenecid or furosemide and aztreonam causes clinically insignificant increases in the serum levels of aztreonam. Single-dose intravenous pharmacokinetic studies have not shown any significant interaction between aztreonam and concomitantly administered gentamicin, nafcillin sodium, cephradine, clindamycin or metronidazole. No reports of disulfiram-like reactions with alcohol ingestion have been noted; this is not unexpected since aztreonam does not contain a methyl-tetrazole side chain.
Microbiology
Aztreonam exhibits potent and specific activity in vitro against a wide spectrum of gram-negative aerobic pathogens including Pseudomonas aeruginosa. The bactericidal action of aztreonam results from the inhibition of bacterial cell wall synthesis due to a high affinity of aztreonam for penicillin binding protein 3 (PBP3). Aztreonam, unlike the majority of beta-lactam antibiotics, does not induce beta-lactamase activity and its molecular structure confers a high degree of resistance to hydrolysis by beta-lactamases (i.e., penicillinases and cephalosporinases) produced by most gram-negative and gram-positive pathogens; it is, therefore, usually active against gram-negative aerobic microorganisms that are resistant to antibiotics hydrolyzed by beta-lactamases. It is active against many strains that are multiply-resistant to other antibiotics, such as certain cephalosporins, penicillin, and aminoglycosides. Aztreonam maintains its antimicrobial activity over a pH range of 6 to 8 in vitro, as well as in the presence of human serum and under anaerobic conditions.
Aztreonam has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.
| Aerobic gram-negative microorganisms: |
|---|
| Citrobacter species, including C. freundii |
| Enterobacter species, including E. cloacae |
| Escherichia coli |
| Haemophilus influenzae (including ampicillin-resistant and other penicillinase-producing strains) |
| Klebsiella oxytoca |
| Klebsiella pneumoniae |
| Proteus mirabilis |
| Pseudomonas aeruginosa |
| Serratia species, including S. marcescens |
The following in vitro data are available, but their clinical significance is unknown.
Aztreonam exhibits in vitro minimal inhibitory concentrations (MICs) of 8 µg/mL or less against most (≥90%) strains of the following microorganisms; however, the safety and effectiveness of aztreonam in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled clinical trials.
| Aerobic gram-negative microorganisms: |
|---|
| Aeromonas hydrophila |
| Morganella morganii |
| Neisseria gonorrhoeae (including penicillinase-producing strains) |
| Pasteurella multocida |
| Proteus vulgaris |
| Providencia stuartii |
| Providencia rettgeri |
| Yersinia enterocolitica |
Aztreonam and aminoglycosides have been shown to be synergistic in vitro against most strains of P. aeruginosa, many strains of Enterobacteriaceae, and other gram-negative aerobic bacilli.
Alterations of the anaerobic intestinal flora by broad spectrum antibiotics may decrease colonization resistance, thus permitting overgrowth of potential pathogens, e.g., Candida and Clostridium species. Aztreonam has little effect on the anaerobic intestinal microflora in in vitro studies. Clostridium difficile and its cytotoxin were not found in animal models following administration of aztreonam. (See ADVERSE REACTIONS: Gastrointestinal.)
Susceptibility Tests
Dilution Techniques: Quantitative methods are used to determine antimicrobial minimal inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method5 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of aztreonam powder. The MIC values should be interpreted according to the following criteria:
| a. Interpretative criteria applicable only to tests performed by broth microdilution method using Haemophilus Test Medium (HTM).5 | |||
| b. The current absence of data on resistant strains precludes defining any categories other than “Susceptible”. Strains yielding MIC results suggestive of a “nonsusceptible” category should be submitted to a reference laboratory for further testing. | |||
| For testing aerobic microorganisms other than Haemophilus influenzae: | |||
| MIC (µg/mL) | Interpretation | ||
| ≤8 | Susceptible (S) | ||
| 16 | Intermediate (I) | ||
| ≥32 | Resistant (R) | ||
| When testing Haemophilus influenzaea: | |||
| MIC (µg/mL) | Interpretationb | ||
| ≤2 | Susceptible (S) | ||
A report of “Susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable. A report of “Intermediate” indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “Resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable; other therapy should be selected.
Standardized susceptibility test procedures require the use of laboratory control microorganisms to control the technical aspects of the laboratory procedures. Standard aztreonam powder should provide the following MIC values:
| a. Range applicable only to tests performed by broth microdilution method using Haemophilus Test Medium (HTM).5 | |
| Microorganism | MIC (µg/mL) |
|---|---|
| Escherichia coli ATCC 25922 | 0.06-0.25 |
| Haemophilus influenzaea ATCC 49247 | 0.12-0.5 |
| Pseudomonas aeruginosa ATCC 27853 | 2.0-8.0 |
Diffusion Techniques: Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure6 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 30-µg aztreonam to test the susceptibility of microorganisms to aztreonam.
Reports from the laboratory providing results of the standard single-disk susceptibility test with a 30-µg aztreonam disk should be interpreted according to the following criteria:
| a. Interpretative criteria applicable only to tests performed by disk diffusion method using Haemophilus Test Medium (HTM).6 | |||
| b. The current absence of data on resistant strains precludes defining any categories other than “Susceptible.” Strains yielding zone diameter results suggestive of a “nonsusceptible” category should be submitted to a reference laboratory for further testing. | |||
| For testing aerobic microorganisms other than Haemophilus influenzae: | |||
| Zone diameter (mm) | Interpretation | ||
| ≥22 | Susceptible (S) | ||
| 16 - 21 | Intermediate (I) | ||
| ≤15 | Resistant (R) | ||
| When testing Haemophilus influenzaea: | |||
| Zone diameter (mm) | Interpretationb | ||
| ≥26 | Susceptible (S) | ||
Interpretation should be as stated above for results using dilution techniques. Interpretation involves correlation of the diameter obtained in the disk test with the MIC for aztreonam.
As with standardized dilution techniques, diffusion methods require the use of laboratory control microorganisms that are used to control the technical aspects of the laboratory procedures. For the diffusion technique, the 30-µg aztreonam disk should provide the following zone diameters in these laboratory test quality control strains.
| a. Range applicable only to tests performed by disk diffusion method using Haemophilus Test Medium (HTM).6 | |
| Microorganism | Zone diameter (mm) |
|---|---|
| Escherichia coli ATCC 25922 | 28-36 mm |
| Haemophilus influenzaea ATCC 49247 | 30-38 mm |
| Pseudomonas aeruginosa ATCC 27853 | 23-29 mm |
INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectiveness of AZACTAM® and other antibacterial drugs, AZACTAM should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
AZACTAM (aztreonam injection) is indicated for the treatment of the following infections caused by susceptible gram-negative microorganisms:
Urinary Tract Infections (complicated and uncomplicated), including pyelonephritis and cystitis (initial and recurrent) caused by Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa, Enterobacter cloacae, Klebsiella oxytoca*, Citrobacter species* and Serratia marcescens*.
Lower Respiratory Tract Infections, including pneumonia and bronchitis caused by Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Haemophilus influenzae, Proteus mirabilis, Enterobacter species and Serratia marcescens*.
Septicemia caused by Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Proteus mirabilis*, Serratia marcescens* and Enterobacter species.
Skin and Skin-Structure Infections, including those associated with postoperative wounds, ulcers and burns caused by Escherichia coli, Proteus mirabilis, Serratia marcescens, Enterobacter species, Pseudomonas aeruginosa, Klebsiella pneumoniae and Citrobacter species*.
Intra-abdominal Infections, including peritonitis caused by Escherichia coli, Klebsiella species including K. pneumoniae, Enterobacter species including E. cloacae*, Pseudomonas aeruginosa, Citrobacter species* including C. freundii* and Serratia species* including S. marcescens*.
Gynecologic Infections, including endometritis and pelvic cellulitis caused by Escherichia coli, Klebsiella pneumoniae*, Enterobacter species* including E. cloacae* and Proteus mirabilis*.
AZACTAM (aztreonam injection) is indicated for adjunctive therapy to surgery in the management of infections caused by susceptible organisms, including abscesses, infections complicating hollow viscus perforations, cutaneous infections and infections of serous surfaces. AZACTAM is effective against most of the commonly encountered gram-negative aerobic pathogens seen in general surgery.
*Efficacy for this organism in this organ system was studied in fewer than ten infections.
Concurrent Therapy
Concurrent initial therapy with other antimicrobial agents and AZACTAM is recommended before the causative organism(s) is known in seriously ill patients who are also at risk of having an infection due to gram-positive aerobic pathogens. If anaerobic organisms are also suspected as etiologic agents, therapy should be initiated using an anti-anaerobic agent concurrently with AZACTAM (see DOSAGE AND ADMINISTRATION). Certain antibiotics (e.g., cefoxitin, imipenem) may induce high levels of beta-lactamase in vitro in some gram-negative aerobes such as Enterobacter and Pseudomonas species, resulting in antagonism to many beta-lactam antibiotics including aztreonam. These in vitro findings suggest that such beta-lactamase inducing antibiotics not be used concurrently with aztreonam. Following identification and susceptibility testing of the causative organism(s), appropriate antibiotic therapy should be continued.
CONTRAINDICATIONS
This preparation is contraindicated in patients with known hypersensitivity to aztreonam or any other component in the formulation.
WARNINGS
Both animal and human data suggest that AZACTAM is rarely cross-reactive with other beta-lactam antibiotics and weakly immunogenic. Treatment with aztreonam can result in hypersensitivity reactions in patients with or without prior exposure. (See CONTRAINDICATIONS.)
Careful inquiry should be made to determine whether the patient has any history of hypersensitivity reactions to any allergens.
While cross-reactivity of aztreonam with other beta-lactam antibiotics is rare, this drug should be administered with caution to any patient with a history of hypersensitivity to beta-lactams (e.g., penicillins, cephalosporins, and/or carbapenems). Treatment with aztreonam can result in hypersensitivity reactions in patients with or without prior exposure to aztreonam. If an allergic reaction to aztreonam occurs, discontinue the drug and institute supportive treatment as appropriate (e.g., maintenance of ventilation, pressor amines, antihistamines, corticosteroids). Serious hypersensitivity reactions may require epinephrine and other emergency measures. (See ADVERSE REACTIONS.)
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including aztreonam, and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents.
Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is one primary cause of “antibiotic-associated colitis.”
After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug clinically effective against C. difficile colitis.
Rare cases of toxic epidermal necrolysis have been reported in association with aztreonam in patients undergoing bone marrow transplant with multiple risk factors including sepsis, radiation therapy and other concomitantly administered drugs associated with toxic epidermal necrolysis.
PRECAUTIONS
General
Prescribing AZACTAM in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
In patients with impaired hepatic or renal function, appropriate monitoring is recommended during therapy.
If an aminoglycoside is used concurrently with aztreonam, especially if high dosages of the former are used or if therapy is prolonged, renal function should be monitored because of the potential nephrotoxicity and ototoxicity of aminoglycoside antibiotics.
The use of antibiotics may promote the overgrowth of nonsusceptible organisms, including gram-positive organisms (Staphylococcus aureus and Streptococcus faecalis) and fungi. Should superinfection occur during therapy, appropriate measures should be taken.
Information for Patients
Patients should be counseled that antibacterial drugs including AZACTAM should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When AZACTAM is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by AZACTAM or other antibacterial drugs in the future.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies in animals have not been performed.
Genetic toxicology studies performed in vivo and in vitro with aztreonam in several standard laboratory models revealed no evidence of mutagenic potential at the chromosomal or gene level.
Two-generation reproduction studies in rats at daily doses up to 20 times the maximum recommended human dose, prior to and during gestation and lactation, revealed no evidence of impaired fertility. There was a slightly reduced survival rate during the lactation period in the offspring of rats that received the highest dosage, but not in offspring of rats that received five times the maximum recommended human dose.
Pregnancy
Pregnancy Category B
Aztreonam crosses the placenta and enters the fetal circulation.
Studies in pregnant rats and rabbits, with daily doses up to 15 and 5 times, respectively, the maximum recommended human dose, revealed no evidence of embryo- or fetotoxicity or teratogenicity. No drug induced changes were seen in any of the maternal, fetal, or neonatal parameters that were monitored in rats receiving 15 times the maximum recommended human dose of aztreonam during late gestation and lactation.
There are no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, aztreonam should be used during pregnancy only if clearly needed.
Nursing Mothers
Aztreonam is excreted in human milk in concentrations that are less than 1 percent of concentrations determined in simultaneously obtained maternal serum; consideration should be given to temporary discontinuation of nursing and use of formula feedings.
Pediatric Use
The safety and effectiveness of intravenous AZACTAM have been established in the age groups 9 months to 16 years. Use of AZACTAM in these age groups is supported by evidence from adequate and well-controlled studies of AZACTAM in adults with additional efficacy, safety, and pharmacokinetic data from noncomparative clinical studies in pediatric patients. Sufficient data are not available for pediatric patients under 9 months of age or for the following treatment indications/pathogens: septicemia and skin and skin-structure infections (where the skin infection is believed or known to be due to H. influenzae type b). In pediatric patients with cystic fibrosis, higher doses of AZACTAM may be warranted. (See CLINICAL PHARMACOLOGY, DOSAGE AND ADMINISTRATION, and CLINICAL STUDIES.)
Geriatric Use
Clinical studies of AZACTAM did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.7-10 In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
In elderly patients, the mean serum half-life of aztreonam increased and the renal clearance decreased, consistent with the age-related decrease in creatinine clearance.1-4 Since aztreonam is known to be substantially excreted by the kidney, the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, renal function should be monitored and dosage adjustments made accordingly (see DOSAGE AND ADMINISTRATION: Renal Impairment in Adult Patients and Dosage in the Elderly).
AZACTAM contains no sodium.
ADVERSE REACTIONS
Local reactions (e.g., phlebitis/thrombophlebitis; discomfort/swelling) following IV administration occurred at rates of approximately 1.9 percent.
Systemic reactions (considered to be related to therapy or of uncertain etiology) occurring at an incidence of 1 to 1.3 percent include diarrhea, nausea and/or vomiting, and rash. Reactions occurring at an incidence of less than 1 percent are listed within each body system in order of decreasing severity:
Hypersensitivity—anaphylaxis, angioedema, bronchospasm
Hematologic—pancytopenia, neutropenia, thrombocytopenia, anemia, eosinophilia, leukocytosis, thrombocytosis
Gastrointestinal—abdominal cramps; rare cases of C. difficile-associated diarrhea, including pseudomembranous colitis, or gastrointestinal bleeding have been reported. Onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment. (See WARNINGS.)
Dermatologic—toxic epidermal necrolysis (see WARNINGS), purpura, erythema multiforme, exfoliative dermatitis, urticaria, petechiae, pruritus, diaphoresis
Cardiovascular—hypotension, transient ECG changes (ventricular bigeminy and PVC), flushing
Respiratory—wheezing, dyspnea, chest pain
Hepatobiliary—hepatitis, jaundice
Nervous System—seizure, confusion, vertigo, paresthesia, insomnia, dizziness
Musculoskeletal—muscular aches
Special Senses—tinnitus, diplopia, mouth ulcer, altered taste, numb tongue, sneezing, nasal congestion, halitosis
Other—vaginal candidiasis, vaginitis, breast tenderness
Body as a Whole—weakness, headache, fever, malaise
Pediatric Adverse Reactions
Of the 612 pediatric patients who were treated with AZACTAM in clinical trials, less than 1% required discontinuation of therapy due to adverse events. The following systemic adverse events, regardless of drug relationship, occurred in at least 1% of treated patients in domestic clinical trials: rash (4.3%), diarrhea (1.4%), and fever (1.0%). These adverse events were comparable to those observed in adult clinical trials.
In 343 pediatric patients receiving intravenous therapy, the following local reactions were noted: pain (12%), erythema (2.9%), induration (0.9%), and phlebitis (2.1%). In the US patient population, pain occurred in 1.5% of patients, while each of the remaining three local reactions had an incidence of 0.5%.
The following laboratory adverse events, regardless of drug relationship, occurred in at least 1% of treated patients: increased eosinophils (6.3%), increased platelets (3.6%), neutropenia (3.2%), increased AST (3.8%), increased ALT (6.5%), and increased serum creatinine (5.8%).
In US pediatric clinical trials, neutropenia (absolute neutrophil count less than 1000/mm3) occurred in 11.3% of patients (8/71) younger than 2 years receiving 30 mg/kg q6h. AST and ALT elevations to greater than 3 times the upper limit of normal were noted in 15-20% of patients aged 2 years or above receiving 50 mg/kg q6h. The increased frequency of these reported laboratory adverse events may be due to either increased severity of illness treated or higher doses of AZACTAM administered.
Adverse Laboratory Changes
Adverse laboratory changes without regard to drug relationship that were reported during clinical trials were:
Hepatic—elevations of AST (SGOT), ALT (SGPT), and alkaline phosphatase; signs or symptoms of hepatobiliary dysfunction occurred in less than 1 percent of recipients (see above).
Hematologic—increases in prothrombin and partial thromboplastin times, positive Coombs’ test.
Renal—increases in serum creatinine.
OVERDOSAGE
If necessary, aztreonam may be cleared from the serum by hemodialysis and/or peritoneal dialysis.
DOSAGE AND ADMINISTRATION
Dosage in Adult Patients
AZACTAM (aztreonam injection), an intravenous solution in Galaxy plastic containers (PL 2040), is intended for intravenous use only. Dosage should be determined by susceptibility of the causative organisms, severity and site of infection, and the condition of the patient.
The intravenous route is recommended for patients with bacterial septicemia, localized parenchymal abscess (e.g., intra-abdominal abscess), peritonitis or other severe systemic or life-threatening infections.
The duration of therapy depends on the severity of infection. Generally, AZACTAM should be continued for at least 48 hours after the patient becomes asymptomatic or evidence of bacterial eradication has been obtained. Persistent infections may require treatment for several weeks. Doses smaller than those indicated should not be used.
Renal Impairment in Adult Patients
Prolonged serum levels of aztreonam may occur in patients with transient or persistent renal insufficiency. Therefore, the dosage of AZACTAM should be halved in patients with estimated creatinine clearances between 10 and 30 mL/min/1.73 m2 after an initial loading dose of 1 g or 2 g.
When only the serum creatinine concentration is available, the following formula (based on sex, weight, and age of the patient) may be used to approximate the creatinine clearance (Clcr). The serum creatinine should represent a steady state of renal function.
weight (kg) x (140-age)
Males: Clcr = ———————————————
72 x serum creatinine (mg/dL)
Females: 0.85 x above value
In patients with severe renal failure (creatinine clearance less than 10 mL/min/1.73 m2), such as those supported by hemodialysis, the usual dose of 500 mg, 1 g or 2 g should be given initially. The maintenance dose should be one-fourth of the usual initial dose given at the usual fixed interval of 6, 8 or 12 hours. For serious or life-threatening infections, in addition to the maintenance doses, one-eighth of the initial dose should be given after each hemodialysis session.
Dosage In The Elderly
Renal status is a major determinant of dosage in the elderly; these patients in particular may have diminished renal function. Serum creatinine may not be an accurate determinant of renal status. Therefore, as with all antibiotics eliminated by the kidneys, estimates of creatinine clearance should be obtained, and appropriate dosage modifications made if necessary.
Dosage in Pediatric Patients
AZACTAM should be administered intravenously to pediatric patients with normal renal function. There are insufficient data regarding intramuscular administration to pediatric patients or dosing in pediatric patients with renal impairment. (See PRECAUTIONS: Pediatric Use.)
| AZACTAM DOSAGE GUIDELINES | |||
|---|---|---|---|
|
Type of Infection |
Dose | Frequency (hours) |
|
| ADULTS* | |||
| Urinary tract infections | 500 mg or 1 g | 8 or 12 | |
| Moderately severe systemic infections | 1 g or 2 g | 8 or 12 | |
| Severe systemic or life- threatening infections | 2 g | 6 or 8 | |
| *Maximum recommended dose is 8 g per day | |||
| PEDIATRIC PATIENTS** | |||
| Mild to moderate infections | 30 mg/kg | 8 | |
| Moderate to severe infections | 30 mg/kg | 6 or 8 | |
| **Maximum recommended dose is 120 mg/kg/day | |||
Because of the serious nature of infections due to Pseudomonas aeruginosa, dosage of 2 g every six or eight hours is recommended, at least upon initiation of therapy, in systemic infections caused by this organism in adults.
CLINICAL STUDIES
A total of 612 pediatric patients aged 1 month to 12 years were enrolled in uncontrolled clinical trials of aztreonam in the treatment of serious gram-negative infections, including urinary tract, lower respiratory tract, skin and skin-structure, and intra-abdominal infections.
Directions for Use of AZACTAM (aztreonam injection) in Galaxy Plastic Container (PL 2040).
AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040) is to be administered as an intermittent intravenous infusion only.
Storage
Store in a freezer capable of maintaining a temperature of -20° C (-4° F).
Thawing of Plastic Containers
Thaw frozen container at room temperature, 25° C (77° F) or in a refrigerator, 2° to 8° C (36° to 46° F). After thawing is complete, invert the container to assure a well-mixed solution. (DO NOT FORCE THAW BY IMMERSION IN WATER BATHS OR BY MICROWAVE IRRADIATION.)
Check for minute leaks by squeezing container firmly. If leaks are detected, discard solution as sterility may be impaired.
The container should be visually inspected. Thawed solutions should not be used unless clear; solutions will be colorless to yellow. Components of the solution may precipitate in the frozen state and will dissolve upon reaching room temperature with little or no agitation. If after visual inspection the solution remains discolored, cloudy, or if an insoluble precipitate is noted or if any seals or outlet ports are not intact, the container should be discarded.
DO NOT ADD SUPPLEMENTARY MEDICATION.
The thawed solution in Galaxy plastic container (PL 2040) remains chemically stable for either 14 days under refrigeration (2° to 8° C/36° to 46° F) or for 48 hours at room temperature (25° C/77° F). DO NOT REFREEZE THAWED ANTIBIOTICS.
Preparation for Intravenous Administration (Use aseptic technique)
- Suspend container(s) from eyelet support.
- Remove protector from outlet port at bottom of container.
- Attach administration set. Refer to complete directions accompanying set.
Additives or other medication should not be added to AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040) or infused simultaneously through the same intravenous line. If the same intravenous line is used for sequential infusion of several different drugs, it should be flushed before and after infusion of AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040) with an infusion solution compatible with AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040)* and any other drug(s) administered via this common line.
It is recommended that the intravenous administration apparatus be replaced at least once every 48 hours.
CAUTION: Do not use plastic containers in series connections. Such use could result in an embolism due to residual air being drawn from the primary container before administration of the fluid from the secondary container is complete.
Intravenous Administration
Infusion of AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040) should be completed within a 20 to 60 minute period. The plastic container is a single-dose unit; discard any unused portion remaining in the container.
*The following infusion solutions are compatible with AZACTAM (aztreonam injection) in Galaxy plastic container (PL 2040):
- Sodium Chloride Injection USP, 0.9%
- Ringer’s Injection USP
- Lactated Ringer’s Injection USP
- Dextrose Injection USP, 5% or 10%
- Dextrose and Sodium Chloride Injection USP, 5%:0.9%
- 5%:0.45% or 5%:0.2%
- Sodium Lactate Injection USP (M/6 Sodium Lactate)
- Ionosol® B and 5% Dextrose
- Isolyte® E
- Isolyte® E with 5% Dextrose
- Isolyte® M with 5% Dextrose
- Normosol®-R
- Normosol®-R and 5% Dextrose
- Normosol®-M and 5% Dextrose
- Mannitol Injection USP, 5% or 10%
- Lactated Ringer’s and 5% Dextrose Injection
- Plasma-Lyte® M and 5% Dextrose
- 10% Travert® Injection
- 10% Travert® and Electrolyte No. 1 Injection
- 10% Travert® and Electrolyte No. 2 Injection
- 10% Travert® and Electrolyte No. 3 Injection
HOW SUPPLIED
AZACTAM® (aztreonam injection) in Galaxy® plastic container (PL 2040) is supplied as a frozen, 50 mL single-dose intravenous solution as follows:
| 1-g aztreonam/50 mL container: | |
|---|---|
| Packages of 24 | NDC 51479-048-01 |
| 2-g aztreonam/50 mL container: | |
| Packages of 24 | NDC 51479-049-01 |
Store at or below -20° C (-4° F) [See Directions for Use of AZACTAM® (aztreonam injection) in Galaxy® Plastic Container (PL 2040)].
REFERENCES
- Naber KG, Dette GA, Kees F, Knothe H, Grobecker H. Pharmacokinetics, in vitro activity, therapeutic efficacy, and clinical safety of aztreonam vs. cefotaxime in the treatment of complicated urinary tract infections. J Antimicrob Chemother 1986; 17:517-527.
- Creasey WA, Platt TB, Frantz M, Sugerman AA. Pharmacokinetics of aztreonam in elderly male volunteers. Br J Clin Pharmacol 1985; 19:233-237.
- Meyers BR, Wilkinson P, Mendelson MH, et al. Pharmacokinetics of aztreonam in healthy elderly and young adult volunteers. J Clin Pharmacol 1993; 33:470-474.
- Sattler FR, Schramm M, Swabb EA. Safety of aztreonam and SQ 26,992 in elderly patients with renal insufficiency. Rev Infect Dis 1985; 7 (suppl 4):S622-S627.
- National Committee for Clinical Laboratory Standards. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically—Fifth Edition. Approved Standard NCCLS Document M7-A5, Vol. 20, No. 2, NCCLS, Wayne, PA, January 2000.
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Disk Susceptibility Tests—Seventh Edition. Approved Standard NCCLS Document M2-A7, Vol. 20, No. 1, NCCLS, Wayne, PA, January 2000.
- Deger F, Douchamps J, Freschi E, et al. Aztreonam in the treatment of serious gram-negative infections in the elderly. Int J Clin Pharmacol Ther and Toxicol 1988; 26: 22-26.
- Knockaert DC, Dejaeger E, Nestor L, et al. Aztreonam-flucloxacillin double beta-lactam treatment as empirical therapy of serious infections in very elderly patients. Age and Aging 1981; 20:135-139.
- Roelandts F. Clinical use of aztreonam in a psychogeriatric population. Acta Clin Belg 1992; 47:251-255.
- Andrews R, Fasoli R, Scoggins WG, et al. Combined aztreonam and gentamicin therapy for pseudomonal lower respiratory tract infections. Clin Therap 1994; 16:236-252.
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing—Eleventh Informational Supplement, NCCLS Document M100-S11, Vol. 21, No. 1, NCCLS, Wayne, PA, January 2001.
AZACTAM® is a registered trademark of Bristol-Myers Squibb Company licensed exclusively in the US to EPI.
Galaxy®, Dianeal®, Plasma-Lyte®, and Travert® are registered trademarks of Baxter International, Inc.
Ionosol® and Normosol® are registered trademarks of Abbott Laboratories Corporation.
Isolyte® is a registered trademark of McGaw Inc.
AZACTAM® (aztreonam injection) in Galaxy® plastic container (PL 2040) is
manufactured to Bristol-Myers Squibb
specifications by
Baxter Healthcare Corporation
Deerfield, IL 60015
for
Bristol-Myers Squibb Company
Princeton, NJ 08543
Distributed by
Elan Biopharmaceuticals,
a business unit of Elan Pharmaceuticals, Inc. (EPI),
a member of the Elan Group,
San Diego, CA 92121 USA
© 2004 Elan Pharmaceuticals, Inc.
J4668D / 1178463 / 6000854
January 2004
| AZACTAM (aztreonam) | ||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
| AZACTAM (aztreonam) | ||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
Revised: 10/2006