IPRIVASK
-
desirudin injection, powder, lyophilized, for solution
Canyon Pharmaceuticals, Inc.
----------
Iprivask 15 mgDESCRIPTION
Iprivask [Desirudin for Injection] is a specific inhibitor of human thrombin. It has a
protein structure that is similar to that of hirudin, the naturally occurring anticoagulant
present in the peripharyngeal glands in the medicinal leech, Hirudo medicinalis.
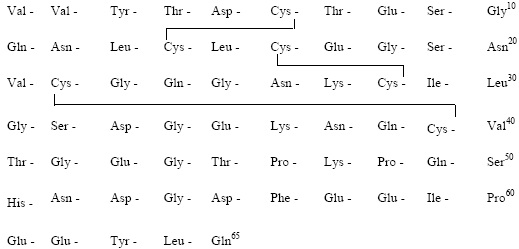
Hirudin is a single polypeptide chain of 65 amino acids residues and contains
three disulfide bridges. Desirudin has a chemical formula of C287H440N80O110S6
with a molecular weight of 6963.52. Desirudin, which is expressed in yeast
(Saccharomyces cerevisiae, strain TR 1456) by recombinant DNA technology differs from
the natural hirudin by lack of a sulfate group on Tyr-63. The biological activity of
desirudin is determined through a chromogenic assay which measures the ability of
desirudin to inhibit the hydrolysis of a chromogenic peptidic substrate by thrombin in
comparison to a desirudin standard. One vial of desirudin contains 15.75 mg
desirudin corresponding to approximately 315,000 antithrombin units (ATU) or
20,000 ATU per milligram of desirudin with reference to the WHO International
Standard (prepared 1991) for alphathrombin.
Iprivask 15 mg is supplied as a sterile, white, freeze dried powder for injection. Each
vial contains 15.75 mg desirudin and the following inactive ingredients: 1.31 mg
anhydrous magnesium chloride USP, sodium hydroxide for injection USP. Each
prefilled syringe of diluent for Iprivask contains 0.6 mL sterile Mannitol USP (3%)
in Water for Injection and is preservative free. See DOSAGE AND
ADMINISTRATION section for reconstitution instructions. Iprivask 15 mg is
administered by subcutaneous (SC) injection, preferably at an abdominal or thigh site.
To prepare the reconstituted aqueous solution, 0.5 mL of the mannitol diluent is added
under aseptic conditions to the vial containing the sterile powder. Shaking gently rapidly
disperses the drug. The reconstituted solution has a pH of 7.4.
STRUCTURAL FORMULA
CLINICAL PHARMACOLOGY
Mechanism of Action: Desirudin is a selective inhibitor of free circulating and
clot-bound thrombin. The anticoagulant properties of desirudin are demonstrated by its
ability to prolong the clotting time of human plasma. One molecule of desirudin binds to
one molecule of thrombin and thereby blocks the thrombogenic activity of thrombin.
As a result, all thrombin-dependent coagulation assays are affected. Activated
partial thromboplastin time (aPTT) is a measure of the anticoagulant activity of
desirudin and increases in a dose-dependent fashion. The pharmacodynamic effect of
desirudin on proteolytic activity of thrombin was assessed as an increase in aPTT. A
mean peak aPTT prolongation of about 1.38 times baseline value (range 0.58 to 3.41)
was observed following subcutaneous b.i.d. injections of 15 mg desirudin. Thrombin
time (TT) frequently exceeds 200 seconds even at low plasma concentrations of
desirudin, which renders this test unsuitable for routine monitoring of Iprivask
therapy. At therapeutic serum concentrations, desirudin has no effect on other
enzymes of the hemostatic system such as factors IXa, Xa, kallikrein, plasmin,
tissue plasminogen activator, or activated protein C. In addition, it does not display
any effect on other serine proteases, such as the digestive enzymes trypsin, chymotrypsin,
or on complement activation by the classical or alternative pathways.
Pharmacokinetic Properties
Pharmacokinetic parameters were calculated based on plasma concentration data
obtained by a nonspecific ELISA method that does not discriminate between native
desirudin and its metabolites. It is not known if the metabolites are pharmacologically
active.
Absorption: The absorption of desirudin is complete when subcutaneously
administered at doses of 0.3 mg/kg or 0.5 mg/kg. Following subcutaneous
administration of single doses of 0.1 to 0.75 mg/kg, plasma concentrations of desirudin
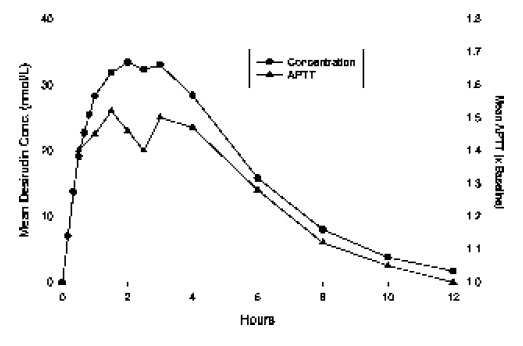
increased to a maximum level (Cmax) between 1 and 3 hours. Both Cmax and
area-under-the-curve (AUC) values are dose proportional.
Mean Desirudin Concentrations and Changes in APTT
After A Single 15 mg Subcutaneous Dose in 12 Healthy Subjects
Distribution: The pharmacokinetic properties of desirudin following intravenous (IV) administration are well described by a two- or three- compartment disposition model. Desirudin is distributed in the extracellular space with a volume of distribution at steady state of 0.25 L/kg, independent of the dose. Desirudin binds specifically and directly to thrombin, forming an extremely tight, non-covalent complex with an inhibition
constant of approximately 2.6 x 10-13 M. Thus, free or protein bound desirudin
immediately binds circulating thrombin. The pharmacological effect of desirudin is not
modified when co-administered with highly protein bound drugs (greater than 99%).
Metabolism: Human and animal data suggest that desirudin is primarily eliminated
and metabolized by the kidney. The total urinary excretion of unchanged desirudin
amounts to 40 to 50% of the administered dose. Metabolites lacking one or two
C-terminal amino acids constitute a minor proportion of the material recovered from
urine (less than 7%). There is no evidence for the presence of other metabolites. This indicates
that desirudin is metabolized by stepwise degradation from the C-terminus probably catalyzed by carboxypeptidase(s) such as carboxypeptidase A, originating from the
pancreas. Total clearance of desirudin is approximately 1.5 to 2.7 mL/min/kg following
either subcutaneous or IV administration and is independent of dose. This clearance
value is close to the glomerular filtration rate.
Elimination: The elimination of desirudin from plasma is rapid after IV
administration, with approximately 90% of the dose disappearing from the plasma
within 2 hours of the injection. Plasma concentrations of desirudin then decline with a
mean terminal elimination half-life of 2 to 3 hours. After subcutaneous administration,
the mean terminal elimination half-life is also approximately 2 hours.
Special Populations:
Renal Insufficiency: In a pharmacokinetic study of renally impaired subjects,
subjects with mild [creatinine clearance (CC) between 61 and 90 mL/min/1.73 m2
body surface area], moderate (CC between 31 and 60 mL/min/1.73 m2 body surface
area), and severe (CC below 31 mL/min/1.73 m2 body surface area) renal
insufficiency, were administered a single IV dose of 0.5, 0.25, or 0.125 mg/kg desirudin,
respectively. This resulted in mean dose-normalized AUCeffect (AUC0-60th for
aPTT prolongation) increases of approximately 3-, and 9-fold for the moderate and
severe renally impaired subjects, respectively, compared with healthy individuals. In
subjects with mild renal impairment, there was no increase in AUCeffect compared with
healthy individuals. In subjects with severe renal insufficiency, terminal elimination
half-lives were prolonged up to 12 hours compared with 2 to 4 hours in normal
volunteers or subjects with mild to moderate renal insufficiency (see WARNINGS).
Dose adjustments are recommended in certain circumstances in relation to the degree of
impairment or degree of aPTT abnormality (see WARNINGS: Renal Insufficiency,
PRECAUTIONS: Laboratory Tests, and DOSAGE AND ADMINISTRATION:
Monitoring and Adjusting Therapy; Use in Renal Insufficiency).
Hepatic Insufficiency: No pharmacokinetic studies have been conducted to investigate
the effects of Iprivask in hepatic insufficiency (see PRECAUTIONS, Hepatic
Insufficiency/Liver Injury and DOSAGE and ADMINISTRATION).
Age/Gender: The mean plasma clearance of desirudin in patientsgreater than or equal to 65 years of
age (n=12; 110 mL/min) is approximately 28% lower than in patients less than 65 years of age
(n=8; 153 mL/min). Population pharmacokinetics conducted in 301 patients undergoing
elective total hip replacement indicate that age or gender do not affect the systemic
clearance of desirudin when renal creatinine clearance is considered. This drug is
substantially excreted by the kidney, and the risk of adverse events due to it may be
greater in patients with impaired renal function. Because elderly patients are more
likely to have decreased renal function, care should be taken in dose selection, and it
may be useful to monitor renal function. Dosage adjustment in the case of moderate and
severe renal impairment is necessary. (See CLINICAL PHARMACOLOGY, Special
Populations, Renal Insufficiency, DOSAGE and ADMINISTRATION, Use in Renal
Insufficiency).
CLINICAL TRIALS
Iprivask was evaluated in two controlled, randomized, multicenter, clinical
efficacy trials and a controlled, double-blind, dose-finding study. In the efficacy
studies, Iprivask was compared to subcutaneously administered unfractionated heparin
or enoxaparin sodium for the reduction of the risk of venous thromboembolic events
(VTE) in patients undergoing total hip replacement surgery. In all studies Iprivask was
initiated prior to surgery and continued for 8 to 12 days postoperatively (median duration
10 days). Patients who received Iprivask had a lower incidence of VTE. The efficacy
studies are described below.
In the first study, Iprivask 15 mg subcutaneously administered every 12 hours was
compared to unfractionated heparin 5000 IU subcutaneously administered every 8
hours. A total of 445 patients were randomized in the study, 436 patients were treated,
and 85 of the treated patients were excluded from efficacy analysis, mainly because of
no phlebography or inadequate reading of phlebography. Patients ranged in age from 34
to 89 years (mean age 68.4 years) with 41.8% men and 58.2% women. All enrolled
patients were Caucasian. Iprivask significantly reduced the number of total VTE
compared to unfractionated heparin: Evaluable population: Iprivask, 13/174 (7.5%) vs.
heparin, 41/177 (23.2%); p value less than0.001; Intent-to-Treat population: Iprivask
13/225 (5.8%) vs. heparin 42/220 (19.1%);p value less than 0.0001.]. Significantly fewer
patients in the group treated with Iprivask experienced proximal DVT than those
patients treated with heparin: Evaluable population: Iprivask 6/174 (3.4%) vs. heparin
29/177 (16.4%); p value less than 0.001: Intent-to-Treat population: Iprivask 6/225 (2.7%)
vs. heparin 30/220 (13.6%); p value less than 0.0001.
In a second study, Iprivask 15 mg subcutaneously administered every 12 hours was
compared to enoxaparin sodium 40 mg subcutaneously administered every 24 hours. A
total of 2079 patients were randomized in the study, 2049 patients were treated, and
508 of the treated patients were excluded from efficacy analysis mainly because of no
phlebography or inadequate reading of phlebography. Patients ranged in age from 18 to
90 years (mean age 68.5 years) with 41.7% men and 58.5% women. All enrolled
patients were Caucasian. In the both the evaluable patient population and the
intent-to-treat population, patients who received Iprivask had a lower incidence of major
VTE, total VTE, and proximal DVT than did patients who received enoxaparin (see
table below).
| Efficacy of Iprivask in Hip Replacement Surgery Patients | Efficacy of Iprivask in Hip Replacement Surgery Patients | Efficacy of Iprivask in Hip Replacement Surgery Patients | Efficacy of Iprivask in Hip Replacement Surgery Patients |
| Dosing Regimen | Dosing Regimen | Dosing Regimen | Dosing Regimen |
|
| Iprivask a 15 mg q12h SC | Enoxaparin 40 mg qd |
|
| Evaluable Hip Replacement Surgery Patients | n equal to 773 | n equal to 768 |
|
|
| n (%) | n (%) | p Value |
| Treatment failures Major VTEb,c Total VTEe Proximal DVT | 39 (4. 9) d | 61 (7.9) | p less than 0.02 |
| Treatment failures Major VTEb,c Total VTEe Proximal DVT | 145 (18.8) | 197 (25.7) | p less than 0.001 |
| Treatment failures Major VTEb,c Total VTEe Proximal DVT | 36 (4.5) | 59 (7.7) | p equal to 0.012 |
| Intent-to-Treat Hip Replacement Surgery Patients | n equal to 1043 | n equal to 1036 |
|
| Treatment Failures Major VTEb Total VTEe Proximal DVT | n (%) | n (%) | p Value |
| Treatment Failures Major VTEb Total VTEe Proximal DVT | 39 (3.7)f | 61 (5.9) | p equal to 0.024 |
| Treatment Failures Major VTEb Total VTEe Proximal DVT | 145 (13.9) | 199 (19.2) | p equal to 0.001 |
| Treatment Failures Major VTEb Total VTEe Proximal DVT | 36 (3.5) | 59 (5.7) | p equal to 0.012 |
anesthesia, if used.
b Major VTE included proximal DVT, PE, or death.
c Total number of patients in this evaluation: Iprivask 802; Enoxaparin 785.
d Odds ratio 0.61 with 95% Confidence Interval of: 0.40; 0.92
e Total VTE = Venous thromboembolic events which included DVT (including proximal events),
PE, or death considered to be thromboembolic in origin.
f Odds ratio 0.62 with 95% Confidence Interval of 0.41; 0.94
In a multicenter, double-blind, dose-finding study, Iprivask 10 mg, 15 mg, and 20 mg
subcutaneously administered every 12 hours was compared to unfractionated heparin
5,000 IU administered every 8 hours SC in patients undergoing hip replacement
surgery. A dose response was seen with regard to both effectiveness and bleeding
complications. The 15-mg and 20-mg doses were superior to heparin and the 10-mg
dose. In a smaller, open-labeled, dose-finding study of Iprivask 10 mg, 15 mg, 20 mg,
and 40 mg subcutaneously administered every 12 hours in patients undergoing hip
replacement surgery, the 40-mg dose was associated with unacceptable major bleeding.
INDICATIONS AND USAGE
Iprivask is indicated for the prophylaxis of deep vein thrombosis, which may lead
to pulmonary embolism, in patients undergoing elective hip replacement surgery.
CONTRAINDICATIONS
Iprivask is contraindicated in patients with known hypersensitivity to natural or
recombinant hirudins, and in patients with active bleeding and/or irreversible
coagulation disorders.
WARNINGS
Renal Insufficiency: Iprivask must be used with caution in patients with renal
impairment, particularly in those with moderate and severe renal
impairment (creatinine clearance ≤60 mL/min/1.73 m2 body surface area)
(see CLINICAL PHARMACOLOGY, Special Populations, Renal Insufficiency).
Dose reductions by factors of three and nine are recommended for pat ients wi th
moderate and severe renal impairment respect ively (see DOSAGE AND
ADMINISTRATION). In addition, daily aPTT and serum creatinine monitoring
are recommended for patients with moderate or severe renal impairment (see
PRECAUTIONS, Laboratory Tests).
Hemorrhagic Events: Iprivask is not intended for intramuscular injection as
local hematoma formation may result.
Iprivask, like other anticoagulants, should be used with caution in patients with
increased risks of hemorrhage such as those with recent major surgery, organ biopsy or
puncture of a non-compressible vessel within the last month; a history of
hemorrhagic stroke, intracranial or intraocular bleeding including diabetic
(hemorrhagic) retinopathy; recent ischemic stroke, severe uncontrolled
hypertension, bacterial endocarditis, a known hemostatic disorder (congenital or
acquired, e.g. hemophilia, liver disease) or a history of gastrointestinal or
pulmonary bleeding within the past 3 months.
Bleeding can occur at any site during therapy with Iprivask. An unexplained fall in
hematocrit or blood pressure should lead to a search for a bleeding site.
Spinal/Epidural Anesthesia: As with other anticoagulants, there is a risk of neuraxial
hematoma formation with the concurrent use of desirudin and spinal/epidural anesthesia,
which has the potential to result in long term or permanent paralysis. The risk may be
greater with the use of post-operative indwelling catheters or the concomitant use of
additional drugs affecting hemostasis such as NSAIDs (Non-Steroidal
Anti-Inflammatory Drugs), platelet inhibitors or other anticoagulants (see Boxed
WARNING and PRECAUTIONS, Drug Interactions). The risk may also be increased
by traumatic or repeated neuraxial puncture.
To reduce the potential risk of bleeding associated with the concurrent use of desirudin
and epidural or spinal anesthesia/analgesia, the pharmacokinetic profile of the
drug should be considered (see CLINICAL PHARMACOLOGY, Pharmacokinetic properties) when scheduling or using epidural or spinal anesthesia in
proximity to desirudin administration. The physician should consider placement of the
catheter prior to initiating desirudin and removal of the catheter when the anticoagulant
effect of desirudin is low (see DOSAGE and ADMINISTRATION).
Should the physician decide to administer anticoagulation in the context of
epidural/spinal anesthesia, extreme vigilance and frequent monitoring must be exercised
to detect any signs and symptoms of neurological impairment such as midline back pain,
sensory and motor deficits (numbness or weakness in lower limbs), bowel and/or bladder
dysfunction. Patients should be instructed to inform their physician immediately if they
experience any of the above signs or symptoms. If signs or symptoms of spinal
hematoma are suspected, urgent diagnosis and treatment including spinal cord
decompression should be initiated.
The physician should consider the potential benefit versus risk before neuraxial
intervention in patients anticoagulated or to be anticoagulated for thromboprophylaxis
(see also WARNINGS, Hemorrhage, and PRECAUTIONS, Drug Interactions).
Iprivask cannot be used interchangeably with other hirudins as they differ in
manufacturing process and specific biological activity (ATUs). Each of these medicines
has its own instructions for use.
PRECAUTIONS
Antibodies/Re-exposure: Antibodies have been reported in patients treated with
hirudins. Potential for cross-sensitivity to hirudin products cannot be excluded. Irritative
skin reactions were observed in 9/322 volunteers exposed to Iprivask by subcutaneous
injection or IV bolus or infusion in single or multiple administrations of the drug.
Allergic events were reported in less than 2% of patients who were administered desirudin in
Phase III clinical trials. Allergic events were reported in 1% of patients receiving
unfractionated heparin and 1% of patients receiving enoxaparin. Hirudin-specific
IgE evaluations may not be indicative of sensitivity to Iprivask as this test was not
always positive in the presence of symptoms. Very rarely, anti-hirudin antibodies have
been detected upon re-exposure to desirudin. (See ADVERSE REACTIONS,
Non-hemorrhagic Events, Allergic Reactions). Fatal anaphylactoid reactions have been
reported during hirudin therapy.
Hepatic Insufficiency/Liver Injury: No information is available about the use
of desirudin in patients with hepatic insufficiency/liver injury. Although Iprivask is
not significantly metabolized by the liver, hepatic impairment or serious liver injury
(e.g., liver cirrhosis) may alter the anticoagulant effect of Iprivask due to coagulation
defects secondary to reduced generation of vitamin K-dependent coagulation factors.
Iprivask should be used with caution in these patients.
Laboratory Tests: Activated partial thromboplastin time (aPTT) should be
monitored daily in patients with increased risk of bleeding and/or renal impairment. Serum creatinine should be monitored daily in patients with renal
impairment. Peak aPTT should not exceed two times control. Should peak aPTT
exceed this level, dose reduction is advised based on the degree of aPTT
abnormality (see DOSAGE and ADMINISTRATION, Initial Dosage, Use in Renal
Insufficiency). If necessary, therapy with desirudin should be interrupted until aPTT
falls to less than two times control, at which time treatment with desirudin can
be resumed at a reduced dose. (See Drug Interactions for information on use of
Iprivask in conjunction with other drugs affecting coagulation). Thrombin time (TT) is
not a suitable test for routine monitoring of Iprivask therapy (see CLINICAL
PHARMACOLOGY, Mechanism of Action). Dose adjustments based on serum
creatinine may be necessary (see DOSAGE AND ADMINISTRATION, Use in Renal
Insufficiency).
Drug Interactions: Any agent which may enhance the risk of hemorrhage should be
discontinued prior to initiation of desirudin therapy. These agents include medications
such as Dextran 40, systemic glucocorticoids, thrombolytics, and anticoagulants. If
co-administration cannot be avoided, close clinical and laboratory moni toring
should be conducted. During prophylaxis of venous thromboembolism,
concomitant treatment with heparins (unfractionated and low-molecular weight
heparins) or dextrans is not recommended. The effects of desirudin and unfractionated
heparins on prolongation of aPTT are additive.
As with other anticoagulants, desirudin should be used with caution in conjunction with
drugs which affect platelet function. These medications include systemic salicylates,
NSAIDS including ketorolac, acetylsalicylic acid, ticlopidine, dipyridamole,
sulfinpyrazone, clopidogrel, abciximab and other glycoprotein IIb/IIIa antagonists (see
PRECAUTIONS, Laboratory Tests).
Use in patients switching from oral anticoagulants to Iprivask or from Iprivask to oral
anticoagulants. The concomitant administration of warfarin did not significantly affect
the pharmacokinetic effects of desirudin. When warfarin and desirudin were
co-administered, greater inhibition of hemostasis measured by activated partial
thromboplastin time (aPTT), prothrombin time (PT), and international normalized ratio
(INR) was observed. If a patient is switched from oral anticoagulants to Iprivask
therapy or from Iprivask to oral anticoagulants, the anticoagulant activity should
continue to be closely monitored with appropriate methods. That activity should be
taken into account in the evaluation of the overall coagulation status of the patient
during the switch.
Animal Pharmacology and Toxicology: General Toxicity Desirudin produced bleeding, local inflammation, and granulation at injection sites
in rat and dog toxicity studies. In a 28-day study in Rhesus monkeys, there was also evidence of subcutaneous bleeding and local inflammation at the injection sites. In addition, desirudin was immunogenic in dogs and formed antibody complexes resulting in prolonged half-life and accumulation. Desirudin showed sensitization potential in guinea pig immediate and delayed hypersensitivity models. Carcinogenesis, Mutagenesis, Impairment of Fertility. No long-term studies in animals have been performed to evaluate the carcinogenic potential of desirudin.
Desirudin was not genotoxic in the Ames test, the Chinese hamster lung cell (V79/HGPRT) forward mutation test or the rat micronucleus test. It was, however, equivocal in its genotoxic effect in Chinese hamster ovarian cell (CCL 61) chromosome aberration tests. Desirudin at subcutaneous doses up to 10mg/kg/day (about 2.7 times the recommended human dose based on body surface area) was found to have no effect on fertility and
reproductive performance of male and female rats.
Pregnancy: Teratogenic Effects: Pregnancy Category C. Teratology studies have been performed in rats at subcutaneous doses in a range of 1 to 15 mg/kg/day (about 0.3 to 4 times the recommended human dose based on body surface area) and in rabbits at IV doses in a range of 0.6 to 6mg/kg/day (about 0.3 to 3 times the recommended human dose based on body surface area) and have revealed desirudin to be teratogenic.
Observed teratogenic findings were: omphalocele, asymmetric and fused sternebrae, edema, shortened hind limbs, etc. in rats; and spina bifida, malrotated hind limb, hydrocephaly, gastroschisis, etc. in rabbits. There are no adequate and well controlled studies in pregnant women. Iprivask should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers: It is not known whether desirudin is excreted in human milk.
Because many drugs are excreted in human milk, caution should be exercised when
desirudin is administered to a nursing woman.
Geriatric Use: In three clinical studies of Iprivask, the percentage of patients greater than 65 years of age treated with 15 mg of Iprivask subcutaneously every 12 hours was 58.5%, while 20.8% were 75 years of age or older. Elderly patients treated with Iprivask had a reduction in the incidence of VTE similar to that observed in the younger patients, and a slightly lower incidence of VTE compared to those patients treated with heparin or enoxaparin.
Regarding safety, in the clinical studies the incidence of hemorrhage (major or otherwise) in patients 65 years of age or older was similar to that in patients less than 65 years of age. In addition, the elderly had a similar incidence of total, treatment-related, or serious adverse events compared to those patients less than 65 years of age. Serious adverse events occurred more frequently in patients 75 years of age or older as compared to those less than 65 years of age. In general, 15 mg desirudin every 12 hours can be used safely in the geriatric population as in the population of patients less than 65 years of age so long as renal function is adequate (see CLINICAL PHARMACOLOGY, Special Populations, Renal Insufficiency, DOSAGE and ADMINISTRATION, Use in Renal Insufficiency).
ADVERSE REACTIONS
In the Phase II and III clinical studies, desirudin was administered to 2159 patients undergoing elective hip replacement surgery to determine the safety and efficacy of Iprivask in preventing VTE in this population. Below is the safety profile of the Iprivask 15 mg (q12h) regimen from these 5 multicenter clinical trials. Hemorrhagic Events: The following rates of hemorrhagic events have been reported during clinical trials.
|
| Dosing Regimen | Dosing Regimen | Dosing Regimen |
|
| Iprivask | Heparin | Enoxaparin |
|
| 15 mg q12h SC N=1561 n (%) | 5000 IU q8h SC N=501 n (%) | 40 mg QD SC N=1036 n (%) |
| Patients with Any Hemorrhagea | 464 (30) | 111 (22) | 341 (33) |
| Patients with Serious Hemorrhageb | 41 (3) | 15 (3) | 21 (2) |
| Patients with Major Hemorrhagec | 13 (less than 1) | 0 (0) | 2 (less than 1) |
b. Bleeding complications were considered serious if perioperative transfusion requirements exceeded 5 units of whole blood or packed red cells, or if total transfusion requirements up to postoperative Day 6 inclusive exceeded 7 units of whole blood or packed red cells, or total blood loss up to postoperative Day 6 inclusive exceeded 3500 mL.
c. Bleeding complications were considered major if the hemorrhage was:
(1) overt and it produced a fall in hemoglobin of greater than or equal to 2g/dL or if it lead to a transfusion of 2 or more units of whole or packed cells outside the perioperative period (the time from start of surgery until up to 12 hours after);
(2) Retroperitoneal, intracranial, intraocular, intraspinal, or occurred in a major prosthetic joint
Non-hemorrhagic Events: Non-hemorrhagic adverse events occurring at greater than or equal to 2% incidence in patients treated with Iprivask 15 mg (q 12h) during elective hip replacement surgery and considered to be remotely, possibly, or probably related to desirudin are provided below.
|
| Iprivask | Heparin | Enoxaparin |
| Body System (Preferred Term) | 15 mg q12h SC N=1561 n (%) | 5000 IU q8h SC N=501 n (%) | 40 mg QD SC N=1036 n (%) |
| Injection Site Mass | 56 (4) | 32 (6) | 7 (less than 1) |
| Wound Secretion | 59 (4) | 23 (5) | 34 (3) |
| Anemia | 51 (3) | 11 (2) | 37 (4) |
| Deep Thrombophlebitis | 24 (2) | 41 (8) | 22 (2) |
| Nausea | 24 (2) | 5 (less than 1) | 10 (less than 1) |
b All hemorrhages that occurred are included in ADVERSE REACTIONS, Hemorrhagic Events.
Related Adverse Events with a Frequency of less than 2% and greater than 0.2% (in decreasing order of frequency): thrombosis, hypotension, leg edema, fever, decreased hemoglobin, hematuria, dizziness, epistaxis, vomiting, impaired healing, cerebrovascular disorder, leg pain, hematemesis.
Allergic Reactions. In clinical studies, allergic events were reported less than 2% overall and in 2% of patients who were administered 15 mg desi rudin. (See PRECAUTIONS, General , Ant ibodies/ Re-exposure).
Post Marketing: In addition to adverse events reported from clinical trials the following adverse events have been identified during post approval use of Iprivask. These events were reported voluntarily from a population of unknown size and the frequency of occurrence cannot be determined precisely: rare reports of major hemorrhages , some of which were fatal , and anaphylactic/anaphylactoid reactions.
OVERDOSAGE
In case of overdose, most likely reflected in hemorrhagic complications or suggested by excessively high aPTT values, Iprivask therapy should be discontinued. Emergency procedures should be instituted as appropriate (for example, determination of aPTT and other coagulation levels, hemoglobin, the use of blood transfusion or plasma expanders).
No specific antidote for Iprivask is available; however, the anticoagulant effect of desirudin is partially reversible using thrombin-rich plasma concentrates while aPTT levels can be reduced by the IV administration of 0.3 Mg/kg DDAVP (desmopressin). The clinical effectiveness of DDAVP in treating bleeding due to desirudin overdose has not been studied. In an open, pilot, dose-ascending study to assess safety, the highest dose of desirudin (40 mg q12h) caused excessive hemorrhage.
DOSAGE AND ADMINISTRATION
All patients should be evaluated for bleeding disorder risk before prophylactic administration of Iprivask (see PRECAUTIONS, Drug Interactions).
Initial Dosage: In patients undergoing hip replacement surgery, the recommended dose of Iprivask is 15 mg every 12 hours administered by subcutaneous injection with the initial dose given up to 5 to 15 minutes prior to surgery, but after induction of regional block anesthesia, if used (see WARNINGS, Spinal/Epidural Anesthesia). Up to 12 days administration (average duration 9 to 12 days) of Iprivask has been well tolerated in
controlled clinical trials.
| Degree of Renal Insufficiency | Creatinine Clearance [mL/min/1.73 m2 body surface area] | aPTT Monitoring and Dosing Instructions |
| Moderate | greater than or equal to 31 to 60 | Initiate therapy at 5 mg every 12 hours by subcutaneous injection. Monitor aPTT and serum creatinine at least daily. If aPTT exceeds 2 times control: 1. Interrupt therapy until the value returns to less than 2 times control. 2. Resume therapy at a reduced dose guided by the initial degree of aPTT abnormality |
| Severea | less than 31 | Initiate therapy at 1.7 mg every 12 hours by subcutaneous injection. Monitor aPTT and serum creatinine at least daily. If aPTT exceeds 2 times control: 1. Interrupt therapy until the value returns to less than 2 times control. 2. Consider further dose reductions guided by the initial degree of aPTT abnormality |
a See CLINICAL PHARMACOLOGY, Special Populations, Renal Insufficiency and WARNINGS, Renal Insufficiency. Use in Hepatic Insufficiency. In the absence of clinical studies in this population, dosing recommendations cannot be made at this time (see CLINICAL PHARMACOLOGY, Metabolism, Special Populations, Hepatic Insufficiency, and PRECAUTIONS, Hepatic Insufficiency).
Administration: Directions on Preparation
Use Iprivask before the expiration date given on the carton and container.
1. Reconstitution should be carried out under sterile conditions.
2. Remove plastic flip-top cap from IprivaskVial. Remove back cover of Vial Adapter package. Attach Vial Adapter to Vial by using the outer package to handle Adapter. Push Adapter down onto Vial until spike pierces rubber stopper and snaps into place. Discard Vial Adapter package.
3. Remove Syringe cap by twisting and pulling gently. Attach Syringe to Adapter on Vial by twisting. Slowly push plunger down to completely transfer solution into Vial. Leaving Syringe connected to Vial, gently swirl. Round tablet in Vial will dissolve within 10 seconds.
4. With Syringe still connected to Vial, turn Vial upside down and withdraw entire contents of Vial back into Syringe. Remove Syringe from Vial and hold it with plunger-end down.
5. You must use enclosed Eclipse™ needle. Attach Needle to Syringe by twisting. Pull pink lever down and uncap needle. You are ready to inject Iprivask. After injection, flip up pink lever to cover needle until it snaps into place. Dispose of the used Syringe in a Sharps® container.
Iprivask should not be mixed with other injections, solvents, or infusions. Iprivask is administered by subcutaneous injection. It must not be administered by intramuscular injection. Subcutaneous Injection Technique: Select a syringe with a 26 or 27 gauge needle which is approximately ½ inch in length for administration of Iprivask. Withdraw the entire reconstituted solution (15.75 mg desirudin/0.5 mL) into the
syringe and inject the total volume subcutaneously.
Patients should be sitting or lying down and Iprivask injection administered by deep subcutaneous injection. Administration should be alternated between the left and right anterolateral and left and right posterolateral thigh or abdominal wall. The whole length of the needle should be introduced into a skin fold held between the thumb and forefinger; the skin fold should be held throughout the injection. To minimize bruising, do not rub the injection site after completion of the injection.
HOW SUPPLIED
Iprivask [Desirudin for Injection] is supplied as a single dose (15.75 mg) lyophilized powder with an accompanying sterile, non-pyrogenic diluent [0.6 mL of Mannitol USP (3%) in Water for Injection].
Each Iprivask Vial contains 15.75 mg desirudin and the following inactive ingredients:
1.31 mg anhydrous magnesium chloride USP, sodium hydroxide for injection USP.
Each carton of Iprivask [Desirudin for Injection] contains 10 individual doses of Iprivask,
each in a separate tray.
Each tray of Iprivask [Desirudin for Injection] contains:
- One (1) x 15.75 mg Single Dose Vial
- One (1) x 0.6 mL Prefilled syringe of Diluent
- One (1) Eclipse™ needle
- One (1) Vial Adapter
Each prefilled syringe of diluent contains 0.6 mL Mannitol USP (3% w/v) in Water for
Injection provided for reconstitution of the desirudin lyophilized powder.
Distributed by:
Canyon Pharmaceuticals
11350 McCormick Rd., Ste. 400
Hunt Valley, MD 21031 USA Rev 0 1 / 1 0
Storage: Protect from light.
Unopened vials or prefilled syringes: Store at 25 degree Celsius (77 degree Fahrenheit); excursions permitted to 15–30 degree C (59-86 degree Fahrenheit). [See USP Controlled Room Temperature.]
Once Iprivask is reconstituted it may be used for up to 24 hours, when stored as indicated above. After 24 hours discard the solution.
Keep this and all medicines out of the reach of children.
SPINAL/EPIDURAL HEMATOMAS
When neuraxial anesthesia (epidural/spinal anesthesia) or spinal puncture is employed,
patients anticoagulated or scheduled to be anticoagulated with selective inhibitors of
thrombin such as Iprivask may be at risk of developing an epidural or spinal
hematoma which can result in long-term or permanent paralysis.
The risk of these events may be increased by the use of indwelling spinal catheters for
administration of analgesia or by the concomitant use of drugs affecting hemostasis such
as non- steroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, or other
anticoagulants. Likewise with such agents, the risk appears to be increased by traumatic
or repeated epidural or spinal puncture.
Patients should be frequently monitored for signs and symptoms of neurological
impairment. If neurological compromise is noted, urgent treatment is necessary.
The physician should consider the potential benefit versus risk before neuraxial
intervention, in patients anticoagulated or to be anticoagulated for thromboprophylaxis
(see also WARNINGS).
NDC 83055-111-12 Rx only
Directions for use: see insert.
Iprivask
(desirudin for injection) 15 mg*
FOR SUBCUTANEOUS INJECTION
Each Iprivask Vial contains
15.75 mg* desirudin to deliver 15 mg
Manufactured for and Distributed
by: Canyon Pharmaceuticals
Hunt Valley, MD 780-05329
Lot
Exp.
Rx only FOR SUBCUTANEOUS INJECTION NDC 83055-111-12
Iprivask
(desirudin for injection) 15 mg
Each vial of Iprivask also
contains the following inactive ingredients:
1.25 mg anhydrous magnesium chloride USP,
sodium hydroxide for injection USP.
Store at 25 degree Centigrade (77 degree F): excursions permitted to 15-30 degree Centigrade (59-86 degree F).
[See USP Controlled Room Temperature]. Protect from light.
Contents:
- One (1) 15.75 mg Single-Dose
Vial of Iprivask to deliver 15mg.
- One (1) 0.6 mL Prefilled Syringe of Diluent
- One (1) BD Eclipse Needle
- One (1) Vial Adapter
Bar Code
750-05513
Iprivask is a licensed trademark of
Canyon Pharmaceuticals Group
and its affillates.
Manufactured for and Distributed by:
Canyon Pharmaceuticals
Hunt Valley, MD 21031 USA
Lot
Exp.
Directions for use:
See package insert
Rx only NDC 83055-111-12
Iprivask
(desirudin for injection) 15mg
Contents:
Ten (10) pre-packaged trays each containing:
- 15.75 mg Single-Dose Vial of Iprivask to dellver 15mg
- 0.6 mL Prefilled Syringe of Diluent
- BD Eclipse Needle
- Vial Adapter
| IPRIVASK
desirudin injection, powder, lyophilized, for solution |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021271 | 06/10/2010 | |
| Labeler - Canyon Pharmaceuticals, Inc. (167549414) |
| Establishment | |||
| Name | Address | ID/FEI | Operations |
| Wasserburger Arzneimittelwerk, GmbH | 326482247 | manufacture | |