FENTORA
-
fentanyl citrate tablet
Cephalon Inc.
----------
FENTORA® CII(fentanyl buccal tablet)
Each tablet contains fentanyl citrate equivalent to fentanyl base: 100, 200, 300, 400, 600, 800 mcg
PHYSICIANS AND OTHER HEALTHCARE PROVIDERS MUST BECOME FAMILIAR WITH THE IMPORTANT WARNINGS IN THIS LABEL.
Reports of serious adverse events, including deaths in patients treated with FENTORA have been reported. Deaths occurred as a result of improper patient selection (e.g., use in opioid non-tolerant patients) and/or improper dosing. The substitution of FENTORA for any other fentanyl product may result in fatal overdose.
FENTORA is indicated only for the management of breakthrough pain in patients with cancer who are already receiving and who are tolerant to around-the-clock opioid therapy for their underlying persistent cancer pain. Patients considered opioid tolerant are those who are taking around-the-clock medicine consisting of at least 60 mg of oral morphine daily, at least 25 mcg of transdermal fentanyl/hour, at least 30 mg of oxycodone daily, at least 8 mg of oral hydromorphone daily or an equianalgesic dose of another opioid daily for a week or longer.
FENTORA is not indicated for use in opioid non-tolerant patients including those with only as needed (PRN) prior exposure.
FENTORA is contraindicated in the management of acute or postoperative pain including headache/migraine. Life-threatening respiratory depression could occur at any dose in opioid non-tolerant patients. Deaths have occurred in opioid non-tolerant patients.
When prescribing, do not convert patients on a mcg per mcg basis from Actiq® to FENTORA. Carefully consult the Initial Dosing Recommendations table. (See DOSAGE AND ADMINISTRATION, Table 7.)
When dispensing, do not substitute a FENTORA prescription for other fentanyl products. Substantial differences exist in the pharmacokinetic profile of FENTORA compared to other fentanyl products that result in clinically important differences in the extent of absorption of fentanyl. As a result of these differences, the substitution of FENTORA for any other fentanyl product may result in fatal overdose.
Special care must be used when dosing FENTORA. If the breakthrough pain episode is not relieved after 30 minutes, patients may take ONLY one additional dose using the same strength and must wait at least 4 hours before taking another dose. (See DOSAGE AND ADMINISTRATION.)
FENTORA contains fentanyl, an opioid agonist and a Schedule II controlled substance, with an abuse liability similar to other opioid analgesics. FENTORA can be abused in a manner similar to other opioid agonists, legal or illicit. This should be considered when prescribing or dispensing FENTORA in situations where the physician or pharmacist is concerned about an increased risk of misuse, abuse or diversion. Schedule II opioid substances which include morphine, oxycodone, hydromorphone, oxymorphone, and methadone have the highest potential for abuse and risk of fatal overdose due to respiratory depression.
Patients and their caregivers must be instructed that FENTORA contains a medicine in an amount which can be fatal to a child. Patients and their caregivers must be instructed to keep all tablets out of the reach of children. (See Information for Patients and Caregivers for disposal instructions.)
FENTORA is intended to be used only in the care of opioid tolerant cancer patients and only by healthcare professionals who are knowledgeable of and skilled in the use of Schedule II opioids to treat cancer pain.
The concomitant use of FENTORA with strong and moderate cytochrome P450 3A4 inhibitors may result in an increase in fentanyl plasma concentrations, and may cause potentially fatal respiratory depression.
DESCRIPTION
FENTORA (fentanyl buccal tablet) is a potent opioid analgesic, intended for buccal mucosal administration. FENTORA is formulated as a flat-faced, round, beveled-edge white tablet.
FENTORA is designed to be placed and retained within the buccal cavity for a period sufficient to allow disintegration of the tablet and absorption of fentanyl across the oral mucosa.
FENTORA employs the OraVescent® drug delivery technology, which generates a reaction that releases carbon dioxide when the tablet comes in contact with saliva. It is believed that transient pH changes accompanying the reaction may optimize dissolution (at a lower pH) and membrane permeation (at a higher pH) of fentanyl through the buccal mucosa.
Active Ingredient: Fentanyl citrate, USP is N-(1-Phenethyl-4-piperidyl) propionanilide citrate (1:1). Fentanyl is a highly lipophilic compound (octanol-water partition coefficient at pH 7.4 is 816:1) that is freely soluble in organic solvents and sparingly soluble in water (1:40). The molecular weight of the free base is 336.5 (the citrate salt is 528.6). The pKa of the tertiary nitrogens are 7.3 and 8.4. The compound has the following structural formula:
All tablet strengths are expressed as the amount of fentanyl free base, e.g., the 100 microgram strength tablet contains 100 micrograms of fentanyl free base.
Inactive Ingredients: Mannitol, sodium starch glycolate, sodium bicarbonate, sodium carbonate, citric acid, and magnesium stearate.
CLINICAL PHARMACOLOGY
Pharmacology:
Fentanyl is a pure opioid agonist whose principal therapeutic action is analgesia. Other members of the class known as opioid agonists include substances such as morphine, oxycodone, hydromorphone, codeine, and hydrocodone. Pharmacological effects of opioid agonists include anxiolysis, euphoria, feelings of relaxation, respiratory depression, constipation, miosis, cough suppression, and analgesia. Like all pure opioid agonist analgesics, with increasing doses there is increasing analgesia, unlike with mixed agonist/antagonists or non-opioid analgesics, where there is a limit to the analgesic effect with increasing doses. With pure opioid agonist analgesics, there is no defined maximum dose; the ceiling to analgesic effectiveness is imposed only by side effects, the more serious of which may include somnolence and respiratory depression.
Analgesia
The analgesic effects of fentanyl are related to the blood level of the drug, if proper allowance is made for the delay into and out of the CNS (a process with a 3-to-5-minute half-life).
In general, the effective concentration and the concentration at which toxicity occurs increase with increasing tolerance with any and all opioids. The rate of development of tolerance varies widely among individuals. As a result, the dose of FENTORA should be individually titrated to achieve the desired effect. (See DOSAGE AND ADMINISTRATION.)
Central Nervous System
The precise mechanism of the analgesic action is unknown although fentanyl is known to be a mu opioid receptor agonist. Specific CNS opioid receptors for endogenous compounds with opioid-like activity have been identified throughout the brain and spinal cord and play a role in the analgesic effects of this drug.
Fentanyl produces respiratory depression by direct action on brain stem respiratory centers. The respiratory depression involves both a reduction in the responsiveness of the brain stem to increases in carbon dioxide and to electrical stimulation.
Fentanyl depresses the cough reflex by direct effect on the cough center in the medulla. Antitussive effects may occur with doses lower than those usually required for analgesia. Fentanyl causes miosis even in total darkness. Pinpoint pupils are a sign of opioid overdose but are not pathognomonic (e.g., pontine lesions of hemorrhagic or ischemic origin may produce similar findings).
Gastrointestinal System
Fentanyl causes a reduction in motility associated with an increase in smooth muscle tone in the antrum of the stomach and in the duodenum. Digestion of food is delayed in the small intestine and propulsive contractions are decreased. Propulsive peristaltic waves in the colon are decreased, while tone may be increased to the point of spasm resulting in constipation. Other opioid-induced effects may include a reduction in gastric, biliary and pancreatic secretions, spasm of the sphincter of Oddi, and transient elevations in serum amylase.
Cardiovascular System
Fentanyl may produce release of histamine with or without associated peripheral vasodilation. Manifestations of histamine release and/or peripheral vasodilation may include pruritus, flushing, red eyes, sweating, and/or orthostatic hypotension.
Endocrine System
Opioid agonists have been shown to have a variety of effects on the secretion of hormones. Opioids inhibit the secretion of ACTH, cortisol, and luteinizing hormone (LH) in humans. They also stimulate prolactin, growth hormone (GH) secretion, and pancreatic secretion of insulin and glucagon in humans and other species, rats and dogs. Thyroid stimulating hormone (TSH) has been shown to be both inhibited and stimulated by opioids.
Respiratory System
All opioid mu-receptor agonists, including fentanyl, produce dose dependent respiratory depression. The risk of respiratory depression is less in patients receiving chronic opioid therapy who develop tolerance to respiratory depression and other opioid effects. During the titration phase of the clinical trials, somnolence, which may be a precursor to respiratory depression, did increase in patients who were treated with higher doses of another oral transmucosal fentanyl citrate (Actiq®). Peak respiratory depressive effects may be seen as early as 15 to 30 minutes from the start of oral transmucosal fentanyl citrate product administration and may persist for several hours.
Serious or fatal respiratory depression can occur even at recommended doses. Fentanyl depresses the cough reflex as a result of its CNS activity. Although not observed with oral transmucosal fentanyl products in clinical trials, fentanyl given rapidly by intravenous injection in large doses may interfere with respiration by causing rigidity in the muscles of respiration. Therefore, physicians and other healthcare providers should be aware of this potential complication.
(See BOXED WARNING, CONTRAINDICATIONS, WARNINGS, PRECAUTIONS, ADVERSE REACTIONS, and OVERDOSAGE for additional information on hypoventilation.)
Pharmacokinetics
Fentanyl exhibits linear pharmacokinetics. Systemic exposure to fentanyl following administration of FENTORA increases linearly in an approximate dose-proportional manner over the 100- to 800-mcg dose range.
Absorption:
Following buccal administration of FENTORA, fentanyl is readily absorbed with an absolute bioavailability of 65%. The absorption profile of FENTORA is largely the result of an initial absorption from the buccal mucosa, with peak plasma concentrations following venous sampling generally attained within an hour after buccal administration. Approximately 50% of the total dose administered is absorbed transmucosally and becomes systemically available. The remaining half of the total dose is swallowed and undergoes more prolonged absorption from the gastrointestinal tract.
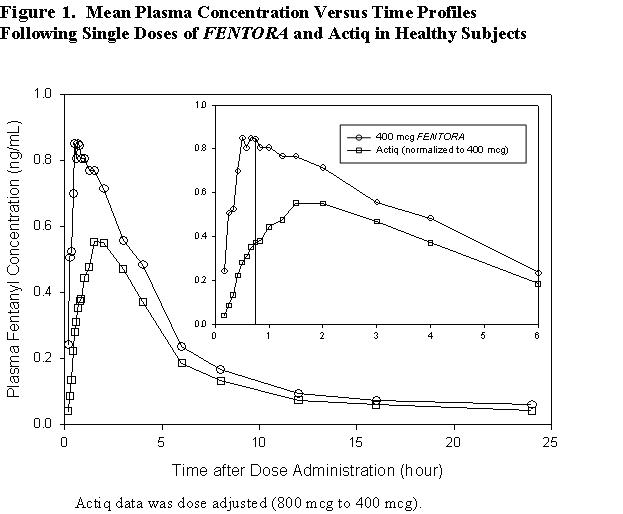
In a study that compared the absolute and relative bioavailability of FENTORA and Actiq (oral transmucosal fentanyl citrate), the rate and extent of fentanyl absorption were considerably different (approximately 30% greater exposure with FENTORA) (Table 1).
| Pharmacokinetic Parameter (mean) | FENTORA 400 mcg | Actiq 400 mcg (adjusted dose)*** |
||
|---|---|---|---|---|
| * Based on venous blood samples. | ||||
| ** Data for Tmax presented as median (range). | ||||
| *** Actiq data was dose adjusted (800 mcg to 400 mcg). | ||||
| Absolute Bioavailability | 65% ± 20% | 47% ± 10.5% | ||
| Fraction Absorbed Transmucosally | 48% ± 31.8% | 22% ± 17.3% | ||
| Tmax (minute)** | 46.8 (20-240) | 90.8 (35-240) | ||
| Cmax (ng/mL) | 1.02 ± 0.42 | 0.63 ± 0.21 | ||
| AUC0-tmax
(ng•hr/mL) | 0.40 ± 0.18 | 0.14 ± 0.05 | ||
| AUC0-inf
(ng•hr/mL) | 6.48 ± 2.98 | 4.79 ± 1.96 | ||
Similarly, in another bioavailability study exposure following administration of FENTORA was also greater (approximately 50%) compared to Actiq.
Due to differences in drug delivery, measures of exposure (Cmax, AUC0-tmax , AUC0-inf) associated with a given dose of fentanyl were substantially greater with FENTORA compared to Actiq (see Figure 1). Therefore, caution must be exercised when switching patients from one product to another. (See DOSAGE AND ADMINISTRATION.) Figure 1 includes an inset which shows the mean plasma concentration versus time profile to 6 hours. The vertical line denotes the median Tmax for FENTORA.
Systemic exposure to fentanyl following administration of FENTORA increases linearly in an approximate dose-proportional manner over the 100- to 800-mcg dose range. Mean pharmacokinetic parameters are presented in Table 2. Mean plasma concentration versus time profiles are presented in Figure 2.
| Pharmacokinetic Parameter (mean±SD) | 100 mcg | 200 mcg | 400 mcg | 800 mcg |
|---|---|---|---|---|
| * Based on venous sampling. | ||||
| ** Data for Tmax presented as median (range). | ||||
| Cmax
(ng/mL) | 0.25 ± 0.14 | 0.40 ± 0.18 | 0.97 ± 0.53 | 1.59 ± 0.90 |
| Tmax, minute** (range) | 45.0 (25.0 - 181.0) | 40.0 (20.0 - 180.0) | 35.0 (20.0 - 180.0) | 40.0 (25.0 - 180.0) |
| AUC0-inf
(ng•hr/mL) | 0.98 ± 0.37 | 2.11 ± 1.13 | 4.72 ± 1.95 | 9.05 ± 3.72 |
| AUC0-tmax
(ng•hr/mL) | 0.09 ± 0.06 | 0.13 ± 0.09 | 0.34 ± 0.23 | 0.52 ± 0.38 |
| T1/2, hr** | 2.63 (1.47 - 13.57) | 4.43 (1.85 - 20.76) | 11.09 (4.63 - 20.59) | 11.70 (4.63 - 28.63) |
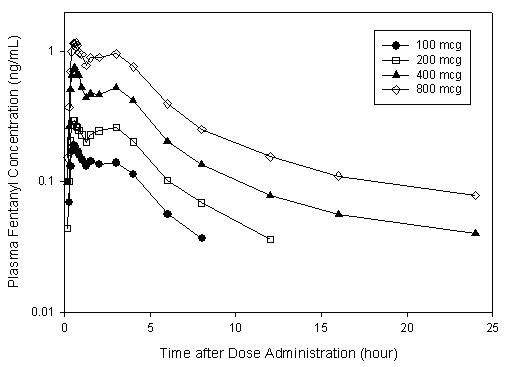
Figure 2. Mean Plasma Concentration Versus Time Profiles Following Single 100, 200, 400, and 800 mcg Doses of FENTORA in Healthy Subjects
Dwell time (defined as the length of time that the tablet takes to fully disintegrate following buccal administration), does not appear to affect early systemic exposure to fentanyl.
The effect of mucositis (Grade 1) on the pharmacokinetic profile of FENTORA was studied in a group of patients with (N = 8) and without mucositis (N = 8) who were otherwise matched. A single 200 mcg tablet was administered, followed by sampling at appropriate intervals. Mean summary statistics (standard deviation in parentheses, expected tmax where range was used) are presented in Table 3.
| Patient status | Cmax (ng/mL) | tmax (min) | AUC0-tmax
(ng•hr/mL) | AUC0-8 (ng•hr/mL) |
|---|---|---|---|---|
| Mucositis | 1.25 ± 0.78 | 25.0 (15 - 45) | 0.21 ± 0.16 | 2.33 ± 0.93 |
| No mucositis | 1.24 ± 0.77 | 22.5 (10 - 121) | 0.25 ± 0.24 | 1.86 ± 0.86 |
Distribution:
Fentanyl is highly lipophilic. The plasma protein binding of fentanyl is 80-85%. The main binding protein is alpha-1-acid glycoprotein, but both albumin and lipoproteins contribute to some extent. The mean oral volume of distribution at steady state (Vss/F) was 25.4 L/kg.
Metabolism:
The metabolic pathways following buccal administration of FENTORA have not been characterized in clinical studies. The progressive decline of fentanyl plasma concentrations results from the uptake of fentanyl in the tissues and biotransformation in the liver. Fentanyl is metabolized in the liver and in the intestinal mucosa to norfentanyl by cytochrome P450 3A4 isoform. In animal studies, norfentanyl was not found to be pharmacologically active. (See PRECAUTIONS: Drug Interactions for additional information.)
Elimination:
Disposition of fentanyl following buccal administration of FENTORA has not been characterized in a mass balance study. Fentanyl is primarily (more than 90%) eliminated by biotransformation to N-dealkylated and hydroxylated inactive metabolites. Less than 7% of the administered dose is excreted unchanged in the urine, and only about 1% is excreted unchanged in the feces. The metabolites are mainly excreted in the urine, while fecal excretion is less important.
The total plasma clearance of fentanyl following intravenous administration is approximately 42 L/h.
Special Populations:
The pharmacokinetics of FENTORA has not been studied in Special Populations.
Race
The pharmacokinetic effects of race with the use of FENTORA have not been systematically evaluated. In studies conducted in healthy Japanese subjects, systemic exposure was generally higher than that observed in US subjects (mean Cmax and AUC values were approximately 50% and 20% higher, respectively). The observed differences were largely attributed to the lower mean weight of the Japanese subjects compared to US subjects (57.4 kg versus 73 kg).
Age
The effect of age on the pharmacokinetics of FENTORA has not been studied.
Gender
Systemic exposure was higher for women than men (mean Cmax and AUC values were approximately 28% and 22% higher, respectively). The observed differences between men and women were largely attributable to differences in weight.
Renal or Hepatic Impairment:
The effect of renal or hepatic impairment on the pharmacokinetics of FENTORA has not been studied. Although fentanyl kinetics are known to be altered as a result of hepatic and renal disease due to alterations in metabolic clearance and plasma protein binding, the duration of effect for the initial dose of fentanyl is largely determined by the rate of distribution of the drug.
Diminished metabolic clearance may, therefore, become significant, primarily with repeated dosing or at very high single doses. For these reasons, while it is recommended that FENTORA is titrated to clinical effect for all patients, special care should be taken in patients with severe hepatic or renal disease. (See PRECAUTIONS.)
Drug Interactions
The interaction between ritonavir and fentanyl was investigated in eleven healthy volunteers in a randomized crossover study. Subjects received oral ritonavir or placebo for 3 days. The ritonavir dose was 200 mg tid on Day 1 and 300 mg tid on Day 2 followed by one morning dose of 300 mg on Day 3. On Day 2, fentanyl was given as a single IV dose at 5 mcg/kg two hours after the afternoon dose of oral ritonavir or placebo. Naloxone was administered to counteract the side effects of fentanyl. The results suggested that ritonavir might decrease the clearance of fentanyl by 67%, resulting in a 174% (range 52%-420%) increase in fentanyl AUC0-inf. Coadministration of ritonavir in patients receiving FENTORA has not been studied; however, an increase in fentanyl AUC is expected. (See DOSAGE AND ADMINISTRATION and PRECAUTIONS.)
CLINICAL TRIALS
Breakthrough Pain:
The efficacy of FENTORA was demonstrated in a double-blind, placebo-controlled, cross-over study in opioid tolerant patients with cancer and breakthrough pain. Patients considered opioid tolerant were those who were taking at least 60 mg of oral morphine/day, at least 25 mcg of transdermal fentanyl/hour, at least 30 mg of oxycodone daily, at least 8 mg of oral hydromorphone daily or an equianalgesic dose of another opioid for a week or longer.
In this trial, patients were titrated in an open-label manner to a successful dose of FENTORA. A successful dose was defined as the dose in which a patient obtained adequate analgesia with tolerable side effects. Patients who identified a successful dose were randomized to a sequence of 10 treatments with 7 being the successful dose of FENTORA and 3 being placebo. Patients used one tablet (either FENTORA or Placebo) per breakthrough pain episode.
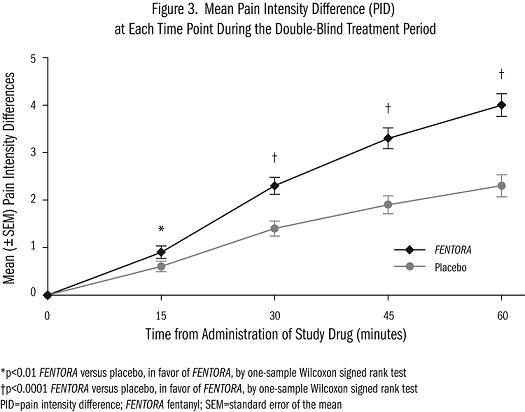
Patients assessed pain intensity on a scale that rated the pain as 0=none to 10=worst possible pain. With each episode of breakthrough pain, pain intensity was assessed first and then treatment was administered. Pain intensity (0-10) was measured at 15, 30, 45 and 60 minutes after the start of administration. The sum of differences in pain intensity scores at 15 and 30 minutes from baseline (SPID30) was the primary efficacy measure.
Sixty five percent of patients who entered the study achieved a successful dose during the titration phase. The distribution of successful doses is shown in Table 4. The median dose was 400 mcg.
| FENTORA Dose | (N=80) n(%) |
|---|---|
| 100 mcg | 13 (16) |
| 200 mcg | 11 (14) |
| 400 mcg | 21 (26) |
| 600 mcg | 10 (13) |
| 800 mcg | 25 (31) |
The LS mean (SE) SPID30 for FENTORA-treated episodes was 3.0 (0.12) while for placebo-treated episodes it was 1.8 (0.18) (p<0.0001).
INDICATIONS AND USAGE
(See BOXED WARNING and CONTRAINDICATIONS.)
FENTORA is indicated only for the management of breakthrough pain in patients with cancer who are already receiving and who are tolerant to around-the-clock opioid therapy for their underlying persistent cancer pain. Patients considered opioid tolerant are those who are taking around-the-clock medicine consisting of at least 60 mg of oral morphine daily, at least 25 mcg of transdermal fentanyl/hour, at least 30 mg of oxycodone daily, at least 8 mg of oral hydromorphone daily or an equianalgesic dose of another opioid daily for a week or longer.
This product must not be used in opioid non-tolerant patients because life-threatening hypoventilation and death could occur at any dose in patients not on a chronic regimen of opioids. For this reason, FENTORA is contraindicated in the management of acute or postoperative pain.
FENTORA is intended to be used only in the care of opioid tolerant cancer patients and only by healthcare professionals who are knowledgeable of and skilled in the use of Schedule II opioids to treat cancer pain.
CONTRAINDICATIONS
FENTORA is contraindicated in opioid non-tolerant patients. FENTORA is contraindicated in the management of acute or postoperative pain including headache/migraine. Life-threatening respiratory depression and death could occur at any dose in opioid non-tolerant patients.
FENTORA is contraindicated in patients with known intolerance or hypersensitivity to any of its components or the drug fentanyl.
WARNINGS
See BOXED WARNING
When prescribing, DO NOT convert a patient from Actiq to FENTORA without following the instructions found in the prescribing information as Actiq andFENTORA are not equivalent on a microgram per microgram basis. FENTORA is NOT a generic version of Actiq.
When dispensing, DO NOT substitute a FENTORA prescription for an Actiq prescription under any circumstances. FENTORA and Actiq are not equivalent. Substantial differences exist in the pharmacokinetic profile of FENTORA compared to other fentanyl products including Actiq that result in clinically important differences in the rate and extent of absorption of fentanyl. As a result of these differences, the substitution of the same dose of FENTORA for the same dose of Actiq or any other fentanyl product may result in a fatal overdose.
There are no safe conversion directions available for patients on any other fentanyl products. (Note: This includes oral, transdermal, or parenteral formulations of fentanyl.) Therefore, for opioid tolerant patients, the initial dose of FENTORA should be 100 mcg. Each patient should be individually titrated to provide adequate analgesia while minimizing side effects. (See DOSAGE AND ADMINISTRATION.)
Use with CNS Depressants
The concomitant use of other CNS depressants, including other opioids, sedatives or hypnotics, general anesthetics, phenothiazines, tranquilizers, skeletal muscle relaxants, sedating antihistamines, potent inhibitors of cytochrome P450 3A4 isoform (e.g., erythromycin, ketoconazole, and certain protease inhibitors), and alcoholic beverages may produce increased depressant effects. Hypoventilation, hypotension, and profound sedation may occur.
FENTORA is not recommended for use in patients who have received MAO inhibitors within 14 days, because severe and unpredictable potentiation by MAO inhibitors has been reported with opioid analgesics.
Pediatric Use:
The safety and efficacy of FENTORA have not been established in pediatric patients below the age of 18 years.
Patients and their caregivers must be instructed that FENTORA contains a medicine in an amount which can be fatal to a child. Patients and their caregivers must be instructed to keep tablets out of the reach of children. (See SAFETY AND HANDLING, PRECAUTIONS, and MEDICATION GUIDE for specific patient instructions.)
Drug Abuse, Addiction and Diversion of Opioids
FENTORA contains fentanyl, a mu-opioid agonist and a Schedule II controlled substance with high potential for abuse similar to hydromorphone, methadone, morphine, oxycodone, and oxymorphone. Fentanyl can be abused and is subject to misuse, and criminal diversion.
Concerns about abuse, addiction, and diversion should not prevent the proper management of pain. However, all patients treated with opioids require careful monitoring for signs of abuse and addiction, since use of opioid analgesic products carries the risk of addiction even under appropriate medical use.
Addiction is a primary, chronic, neurobiologic disease, with genetic, psychosocial, and environmental factors influencing its development and manifestations. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving. Drug addiction is a treatable disease, utilizing a multidisciplinary approach, but relapse is common.
“Drug-seeking” behavior is very common in addicts and drug abusers. FENTORA should be prescribed with caution to patients who have a higher risk of substance abuse, including patients with bipolar disorder and/or schizophrenia.
Patients with chronic pain may be at a higher risk for suicide.
Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of addiction and is characterized by misuse for non-medical purposes, often in combination with other psychoactive substances. Since FENTORA tablets may be diverted for non-medical use, careful record keeping of prescribing information, including quantity, frequency, and renewal requests is strongly advised.
Proper assessment of patients, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
FENTORA should be handled appropriately to minimize the risk of diversion, including restriction of access and accounting procedures as appropriate to the clinical setting and as required by law.
Healthcare professionals should contact their State Professional Licensing Board, or State Controlled Substances Authority for information on how to prevent and detect abuse or diversion of this product.
Physical Dependence and Withdrawal
The administration of FENTORA should be guided by the response of the patient. Physical dependence, per se, is not ordinarily a concern when one is treating a patient with cancer and chronic pain, and fear of tolerance and physical dependence should not deter using doses that adequately relieve the pain.
Opioid analgesics may cause physical dependence. Physical dependence results in withdrawal symptoms in patients who abruptly discontinue the drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity, e.g., naloxone, nalmefene, or mixed agonist/antagonist analgesics (pentazocine, butorphanol, buprenorphine, nalbuphine).
Physical dependence usually does not occur to a clinically significant degree until after several weeks of continued opioid usage. Tolerance, in which increasingly larger doses are required in order to produce the same degree of analgesia, is initially manifested by a shortened duration of analgesic effect, and subsequently, by decreases in the intensity of analgesia.
Respiratory Depression
Respiratory depression is the chief hazard of opioid agonists, including fentanyl, the active ingredient in FENTORA. Respiratory depression is more likely to occur in patients with underlying respiratory disorders and elderly or debilitated patients, usually following large initial doses in opioid non-tolerant patients, or when opioids are given in conjunction with other drugs that depress respiration.
Respiratory depression from opioids is manifested by a reduced urge to breathe and a decreased rate of respiration, often associated with the “sighing” pattern of breathing (deep breaths separated by abnormally long pauses). Carbon dioxide retention from opioid-induced respiratory depression can exacerbate the sedating effects of opioids. This makes overdoses involving drugs with sedative properties and opioids especially dangerous.
PRECAUTIONS
General
Opioid analgesics impair the mental and/or physical ability required for the performance of potentially dangerous tasks (e.g., driving a car or operating machinery). Patients taking FENTORA should be warned of these dangers and should be counseled accordingly.
The use of concomitant CNS active drugs requires special patient care and observation. (See WARNINGS.)
Chronic Pulmonary Disease
Because potent opioids can cause respiratory depression, FENTORA should be titrated with caution in patients with chronic obstructive pulmonary disease or pre-existing medical conditions predisposing them to respiratory depression. In such patients, even normal therapeutic doses of FENTORA may further decrease respiratory drive to the point of respiratory failure.
Head Injuries and Increased Intracranial Pressure
FENTORA should only be administered with extreme caution in patients who may be particularly susceptible to the intracranial effects of CO2 retention such as those with evidence of increased intracranial pressure or impaired consciousness. Opioids may obscure the clinical course of a patient with a head injury and should be used only if clinically warranted.
Application Site Reactions
In clinical trials, 10% of all patients exposed to FENTORA reported application site reactions. These reactions ranged from paresthesia to ulceration and bleeding. Application site reactions occurring in ≥1% of patients were pain (4%), ulcer (3%), and irritation (3%). Application site reactions tended to occur early in treatment, were self-limited and only resulted in treatment discontinuation for 2% of patients.
Cardiac Disease
Intravenous fentanyl may produce bradycardia. Therefore, FENTORA should be used with caution in patients with bradyarrhythmias.
Hepatic or Renal Disease
Insufficient information exists to make recommendations regarding the use of FENTORA in patients with impaired renal or hepatic function. Fentanyl is metabolized primarily via human cytochrome P450 3A4 isoenzyme system and mostly eliminated in urine. If the drug is used in these patients, it should be used with caution because of the hepatic metabolism and renal excretion of fentanyl.
Information for Patients and Caregivers
- Patients and their caregivers must be instructed that children, especially small children, exposed to FENTORA are at high risk of FATAL RESPIRATORY DEPRESSION. Patients and their caregivers must be instructed to keep FENTORA tablets out of the reach of children. (See SAFETY AND HANDLING, WARNINGS, and MEDICATION GUIDE for specific patient instructions.)
- Patients and their caregivers must be provided a Medication Guide each time FENTORA is dispensed because new information may be available.
- Patients must be instructed not to take FENTORA for acute pain, postoperative pain, pain from injuries, headache, migraine or any other short term pain, even if they have taken other opioid analgesics for these conditions.
- Patients must be instructed on the meaning of opioid tolerance and that FENTORA is only to be used as a supplemental pain medication for patients with pain requiring around-the-clock opioids, who have developed tolerance to the opioid medication, and who need additional opioid treatment of breakthrough pain episodes.
- Patients must be instructed that, if they are not taking an opioid medication on a scheduled basis (around-the-clock), they should not take FENTORA.
- Patients should be instructed that the titration phase is the only period in which they may take more than ONE tablet to achieve a desired dose (e.g., two 100 mcg tablets for a 200 mcg dose).
- Patients must be instructed that, if the breakthrough pain episode is not relieved after 30 minutes, they may take ONLY ONE ADDITIONAL DOSE OF FENTORA USING THE SAME STRENGTH FOR THAT EPISODE. Thus, patients should take a maximum of two doses of FENTORA for any breakthrough pain episode.
- Patients must be instructed that they MUST wait at least 4 hours before treating another episode of breakthrough pain with FENTORA.
- Patients must be instructed NOT to share FENTORA and that sharing FENTORA with anyone else could result in the other individual’s death due to overdose.
- Patients must be aware that FENTORA contains fentanyl which is a strong pain medication similar to hydromorphone, methadone, morphine, oxycodone, and oxymorphone.
- Patients must be instructed that the active ingredient in FENTORA, fentanyl, is a drug that some people abuse. FENTORA should be taken only by the patient it was prescribed for, and it should be protected from theft or misuse in the work or home environment.
- Patients should be instructed that FENTORA tablets are not to be swallowed whole; this will reduce the effectiveness of the medication. Tablets are to be placed between the cheek and gum above a molar tooth and allowed to dissolve. After 30 minutes if remnants of the tablet still remain, patients may swallow it with a glass of water.
- Patients must be cautioned to talk to their doctor if breakthrough pain is not alleviated or worsens after taking FENTORA.
- Patients must be instructed to use FENTORA exactly as prescribed by their doctor and not to take FENTORA more often than prescribed.
- Patients must be cautioned that FENTORA can affect a person’s ability to perform activities that require a high level of attention (such as driving or using heavy machinery). Patients taking FENTORA should be warned of these dangers and counseled accordingly.
- Patients must be warned to not combine FENTORA with alcohol, sleep aids, or tranquilizers except by the orders of the prescribing physician, because dangerous additive effects may occur, resulting in serious injury or death.
- Female patients must be informed that if they become pregnant or plan to become pregnant during treatment with FENTORA, they should ask their doctor about the effects that FENTORA (or any medicine) may have on them and their unborn children.
- Patients and caregivers must be advised that if they have been receiving treatment with FENTORA and the medicine is no longer needed they should flush any remaining product down the toilet, and if they then need further assistance, contact Cephalon at 1-800-896-5855.
Disposal of Unopened FENTORA Blister Packages When No Longer Needed
Patients and members of their household must be advised to dispose of any unopened blister packages remaining from a prescription as soon as they are no longer needed.
To dispose of unused FENTORA, remove FENTORA tablets from blister packages and flush down the toilet. Do not flush the FENTORA blister packages or cartons down the toilet. (See SAFETY AND HANDLING.)
Detailed instructions for the proper storage, administration, disposal, and important instructions for managing an overdose of FENTORA are provided in the FENTORA Medication Guide. Patients should be encouraged to read this information in its entirety and be given an opportunity to have their questions answered.
In the event that a caregiver requires additional assistance in disposing of excess unusable tablets that remain in the home after a patient has expired, they should be instructed to call the Cephalon toll-free number (1-800-896-5855) or seek assistance from their local DEA office.
Laboratory Tests
The effects of FENTORA on laboratory tests have not been evaluated.
Drug Interactions
See WARNINGS.
Fentanyl is metabolized mainly via the human cytochrome P450 3A4 isoenzyme system (CYP3A4); therefore potential interactions may occur when FENTORA is given concurrently with agents that affect CYP3A4 activity. The concomitant use of FENTORA with strong CYP3A4 inhibitors (e.g., ritonavir, ketoconazole, itraconazole, troleandomycin, clarithromycin, nelfinavir, and nefazadone) or moderate CYP3A4 inhibitors (e.g., amprenavir, aprepitant, diltiazem, erythromycin, fluconazole, fosamprenavir, and verapamil) may result in increased fentanyl plasma concentrations, potentially causing serious adverse drug effects including fatal respiratory depression. Patients receiving FENTORA concomitantly with moderate or strong CYP 3A4 inhibitors should be carefully monitored for an extended period of time. Dosage increase should be done conservatively. (See PHARMACOKINETICS, Drug Interactions and DOSAGE AND ADMINISTRATION.)
Grapefruit and grapefruit juice decrease CYP3A4 activity, increasing blood concentrations of fentanyl, thus should be avoided.
Drugs that induce cytochrome P450 3A4 activity may have the opposite effects.
Concomitant use of FENTORA with an MAO inhibitor, or within 14 days of discontinuation, is not recommended.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Long-term studies in animals have not been performed to evaluate the carcinogenic potential of fentanyl.
Fentanyl citrate was not mutagenic in the in vitro Ames reverse mutation assay in S. tymphimurium or E. coli, or the mouse lymphoma mutagenesis assay. Fentanyl citrate was not clastogenic in the in vivo mouse micronucleus assay.
Fentanyl impairs fertility in rats at doses of 30 mcg/kg IV and 160 mcg/kg SC. Conversion to human equivalent doses indicates this is within the range of the human recommended dosing for FENTORA.
Pregnancy - Category C
There are no adequate and well-controlled studies in pregnant women. FENTORA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. No epidemiological studies of congenital anomalies in infants born to women treated with fentanyl during pregnancy have been reported.
Chronic maternal treatment with fentanyl during pregnancy has been associated with transient respiratory depression, behavioral changes, or seizures characteristic of neonatal abstinence syndrome in newborn infants. Symptoms of neonatal respiratory or neurological depression were no more frequent than expected in most studies of infants born to women treated acutely during labor with intravenous or epidural fentanyl. Transient neonatal muscular rigidity has been observed in infants whose mothers were treated with intravenous fentanyl.
Fentanyl is embryocidal as evidenced by increased resorptions in pregnant rats at doses of 30 mcg/kg IV or 160 mcg/kg SC. Conversion to human equivalent doses indicates this is within the range of the human recommended dosing for FENTORA.
Fentanyl citrate was not teratogenic when administered to pregnant animals. Published studies demonstrated that administration of fentanyl (10, 100, or 500 mcg/kg/day) to pregnant rats from day 7 to 21, of their 21 day gestation, via implanted microosmotic minipumps was not teratogenic (the high dose was approximately 3-times the human dose of 1600 mcg per pain episode on a mg/m2 basis). Intravenous administration of fentanyl (10 or 30 mcg/kg) to pregnant female rats from gestation day 6 to 18, was embryo or fetal toxic, and caused a slightly increased mean delivery time in the 30 mcg/kg/day group, but was not teratogenic.
Labor and Delivery
Fentanyl readily passes across the placenta to the fetus; therefore FENTORA is not recommended for analgesia during labor and delivery.
Nursing Mothers
Fentanyl is excreted in human milk; therefore FENTORA should not be used in nursing women because of the possibility of sedation and/or respiratory depression in their infants. Symptoms of opioid withdrawal may occur in infants at the cessation of nursing by women using FENTORA.
Pediatric Use
See WARNINGS.
Geriatric Use
Of the 304 patients with cancer in clinical studies of FENTORA, 69 (23%) were 65 years of age and older.
Patients over the age of 65 years tended to titrate to slightly lower doses than younger patients.
Patients over the age of 65 years reported a slightly higher frequency for some adverse events specifically vomiting, constipation, and abdominal pain. Therefore, caution should be exercised in individually titrating FENTORA in elderly patients to provide adequate efficacy while minimizing risk.
ADVERSE REACTIONS
Pre-Marketing Clinical Trial Experience
The safety of FENTORA has been evaluated in 304 opioid tolerant cancer patients with breakthrough pain. The average duration of therapy was 76 days with some patients being treated for over 12 months.
The most commonly observed adverse events seen with FENTORA are typical of opioid side effects. Opioid side effects should be expected and managed accordingly.
The clinical trials of FENTORA were designed to evaluate safety and efficacy in treating patients with cancer and breakthrough pain; all patients were taking concomitant opioids, such as sustained-release morphine, sustained-release oxycodone or transdermal fentanyl, for their persistent pain.
The adverse event data presented here reflect the actual percentage of patients experiencing each adverse effect among patients who received FENTORA for breakthrough pain along with a concomitant opioid for persistent pain. There has been no attempt to correct for concomitant use of other opioids, duration of FENTORA therapy or cancer-related symptoms.
Table 5 lists, by maximum dose received, adverse events with an overall frequency of 5% or greater within the total population that occurred during titration. The ability to assign a dose-response relationship to these adverse events is limited by the titration schemes used in these studies.
| System Organ Class MeDRA preferred term, n (%) | 100 mcg (N=45) | 200 mcg (N=34) | 400 mcg (N=53) | 600 mcg (N=56) | 800 mcg (N=113) | Total (N=304)* |
|
|---|---|---|---|---|---|---|---|
| * Three hundred and two (302) patients were included in the safety analysis. | |||||||
| Gastrointestinal disorders | |||||||
| Nausea | 4 (9) | 5 (15) | 10 (19) | 13 (23) | 18 (16) | 50 (17) | |
| Vomiting | 0 | 2 (6) | 2 (4) | 7 (13) | 3 (3) | 14 (5) | |
| General disorders and administration site conditions | |||||||
| Fatigue | 3 (7) | 1 (3) | 9 (17) | 1 (2) | 5 (4) | 19 (6) | |
| Nervous system disorders | |||||||
| Dizziness | 5 (11) | 2 (6) | 12 (23) | 18 (32) | 21 (19) | 58 (19) | |
| Somnolence | 2 (4) | 2 (6) | 6 (12) | 7 (13) | 3 (3) | 20 (7) | |
| Headache | 1 (2) | 3 (9) | 4 (8) | 8 (14) | 10 (9) | 26 (9) | |
Table 6 lists, by successful dose, adverse events with an overall frequency of ≥ 5% within the total population that occurred after a successful dose had been determined.
| System Organ Class MeDRA preferred term, n (%) | 100 mcg (N=19) | 200 mcg (N=31) | 400 mcg (N=44) | 600 mcg (N=48) | 800 mcg (N=58) | Total (N=200) |
|
|---|---|---|---|---|---|---|---|
| Blood and lymphatic system disorders | |||||||
| Anemia | 6 (32) | 4 (13) | 4 (9) | 5 (10) | 7 (13) | 26 (13) | |
| Neutropenia | 0 | 2 (6) | 1 (2) | 4 (8) | 4 (7) | 11 (6) | |
| Gastrointestinal disorders | |||||||
| Nausea | 8 (42) | 5 (16) | 14 (32) | 13 (27) | 17 (31) | 57 (29) | |
| Vomiting | 7 (37) | 5 (16) | 9 (20) | 8 (17) | 11 (20) | 40 (20) | |
| Constipation | 5 (26) | 4 (13) | 5 (11) | 4 (8) | 6 (11) | 24 (12) | |
| Diarrhea | 3 (16) | 0 | 4 (9) | 3 (6) | 5 (9) | 15 (8) | |
| Abdominal pain | 2 (11) | 1 (3) | 4 (9) | 7 (15) | 4 (7) | 18 (9) | |
| General disorders and administration site conditions | |||||||
| Edema peripheral | 6 (32) | 5 (16) | 4 (9) | 5 (10) | 3 (5) | 23 (12) | |
| Asthenia | 3 (16) | 5 (16) | 2 (5) | 3 (6) | 8 (15) | 21 (11) | |
| Fatigue | 3 (16) | 3 (10) | 9 (20) | 9 (19) | 8 (15) | 32 (16) | |
| Infections and infestations | |||||||
| Pneumonia | 1 (5) | 5 (16) | 1 (2) | 1 (2) | 4 (7) | 12 (6) | |
| Investigations | |||||||
| Weight decreased | 1 (5) | 1 (3) | 3 (7) | 2 (4) | 6 (11) | 13 (7) | |
| Metabolism and nutrition disorders | |||||||
| Dehydration | 4 (21) | 0 | 4 (9) | 6 (13) | 7 (13) | 21 (11) | |
| Anorexia | 1 (5) | 2 (6) | 4 (9) | 3 (6) | 6 (11) | 16 (8) | |
| Hypokalemia | 0 | 2 (6) | 0 | 1 (2) | 8 (15) | 11 (6) | |
| Musculoskeletal and connective tissue disorders | |||||||
| Back pain | 2 (11) | 0 | 2 (5) | 3 (6) | 2 (4) | 9 (5) | |
| Arthralgia | 0 | 1 (3) | 3 (7) | 4 (8) | 3 (5) | 11 (6) | |
| Neoplasms benign, malignant and unspecified (including cysts and polyps) | |||||||
| Cancer pain | 3 (16) | 1 (3) | 3 (7) | 2 (4) | 1 (2) | 10 (5) | |
| Nervous system disorders | |||||||
| Dizziness | 5 (26) | 3 (10) | 5 (11) | 6 (13) | 6 (11) | 25 (13) | |
| Headache | 2 (11) | 1 (3) | 4 (9) | 5 (10) | 8 (15) | 20 (10) | |
| Somnolence | 0 | 1 (3) | 4 (9) | 4 (8) | 8 (15) | 17 (9) | |
| Psychiatric disorders | |||||||
| Confusional state | 3 (16) | 1 (3) | 2 (5) | 3 (6) | 5 (9) | 14 (7) | |
| Depression | 2 (11) | 1 (3) | 4 (9) | 3 (6) | 5 (9) | 15 (8) | |
| Insomnia | 2 (11) | 1 (3) | 3 (7) | 2 (4) | 4 (7) | 12 (6) | |
| Respiratory, thoracic, and mediastinal disorders | |||||||
| Cough | 1 (5) | 1 (3) | 2 (5) | 4 (8) | 5 (9) | 13 (7) | |
| Dyspnea | 1 (5) | 6 (19) | 0 | 7 (15) | 4 (7) | 18 (9) | |
In addition, a small number of patients (n=11) with Grade 1 mucositis were included in clinical trials designed to support the safety of FENTORA. There was no evidence of excess toxicity in this subset of patients.
The duration of exposure to FENTORA varied greatly, and included open-label and double-blind studies. The frequencies listed below represent the ≥1% of patients from three clinical trials (titration and post-titration periods combined) who experienced that event while receiving FENTORA. Events are classified by system organ class.
Adverse Events (≥1%)
Blood and Lymphatic System Disorders: Anemia, Neutropenia, Thrombocytopenia, Leukopenia
Cardiac Disorders: Tachycardia
Gastrointestinal Disorders: Nausea, Vomiting, Constipation, Abdominal Pain, Diarrhea, Stomatitis, Dry Mouth, Dyspepsia, Upper Abdominal Pain, Abdominal Distension, Dysphagia, Gingival Pain, Stomach Discomfort, Gastroesophageal Reflux Disease, Glossodynia, Mouth Ulceration
General Disorders and Administration Site Conditions: Fatigue, Edema Peripheral, Asthenia, Pyrexia, Application Site Pain, Application Site Ulcer, Chest Pain, Chills, Application Site Irritation, Edema, Mucosal Inflammation, Pain
Hepatobiliary Disorders: Jaundice
Infections and Infestations: Pneumonia, Oral Candidiasis, Urinary Tract Infection, Cellulitis, Nasopharyngitis, Sinusitis, Upper Respiratory Tract Infection, Influenza, Tooth Abscess
Injury, Poisoning and Procedural Complications: Fall, Spinal Compression Fracture
Investigations: Decreased Weight, Decreased Hemoglobin, Increased Blood Glucose, Decreased Hematocrit, Decreased Platelet Count
Metabolism and Nutrition Disorders: Dehydration, Anorexia, Hypokalemia, Decreased Appetite, Hypoalbuminemia, Hypercalcemia, Hypomagnesemia, Hyponatremia, Reduced Oral Intake
Musculoskeletal and Connective Tissue Disorders: Arthralgia, Back Pain, Pain in Extremity, Myalgia, Chest Wall Pain, Muscle Spasms, Neck Pain, Shoulder Pain
Nervous System Disorders: Dizziness, Headache, Somnolence, Hypoesthesia, Dysgeusia, Lethargy, Peripheral Neuropathy, Paresthesia, Balance Disorder, Migraine, Neuropathy
Psychiatric Disorders: Confusional State, Depression, Insomnia, Anxiety, Disorientation, Euphoric Mood, Hallucination, Nervousness
Renal and Urinary Disorders: Renal Failure
Respiratory, Thoracic and Mediastinal Disorders: Dyspnea, Cough, Pharyngolaryngeal Pain, Exertional Dyspnea, Pleural Effusion, Decreased Breathing Sounds, Wheezing
Skin and Subcutaneous Tissue Disorders: Pruritus, Rash, Hyperhidrosis, Cold Sweat
Vascular Disorders: Hypertension, Hypotension, Pallor, Deep Vein Thrombosis
OVERDOSAGE
Clinical Presentation
The manifestations of FENTORA overdosage are expected to be similar in nature to intravenous fentanyl and other opioids, and are an extension of its pharmacological actions with the most serious significant effect being hypoventilation. (See CLINICAL PHARMACOLOGY.)
General
Immediate management of opioid overdose includes removal of the FENTORA tablet, if still in the mouth, ensuring a patent airway, physical and verbal stimulation of the patient, and assessment of level of consciousness, as well as ventilatory and circulatory status.
Treatment of Overdosage in the Opioid Non-Tolerant Person
Ventilatory support should be provided, intravenous access obtained, and naloxone or other opioid antagonists should be employed as clinically indicated. The duration of respiratory depression following overdose may be longer than the effects of the opioid antagonist’s action (e.g., the half-life of naloxone ranges from 30 to 81 minutes) and repeated administration may be necessary. Consult the package insert of the individual opioid antagonist for details about such use.
Treatment of Overdose in Opioid-Tolerant Patients
Ventilatory support should be provided and intravenous access obtained as clinically indicated. Judicious use of naloxone or another opioid antagonist may be warranted in some instances, but it is associated with the risk of precipitating an acute withdrawal syndrome.
General Considerations for Overdose
Management of severe FENTORA overdose includes: securing a patent airway, assisting or controlling ventilation, establishing intravenous access, and GI decontamination by lavage and/or activated charcoal, once the patient’s airway is secure. In the presence of hypoventilation or apnea, ventilation should be assisted or controlled and oxygen administered as indicated.
Patients with overdose should be carefully observed and appropriately managed until their clinical condition is well controlled.
Although muscle rigidity interfering with respiration has not been seen following the use of FENTORA, this is possible with fentanyl and other opioids. If it occurs, it should be managed by the use of assisted or controlled ventilation, by an opioid antagonist, and as a final alternative, by a neuromuscular blocking agent.
DOSAGE AND ADMINISTRATION
Physicians should individualize treatment using a progressive plan of pain management. Healthcare professionals should follow appropriate pain management principles of careful assessment and ongoing monitoring. (See BOXED WARNING and Dosing.)
It is important to minimize the number of strengths available to patients at any time to prevent confusion and possible overdose.
Dosing
-
Initial Dose
- For opioid-tolerant patients not being converted from Actiq, the initial dose of FENTORA is always 100 mcg.
- For patients being converted from Actiq, prescribers must use the Initial Dosing Recommendations table below (Table 7). The doses of FENTORA in this table are starting doses and not intended to represent equianalgesic doses to Actiq. Patients must be instructed to stop the use of Actiq and dispose of any remaining units.
Table 7. Initial Dosing Recommendations for Patients on Actiq Current Actiq Dose
(mcg)Initial FENTORA Dose
(mcg)200 100 mcg tablet 400 100 mcg tablet 600 200 mcg tablet 800 200 mcg tablet 1200 2 x 200 mcg tablets 1600 2 x 200 mcg tablets - For patients converting from Actiq doses equal to or greater than 600 mcg, titration should be initiated with the 200 mcg FENTORA tablet and should proceed using multiples of this tablet strength.
- In cases where the breakthrough pain episode is not relieved after 30 minutes, patients may take ONLY ONE additional dose using the same strength for that episode. Thus patients should take a maximum of two doses of FENTORA for any episode of breakthrough pain.
- Patients MUST wait at least 4 hours before treating another episode of breakthrough pain with FENTORA.
-
Titration
- From an initial dose, patients should be closely followed by the prescriber and the dosage strength changed until the patient reaches a dose that provides adequate analgesia with tolerable side effects. Patients should record their use of FENTORA over several episodes of breakthrough pain and discuss their experience with their physician to determine if a dosage adjustment is warranted.
- Patients whose initial dose is 100 mcg and who need to titrate to a higher dose, can be instructed to use two 100-mcg tablets (one on each side of the mouth in the buccal cavity) with their next breakthrough pain episode. If this dosage is not successful, the patient may be instructed to place two 100-mcg tablets on each side of the mouth in the buccal cavity (total of four 100-mcg tablets). Titrate using multiples of the 200-mcg FENTORA tablet for doses above 400 mcg (600 mcg and 800 mcg). Note: Do not use more than 4 tablets simultaneously.
- In cases where the breakthrough pain episode is not relieved after 30 minutes, patients may take ONLY ONE additional dose of the same strength for that episode. Thus patients should take a maximum of two doses of FENTORA for any breakthrough pain episode. During titration, one dose of FENTORA may include administration of 1 to 4 tablets of the same dosage strength (100 mcg or 200 mcg).
- Patients MUST wait at least 4 hours before treating another episode of breakthrough pain with FENTORA. To reduce the risk of overdosing during titration, patients should have only one strength of FENTORA tablets available at any one time.
- Patients should be strongly encouraged to use all of their FENTORA tablets of one strength prior to being prescribed the next strength. If this is not practical, unused FENTORA should be disposed of safely. (See DISPOSAL OF FENTORA.) Dispose of any unopened FENTORA tablets remaining from a prescription as soon as they are no longer needed.
-
Maintenance Dosing
- Once titrated to an effective dose, patients should generally use only ONE FENTORA tablet of the appropriate strength per breakthrough pain episode.
- On occasion when the breakthrough pain episode is not relieved after 30 minutes, patients may take ONLY ONE additional dose using the same strength for that episode.
- Patients MUST wait at least 4 hours before treating another episode of breakthrough pain with FENTORA.
- Dosage adjustment of FENTORA may be required in some patients in order to continue to provide adequate relief of breakthrough pain.
Generally, the FENTORA dose should be increased only when a single administration of the current dose fails to adequately treat the breakthrough pain episode for several consecutive episodes.
If the patient experiences greater than four breakthrough pain episodes per day, the dose of the maintenance (around-the-clock) opioid used for persistent pain should be re-evaluated.
Patients With Hepatic and/or Renal Impairment
Caution should be exercised for patients with hepatic and/or renal impairment, and the lowest possible dose should be used in these patients. (See PRECAUTIONS.)
Patients Receiving CYP3A4 Inhibitors
Particular caution should be exercised for patients receiving CYP3A4 inhibitors, and the lowest possible dose should be used in these patients. (See PRECAUTIONS.)
Patients With Mucositis
No dose adjustment appears necessary in patients with Grade 1 mucositis. The safety and efficacy of FENTORA when used in patients with mucositis more severe than Grade 1 have not been studied.
Opening the Blister Package
- Patients should be instructed not to open the blister until ready to administer FENTORA.
- A single blister unit should be separated from the blister card by bending and tearing apart at the perforations.
- The blister unit should then be bent along the line where indicated.
- The blister backing should then be peeled back to expose the tablet. Patients should NOT attempt to push the tablet through the blister as this may cause damage to the tablet.
- The tablet should not be stored once it has been removed from the blister package as the tablet integrity may be compromised, and more importantly, because this increases the risk of accidental exposure to the tablet.
Tablet Administration
Once the tablet is removed from the blister unit, the patient should immediately place the entire FENTORA tablet in the buccal cavity (above a rear molar, between the upper cheek and gum). Patients should not split the tablet.
The FENTORA tablet should not be sucked, chewed or swallowed, as this will result in lower plasma concentrations than when taken as directed.
The FENTORA tablet should be left between the cheek and gum until it has disintegrated, which usually takes approximately 14-25 minutes.
After 30 minutes, if remnants from the FENTORA tablet remain, they may be swallowed with a glass of water.
It is recommended that patients alternate sides of the mouth when administering subsequent doses of FENTORA.
SAFETY AND HANDLING
FENTORA is supplied in individually sealed, child-resistant blister packages. The amount of fentanyl contained in FENTORA can be fatal to a child. Patients and their caregivers must be instructed to keep FENTORA out of the reach of children. (See BOXED WARNING, WARNINGS, PRECAUTIONS, and MEDICATION GUIDE.)
Store at 20-25°C (68-77°F) with excursions permitted between 15° and 30°C (59° to 86°F) until ready to use. (See USP Controlled Room Temperature.)
FENTORA should be protected from freezing and moisture. Do not use if the blister package has been tampered with.
DISPOSAL OF FENTORA
Patients and members of their household must be advised to dispose of any tablets remaining from a prescription as soon as they are no longer needed. Information is available in the Information for Patients and Caregivers and in the Medication Guide. If additional assistance is required, referral to the Cephalon 800# (1-800-896-5855) should be made.
To dispose of unused FENTORA, remove FENTORA tablets from blister packages and flush down the toilet. Do not flush FENTORA blister packages or cartons down the toilet. If you need additional assistance with disposal of FENTORA, call Cephalon, Inc., at 1-800-896-5855.
HOW SUPPLIED
Each carton contains 7 blister cards with 4 white tablets in each card. The blisters are child-resistant, encased in peelable foil, and provide protection from moisture. Each tablet is debossed on one side with  , and the other side of each dosage strength is uniquely identified by the debossing on the tablet as described in the table below. The dosage strength of each tablet is marked on the tablet, the blister package and the carton. See blister package and carton for product information.
, and the other side of each dosage strength is uniquely identified by the debossing on the tablet as described in the table below. The dosage strength of each tablet is marked on the tablet, the blister package and the carton. See blister package and carton for product information.
| Dosage Strength | Debossing | Carton/Blister | NDC Number |
|---|---|---|---|
| (fentanyl base) | Package Color | ||
| Note: Carton/blister package colors are a secondary aid in product identification. Please be sure to confirm the printed dosage before dispensing. |
|||
| 100 mcg | 1 | Blue | NDC 63459-541-28 |
| 200 mcg | 2 | Orange | NDC 63459-542-28 |
| 300 mcg | 3 | Gray | NDC 63459-543-28 |
| 400 mcg | 4 | Sage green | NDC 63459-544-28 |
| 600 mcg | 6 | Magenta (pink) | NDC 63459-546-28 |
| 800 mcg | 8 | Yellow | NDC 63459-548-28 |
Rx only.
DEA order form required. A Schedule CII narcotic.
Manufactured for:
Cephalon, Inc.
Frazer, PA 19355
By:
CIMA LABS, INC.
10000 Valley View Road
Eden Prairie, MN 55344
and
Cephalon, Inc.
4745 Wiley Post Way
Salt Lake City, UT 84116
U. S. Patent Nos. 6,200,604 and 6,974,590
Printed in USA
FENTORA® is a registered trademark of Cephalon, Inc., or its affiliates.
Label code 00010583.04
December 2009
© 2006 - 2009 Cephalon, Inc., or its affiliates. All rights reserved.
Medication Guide
FENTORA® (fen-tor-a) CII
(fentanyl buccal tablet)
100 mcg, 200 mcg, 300 mcg, 400 mcg, 600 mcg, 800 mcg
IMPORTANT:
- Do not use FENTORA unless you are regularly using other opioid pain medicines around-the-clock for your constant cancer pain and your body is used to these medicines.
- Keep FENTORA in a safe place away from children. Accidental use by a child is a medical emergency and can result in death. If a child accidentally takes FENTORA, get emergency help right away.
Read the Medication Guide that comes with FENTORA before you start taking it and each time you get a new prescription. There may be new information. This Medication Guide does not take the place of talking to your doctor about your medical condition or your treatment. Share this important information with members of your household.
What is the most important information I should know about FENTORA?
-
FENTORA can cause life threatening breathing problems which can lead to death:
- if you are not regularly using other opioid pain medicines around-the-clock for your constant cancer pain and your body is not used to these medicines. This means that you are not opioid tolerant.
- if you do not use it exactly as prescribed by your doctor.
- Your doctor will prescribe a starting dose of FENTORA that is different than other fentanyl containing medicines you may have been taking. Do not substitute FENTORA for other fentanyl medicines, including Actiq®, without talking to your doctor.
What is FENTORA?
- FENTORA is a prescription medicine that contains the medicine fentanyl. FENTORA is a federally controlled substance (CII) because it is a strong opioid pain medicine that can be abused by people who abuse prescription medicines or street drugs.
- FENTORA is used to treat breakthrough pain in adult patients with cancer (18 years of age and older) who are regularly using other opioid pain medicines around-the-clock for their constant cancer pain. FENTORA is started only after you have been taking other opioid pain medicines and your body has gotten used to them (you are opioid tolerant). DO NOT USE FENTORA if you are not opioid tolerant.
- You must stay under your doctor’s care while taking FENTORA.
- FENTORA must not be used for the treatment of short-term pain from injuries, surgery, and headaches, including migraines.
- FENTORA should be placed in the mouth, against your gum and allowed to dissolve. You may feel a gentle bubbling sensation between your cheek and gum as the tablet dissolves. FENTORA is not meant to be chewed or swallowed.
- Prevent theft and misuse. Keep FENTORA in a safe place to protect it from being stolen since it can be a target for people who abuse narcotic medicines or street drugs.
- Never give FENTORA to anyone else, even if they have the same symptoms you have. It may harm them and even cause death.
- Selling or giving away this medicine is against the law.
Who should not take FENTORA?
Do Not Take FENTORA:
- if you are not regularly using other opioid pain medicines around-the-clock for your constant cancer pain.
- for the treatment of short-term pain from injuries, surgery, and headaches, including migraines.
- if you are allergic to anything in FENTORA. The active ingredient is fentanyl. See the end of this Medication Guide for a complete list of ingredients in FENTORA.
What should I tell my doctor before starting FENTORA?
Tell your doctor about all of your medical and mental problems, especially the ones listed below:
- Trouble breathing or lung problems such as asthma, wheezing, or shortness of breath
- A head injury or brain problem
- Liver or kidney problems
- Seizures (convulsions or fits)
- Slow heart rate or other heart problems
- Low blood pressure
- Mental problems including major depression or hallucinations (seeing or hearing things that are not there)
- A past or present drinking problem or alcoholism, or a family history of this problem
- A past or present drug abuse or addiction problem, or a family history of this problem
Tell your doctor if you are:
- pregnant or planning to become pregnant. FENTORA may harm your unborn baby.
- breast feeding. FENTORA passes through your breast milk, and it can cause serious harm to your baby. You should not use FENTORA while breast feeding.
Tell your doctor about all the medicines you take, including prescription and non-prescription medicines, vitamins, and herbal and dietary supplements. Some medicines may cause serious or life-threatening medical problems when taken with FENTORA. Sometimes, the doses of certain medicines and FENTORA need to be changed if used together.
Do not take any medicine while using FENTORA until you have talked to your doctor. Your doctor will tell you if it is safe to take other medicines while you are using FENTORA. Be especially careful about taking other medicines that make you sleepy such as other pain medicines, anti-depressant medicines, sleeping pills, anxiety medicines, antihistamines, or tranquilizers.
Know the medicines you take. Keep a list of them to show your doctor and pharmacist.
How should I use FENTORA?
-
Use FENTORA exactly as prescribed by your doctor. Do not use FENTORA more often than prescribed.
- Use 1 dose of FENTORA for an episode of breakthrough cancer pain. When the amount of FENTORA is being adjusted by your doctor, a dose may include more than 1 tablet.
- If your breakthrough cancer pain is not relieved after 30 minutes, use ONLY 1 more dose of FENTORA at this time.
- Wait at least 4 more hours before using FENTORA again for another episode of breakthrough cancer pain.
- Remember you must continue taking your regularly used around-the-clock opioid medicine while taking FENTORA.
- Talk to your doctor if your dose of FENTORA does not relieve your breakthrough cancer pain. Your doctor will decide if your dose of FENTORA needs to be changed.
- Talk to your doctor if you have more than 4 episodes of breakthrough cancer pain per day. The dose of your around-the-clock opioid pain medicine may need to be adjusted.
-
FENTORA comes packaged in a blister card. Do not open the blister until ready to use. Separate one of the blister units from the blister card by tearing apart at the perforations. Bend the blister unit along the line where indicated. Peel back foil on blister pack to expose tablet.

- DO NOT push the tablet through the foil on the blister pack because this could damage the tablet.
- Once removed from the blister pack, FENTORA must be used right away.
-
Place a FENTORA tablet in your mouth above a rear molar tooth between the upper cheek and gum and leave in place until the tablet is dissolved. This generally takes between 14 to 25 minutes. After 30 minutes if there is any tablet left, swallow it with a glass of water. If you cannot take the medicine in this manner, tell your doctor who will advise you what to do. Do not split the tablet.

- Do not bite, chew or suck FENTORA tablets. If you do so, you will swallow more of the medicine and get less relief for your breakthrough cancer pain.
- Do not split the FENTORA tablet. The FENTORA tablet should be used whole.
- If you begin to feel dizzy, sick to your stomach, or very sleepy before the tablet is completely dissolved, rinse your mouth with water and spit the remaining pieces of the tablet into a sink or toilet right away. Rinse the sink or flush the toilet to dispose of any remaining tablet pieces.
- If you take too much FENTORA or overdose, call 911 for emergency help.
What should I avoid while taking FENTORA?
- Do not drive, operate heavy machinery, or do other dangerous activities until you know how FENTORA affects how alert you are. FENTORA can make you sleepy. Ask your doctor when it is okay to do these activities.
- Do not drink alcohol while using FENTORA. It can increase your chance of getting dangerous side effects.
- Do not take any medicine while using FENTORA until you have talked to your doctor. Your doctor will tell you if it is safe to take other medicines while you are using FENTORA. Be especially careful about taking other medicines that make you sleepy such as other pain medicines, anti-depressant medicines, sleeping pills, anxiety medicines, antihistamines, or tranquilizers
What are the possible or reasonably likely SIDE EFFECTS of FENTORA?
- FENTORA can cause serious breathing problems that can become life-threatening, especially if used the wrong way. See “What is the most important information I should know about FENTORA?”
Call your doctor or get emergency medical help right away if you:
- have trouble breathing
- have extreme drowsiness with slowed breathing
- have slow, shallow breathing (little chest movement with breathing)
- feel faint, very dizzy, confused, or have unusual symptoms
The above symptoms mean that you have taken too much (overdose) FENTORA or the dose is too high for you. These symptoms may lead to serious problems or death if not treated right away. Do not take another dose of FENTORA.
- FENTORA can cause pain or sores at the application site (on your gum or the inside of your cheek). Tell your doctor if this is a problem for you.
- FENTORA can cause your blood pressure to drop. This can make you feel dizzy if you get up too fast from sitting or lying down.
- FENTORA can cause physical dependence. Do not stop taking FENTORA or any other opioid without talking to your doctor. You could become sick with uncomfortable withdrawal symptoms because your body has become used to these medicines. Physical dependence is not the same as drug addiction.
- There is a chance of abuse or addiction with FENTORA. The chance is higher if you are or have been addicted to or abused other medications, street drugs, or alcohol, or if you have a history of mental problems.
- The most common side effects of FENTORA are nausea, vomiting, dizziness, sleepiness, headache, and constipation. Constipation (not often enough or hard bowel movements) is a very common side effect of pain medicines (opioids) including FENTORA and is unlikely to go away without treatment. Talk to your doctor about dietary changes, and the use of laxatives (medicines to treat constipation) and stool softeners to prevent or treat constipation while taking FENTORA.
Talk to your doctor about any side effects that bother you or that do not go away.
These are not all the possible side effects of FENTORA. For a complete list, ask your doctor.
Call your doctor for medical advice about sideeffects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store FENTORA?
- Keep FENTORA in a safe and secure place away from children and from anyone for whom it has not been prescribed. Accidental use by a child is a medical emergency and can result in death. If a child accidentally takes FENTORA, get emergency help right away.
- FENTORA is supplied in single sealed child-resistant blister packages.
- Do NOT remove FENTORA from its blister packaging for storage in a temporary container, such as a pillbox.
- Store FENTORA at room temperature, 59° to 86°F (15° to 30°C) until ready to use.
- Always keep FENTORA in a secure place to protect from theft.
How should I dispose of unopened FENTORA tablets when they are no longer needed?
- Dispose of any unopened FENTORA tablets remaining from a prescription as soon as they are no longer needed.
- To dispose of unused FENTORA, remove FENTORA tablets from blister packages and flush down the toilet. Do not flush the FENTORA blister packages or cartons down the toilet.
- If you need help with disposal of FENTORA, call Cephalon, Inc., at 1-800-896-5855.
General Information About the Safe and Effective Use of FENTORA
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Use FENTORA only for the purpose for which it was prescribed. Do not give FENTORA to other people, even if they have the same symptoms you have. FENTORA can harm other people and even cause death. Sharing FENTORA is against the law.
This Medication Guide summarizes the most important information about FENTORA. If you would like more information, talk with your doctor. You can ask your pharmacist or doctor for information about FENTORA that is written for healthcare professionals. You can also call Cephalon, Inc., at 1-800-896-5855.
What are the ingredients of FENTORA?
Active Ingredient: fentanyl citrate
Inactive Ingredients: mannitol, sodium starch glycolate, sodium bicarbonate, sodium carbonate, citric acid, and magnesium stearate.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Rx Only.
Cephalon, Inc.
FRAZER, PA 19355, USA
Reference Number 00010583.04
December 2009
U.S. Patent Nos. 6,200,604 and 6,974,590
Printed in the USA
FENTORA® is a trademark of Cephalon, Inc., or its affiliates.
© 2006 - 2009 Cephalon, Inc., or its affiliates. All rights reserved.
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-541-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-541-04

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-542-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-542-04

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-543-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-543-04

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-544-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-544-04

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-546-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-546-04

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Primary label panel for NDC 63459-548-28

PACKAGE LABEL.PRINCIPAL DISPLAY PANEL SECTION
Blister label for NDC 63459-548-04

| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 09/25/2006 | |
| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 09/25/2006 | |
| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 03/02/2007 | |
| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 09/25/2006 | |
| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 09/25/2006 | |
| FENTORA
fentanyl buccal tablet tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021947 | 09/25/2006 | |
| Labeler - Cephalon Inc. (183236314) |
| Establishment | |||
| Name | Address | ID/FEI | Operations |
| Cephalon, Inc. | 177319472 | manufacture | |