ADVICOR
-
niacin and
lovastatin tablet, extended release
ADVICOR
-
niacin and
lovastatin tablet, film coated
Physicians Total Care, Inc.
----------
DESCRIPTION
ADVICOR® (niacin extended-release and lovastatin) is intended to facilitate the daily administration of its individual components, Niaspan® and lovastatin, when used together for the intended patient population (see INDICATIONS AND USAGE and DOSAGE AND ADMINISTRATION).
ADVICOR contains niacin extended-release and lovastatin in combination. Lovastatin, an inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, and niacin are both lipid-altering agents.
Niacin is nicotinic acid, or 3-pyridinecarboxylic acid. Niacin is a white, nonhygroscopic crystalline powder that is very soluble in water, boiling ethanol and propylene glycol. It is insoluble in ethyl ether. The empirical formula of niacin is C6H5NO2 and its molecular weight is 123.11. Niacin has the following structural formula:
Lovastatin is [1S -[1(alpha)(R *), 3(alpha), 7(beta), 8(beta)(2S *, 4S *), 8a(beta)]]-1,2,3, 7,8,8a-hexahydro-3,7-dimethyl-8-[2-(tetrahydro-4-hydroxy-6-oxo-2H-pyran-2-yl) ethyl]-1-naphthalenyl 2-methylbutanoate. Lovastatin is a white, nonhygroscopic crystalline powder that is insoluble in water and sparingly soluble in ethanol, methanol, and acetonitrile. The empirical formula of lovastatin is C24H36O5 and its molecular weight is 404.55. Lovastatin has the following structural formula:
ADVICOR tablets contain the labeled amount of niacin and lovastatin and have the following inactive ingredients: hypromellose, povidone, stearic acid, polyethylene glycol, titanium dioxide, polysorbate 80.
The individual tablet strengths (expressed in terms of mg niacin/mg lovastatin) contain the following coloring agents:
ADVICOR 500 mg/20 mg - synthetic red and yellow iron oxides.
ADVICOR 750
mg/20 mg – FD&C yellow #6 Aluminum Lake.
ADVICOR 1000 mg/20 mg -
synthetic red, yellow, and black iron oxides.
ADVICOR 1000 mg/40 mg – red
iron oxide.
CLINICAL PHARMACOLOGY
A variety of clinical studies have demonstrated that elevated levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and apolipoprotein B-100 (Apo B) promote human atherosclerosis. Similarly, decreased levels of high-density lipoprotein cholesterol (HDL-C) are associated with the development of atherosclerosis. Epidemiological investigations have established that cardiovascular morbidity and mortality vary directly with the level of TC and LDL-C, and inversely with the level of HDL-C.
Cholesterol-enriched triglyceride-rich lipoproteins, including very low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), and their remnants, can also promote atherosclerosis. Elevated plasma triglycerides (TG) are frequently found in a triad with low HDL-C levels and small LDL particles, as well as in association with non-lipid metabolic risk factors for coronary heart disease (CHD). As such, total plasma TG have not consistently been shown to be an independent risk factor for CHD.
As an adjunct to diet, the efficacy of niacin and lovastatin in improving lipid profiles (either individually, or in combination with each other, or niacin in combination with other statins) for the treatment of dyslipidemia has been well documented. The effect of combined therapy with niacin and lovastatin on cardiovascular morbidity and mortality has not been determined.
Effects on lipids ADVICORADVICOR reduces LDL-C, TC, and TG, and increases HDL-C due to the individual actions of niacin and lovastatin. The magnitude of individual lipid and lipoprotein responses may be influenced by the severity and type of underlying lipid abnormality.
NiacinNiacin functions in the body after conversion to nicotinamide adenine dinucleotide (NAD) in the NAD coenzyme system. Niacin (but not nicotinamide) in gram doses reduces LDL-C, Apo B, Lp(a), TG, and TC, and increases HDL-C. The increase in HDL-C is associated with an increase in apolipoprotein A-I (Apo A-I) and a shift in the distribution of HDL subfractions. These shifts include an increase in the HDL2:HDL3 ratio, and an elevation in lipoprotein A-I (Lp A-I, an HDL-C particle containing only Apo A-I). In addition, preliminary reports suggest that niacin causes favorable LDL particle size transformations, although the clinical relevance of this effect is not yet clear.
LovastatinLovastatin has been shown to reduce both normal and elevated LDL-C concentrations. Apo B also falls substantially during treatment with lovastatin. Since each LDL-C particle contains one molecule of Apo B, and since little Apo B is found in other lipoproteins, this strongly suggests that lovastatin does not merely cause cholesterol to be lost from LDL-C, but also reduces the concentration of circulating LDL particles. In addition, lovastatin can produce increases of variable magnitude in HDL-C, and modestly reduces VLDL-C and plasma TG. The effects of lovastatin on Lp(a), fibrinogen, and certain other independent biochemical risk markers for coronary heart disease are not well characterized.
Mechanism of Action NiacinThe mechanism by which niacin alters lipid profiles is not completely understood and may involve several actions, including partial inhibition of release of free fatty acids from adipose tissue, and increased lipoprotein lipase activity (which may increase the rate of chylomicron triglyceride removal from plasma). Niacin decreases the rate of hepatic synthesis of VLDL-C and LDL-C, and does not appear to affect fecal excretion of fats, sterols, or bile acids.
LovastatinLovastatin is a specific inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, the enzyme that catalyzes the conversion of HMG-CoA to mevalonate. The conversion of HMG-CoA to mevalonate is an early step in the biosynthetic pathway for cholesterol. Lovastatin is a prodrug and has little, if any, activity until hydrolyzed to its active beta-hydroxyacid form, lovastatin acid. The mechanism of the LDL-lowering effect of lovastatin may involve both reduction of VLDL-C concentration and induction of the LDL receptor, leading to reduced production and/or increased catabolism of LDL-C.
Pharmacokinetics Absorption and Bioavailability ADVICORIn single-dose studies of ADVICOR, rate and extent of niacin and lovastatin absorption were bioequivalent under fed conditions to that from NIASPAN® (niacin extended-release tablets) and Mevacor® (lovastatin) tablets, respectively. After administration of two ADVICOR 1000 mg/20 mg tablets, peak niacin concentrations averaged about 18 mcg/mL and occurred about 5 hours after dosing; about 72% of the niacin dose was absorbed according to the urinary excretion data. Peak lovastatin concentrations averaged about 11 ng/mL and occurred about 2 hours after dosing.
The extent of niacin absorption from ADVICOR was increased by administration with food. The administration of two ADVICOR 1000 mg/20 mg tablets under low-fat or high-fat conditions resulted in a 22 to 30% increase in niacin bioavailability relative to dosing under fasting conditions. Lovastatin bioavailability is affected by food. Lovastatin Cmax was increased 48% and 21% after a high- and a low-fat meal, respectively, but the lovastatin AUC was decreased 26% and 24% after a high- and a low-fat meal, respectively, compared to those under fasting conditions.
A relative bioavailability study results indicated that ADVICOR tablet strengths (i.e., two tablets of 500 mg/20 mg and one tablet of 1000 mg/40 mg) are not interchangeable.
NiacinDue to extensive and saturable first-pass metabolism, niacin concentrations in the general circulation are dose dependent and highly variable. Peak steady-state niacin concentrations were 0.6, 4.9, and 15.5 mcg/mL after doses of 1000, 1500, and 2000 mg NIASPAN once daily (given as two 500 mg, two 750 mg, and two 1000 mg tablets, respectively).
LovastatinLovastatin appears to be incompletely absorbed after oral administration. Because of extensive hepatic extraction, the amount of lovastatin reaching the systemic circulation as active inhibitors after oral administration is low (less than 5%) and shows considerable inter-individual variation. Peak concentrations of active and total inhibitors occur within 2 to 4 hours after Mevacor® administration.
Lovastatin absorption appears to be increased by at least 30% by grapefruit juice; however, the effect is dependent on the amount of grapefruit juice consumed and the interval between grapefruit juice and lovastatin ingestion. With a once-a-day dosing regimen, plasma concentrations of total inhibitors over a dosing interval achieved a steady-state between the second and third days of therapy and were about 1.5 times those following a single dose of Mevacor®.
Although the mechanism is not fully understood, cyclosporine has been shown to increase the AUC of HMG-CoA reductase inhibitors. The increase in AUC for lovastatin and lovastatin acid is presumably due, in part, to inhibition of CYP3A4.
Distribution NiacinNiacin is less than 20% bound to human serum proteins and distributes into milk. Studies using radiolabeled niacin in mice show that niacin and its metabolites concentrate in the liver, kidney, and adipose tissue.
LovastatinBoth lovastatin and its beta-hydroxyacid metabolite are highly bound (greater than 95%) to human plasma proteins. Distribution of lovastatin or its metabolites into human milk is unknown; however, lovastatin distributes into milk in rats. In animal studies, lovastatin concentrated in the liver, and crossed the blood-brain and placental barriers.
Metabolism NiacinNiacin undergoes rapid and extensive first-pass metabolism that is dose-rate specific and, at the doses used to treat dyslipidemia, saturable. In humans, one pathway is through a simple conjugation step with glycine to form nicotinuric acid (NUA). NUA is then excreted, although there may be a small amount of reversible metabolism back to niacin. The other pathway results in the formation of NAD. It is unclear whether nicotinamide is formed as a precursor to, or following the synthesis of, NAD. Nicotinamide is further metabolized to at least N-methylnicotinamide (MNA) and nicotinamide-N-oxide (NNO). MNA is further metabolized to two other compounds, N-methyl-2-pyridone-5-carboxamide (2PY) and N-methyl-4-pyridone-5-carboxamide (4PY). The formation of 2PY appears to predominate over 4PY in humans.
LovastatinLovastatin undergoes extensive first-pass extraction and metabolism by cytochrome P450 3A4 in the liver, its primary site of action. The major active metabolites present in human plasma are the beta-hydroxyacid of lovastatin (lovastatin acid), its 6'-hydroxy derivative, and two additional metabolites.
Elimination ADVICORNiacin is primarily excreted in urine mainly as metabolites. After a single dose of ADVICOR, at least 60% of the niacin dose was recovered in urine as unchanged niacin and its metabolites. The plasma half-life for lovastatin was about 4.5 hours in single-dose studies.
NiacinThe plasma half-life for niacin is about 20 to 48 minutes after oral administration and dependent on dose administered. Following multiple oral doses of NIASPAN, up to 12% of the dose was recovered in urine as unchanged niacin depending on dose administered. The ratio of metabolites recovered in the urine was also dependent on the dose administered.
LovastatinLovastatin is excreted in urine and bile, based on studies of Mevacor®. Following an oral dose of radiolabeled lovastatin in man, 10% of the dose was excreted in urine and 83% in feces. The latter represents absorbed drug equivalents excreted in bile, as well as any unabsorbed drug.
Special Populations HepaticNo pharmacokinetic studies have been conducted in patients with hepatic insufficiency for either niacin or lovastatin (see WARNINGS, Liver Dysfunction).
RenalNo information is available on the pharmacokinetics of niacin in patients with renal insufficiency.
In a study of patients with severe renal insufficiency (creatinine clearance 10 to 30 mL/min), the plasma concentrations of total inhibitors after a single dose of lovastatin were approximately two-fold higher than those in healthy volunteers.
ADVICOR should be used with caution in patients with renal disease.
GenderPlasma concentrations of niacin and metabolites after single- or multiple-dose administration of niacin are generally higher in women than in men, with the magnitude of the difference varying with dose and metabolite. Recovery of niacin and metabolites in urine, however, is generally similar for men and women, indicating similar absorption for both genders. The gender differences observed in plasma niacin and metabolite levels may be due to gender-specific differences in metabolic rate or volume of distribution. Data from clinical trials suggest that women have a greater hypolipidemic response than men at equivalent doses of NIASPAN and ADVICOR.
In a multiple-dose study, plasma concentrations of active and total HMG-CoA reductase inhibitors were 20 to 50% higher in women than in men. In two single-dose studies with ADVICOR, lovastatin concentrations were about 30% higher in women than men, and total HMG-CoA reductase inhibitor concentrations were about 20 to 25% greater in women.
In a multi-center, randomized, double-blind, active-comparator study in patients with Type IIa and IIb hyperlipidemia, ADVICOR was compared to single-agent treatment (NIASPAN and lovastatin). The treatment effects of ADVICOR compared to lovastatin and NIASPAN differed for males and females with a significantly larger treatment effect seen for females. The mean percent change from baseline at endpoint for LDL-C, TG, and HDL-C by gender are as follows (Table 1):
|
| ADVICOR 2000 mg/40 mg | NIASPAN 2000 mg | Lovastatin 40 mg | |||
|
| Women (n=22) | Men (n=30) | Women (n=28) | Men (n=28) | Women (n=21) | Men (n=38) |
| LDL-C | -47% | -34% | -12% | -9% | -31% | -31% |
| HDL-C | +33% | +24% | +22% | +15% | +3% | +7% |
| TG | -48% | -35% | -25% | -15% | -15% | -23% |
In a multi-center, randomized, double-blind, parallel, 28-week, active-comparator study in patients with Type IIa and IIb hyperlipidemia, ADVICOR was compared to each of its components (NIASPAN and lovastatin). Using a forced dose-escalation study design, patients received each dose for at least 4 weeks. Patients randomized to treatment with ADVICOR initially received 500 mg/20 mg. The dose was increased at 4-week intervals to a maximum of 1000 mg/20 mg in one-half of the patients and 2000 mg/40 mg in the other half. The NIASPAN monotherapy group underwent a similar titration from 500 mg to 2000 mg. The patients randomized to lovastatin monotherapy received 20 mg for 12 weeks titrated to 40 mg for up to 16 weeks. Up to a third of the patients randomized to ADVICOR or NIASPAN discontinued prior to Week 28. In this study, ADVICOR decreased LDL-C, TG and Lp(a), and increased HDL-C in a dose-dependent fashion (Tables 2, 3, 4 and 5 below). Results from this study for LDL-C mean percent change from baseline (the primary efficacy variable) showed that:
- LDL-lowering with ADVICOR was significantly greater than that achieved with lovastatin 40 mg only after 28 weeks of titration to a dose of 2000 mg/40 mg (p less than .0001)
- ADVICOR at doses of 1000 mg/20 mg or higher achieved greater LDL-lowering than NIASPAN (p less than .0001) The LDL-C results are summarized in Table 2.
| Week | ADVICOR | NIASPAN | Lovastatin | ||||||
|
| n* | Dose (mg/mg) | LDL | n* | Dose (mg) | LDL | n* | Dose (mg) | LDL |
| Baseline | 57 | - | 190.9 mg/dL | 61 | - | 189.7 mg/dL | 61 | - | 185.6 mg/dL |
| 12 | 47 | 1000/20 | -30% | 46 | 1000 | -3% | 56 | 20 | -29% |
| 16 | 45 | 1000/40 | -36% | 44 | 1000 | -6% | 56 | 40 | -31% |
| 20 | 42 | 1500/40 | -37% | 43 | 1500 | -12% | 54 | 40 | -34% |
| 28 | 42 | 2000/40 | -42% | 41 | 2000 | -14% | 53 | 40 | -32% |
ADVICOR achieved significantly greater HDL-raising compared to lovastatin and NIASPAN monotherapy at all doses (Table 3).
Table 3. HDL-C mean percent change from baseline
| Week | ADVICOR | NIASPAN | Lovastatin | ||||||
|
| n* | Dose (mg/mg) | HDL | n* | Dose (mg) | HDL | n* | Dose (mg) | HDL |
| Baseline | 57 | - | 45 mg/dL | 61 | - | 47 mg/dL | 61 | - | 43 mg/dL |
| 12 | 47 | 1000/20 | +20% | 46 | 1000 | +14% | 56 | 20 | +3% |
| 16 | 45 | 1000/40 | +20% | 44 | 1000 | +15% | 56 | 40 | +5% |
| 20 | 42 | 1500/40 | +27% | 43 | 1500 | +22% | 54 | 40 | +6% |
| 28 | 42 | 2000/40 | +30% | 41 | 2000 | +24% | 53 | 40 | +6% |
In addition, ADVICOR achieved significantly greater TG-lowering at doses of 1000 mg/20 mg or greater compared to lovastatin and NIASPAN monotherapy (Table 4).
Table 4. TG median percent change from baseline
| Week | ADVICOR | NIASPAN | Lovastatin | ||||||
|
| n* | Dose (mg/mg) | TG | n* | Dose (mg) | TG | n* | Dose (mg) | TG |
| Baseline | 57 | - | 174 mg/dL | 61 | - | 186 mg/dL | 61 | - | 171 mg/dL |
| 12 | 47 | 1000/20 | -32% | 46 | 1000 | -22% | 56 | 20 | -20% |
| 16 | 45 | 1000/40 | -39% | 44 | 1000 | -23% | 56 | 40 | -17% |
| 20 | 42 | 1500/40 | -44% | 43 | 1500 | -31% | 54 | 40 | -21% |
| 28 | 42 | 2000/40 | -44% | 41 | 2000 | -31% | 53 | 40 | -20% |
The Lp(a) lowering effects of ADVICOR and NIASPAN were similar, and both were superior to lovastatin (Table 5). The independent effect of lowering Lp(a) with NIASPAN or ADVICOR on the risk of coronary and cardiovascular morbidity and mortality has not been determined.
Table 5. Lp(a) median percent change from baseline
| Week | ADVICOR | NIASPAN | Lovastatin | ||||||
|
| n* | Dose (mg/mg) | Lp(a) | n* | Dose (mg) | Lp(a) | n* | Dose (mg) | Lp(a) |
| Baseline | 57 | - | 34 mg/dL | 61 | - | 41 mg/dL | 60 | - | 42 mg/dL |
| 12 | 47 | 1000/20 | -9% | 46 | 1000 | -8% | 55 | 20 | +8% |
| 16 | 45 | 1000/40 | -9% | 44 | 1000 | -12% | 55 | 40 | +8% |
| 20 | 42 | 1500/40 | -17% | 43 | 1500 | -22% | 53 | 40 | +6% |
| 28 | 42 | 2000/40 | -22% | 41 | 2000 | -32% | 52 | 40 | 0% |
ADVICOR Long-Term Study
A total of 814 patients were enrolled in a long-term (52-week), open-label, single-arm study of ADVICOR. Patients were force dose-titrated to 2000 mg/40 mg over 16 weeks. After titration, patients were maintained on the maximum tolerated dose of ADVICOR for a total of 52 weeks. Five hundred-fifty (550) patients (68%) completed the study, and fifty-six percent (56%) of all patients were able to maintain a dose of 2000 mg/40 mg for the 52 weeks of treatment. The lipid-altering effects of ADVICOR peaked after 4 weeks on the maximum tolerated dose, and were maintained for the duration of treatment. These effects were comparable to what was observed in the double-blind study of ADVICOR (Tables 2-4).
INDICATIONS AND USAGE
Therapy with lipid-altering agents should be only one component of multiple risk-factor intervention in individuals at significantly increased risk for atherosclerotic vascular disease due to hypercholesterolemia. Drug therapy is indicated as an adjunct to diet when the response to a diet restricted in saturated fat and cholesterol and other nonpharmacologic measures alone has been inadequate (see also Table 7 and the NCEP treatment guidelines1).
ADVICORADVICOR (niacin extended-release and lovastatin) is indicated for use when treatment with both NIASPAN and lovastatin is appropriate. As described in the labeling for Niaspan and lovastatin below, the components of ADVICOR are both indicated for the treatment of hypercholesterolemia. Patients receiving treatment with ADVICOR should be on a standard cholesterol-lowering diet and should continue on this diet during treatment.
NIASPAN (niacin extended-release) HypercholesterolemiaNIASPAN is indicated as an adjunct to diet for reduction of elevated TC, LDL-C, Apo B and TG levels, and to increase HDL-C in patients with primary hypercholesterolemia (heterozygous familial and nonfamilial) and mixed dyslipidemia (Frederickson Types IIa and IIb; Table 6), when the response to an appropriate diet has been inadequate.
Secondary Prevention of Cardiovascular EventsIn patients with a history of myocardial infarction and hypercholesterolemia, niacin is indicated to reduce the risk of recurrent nonfatal myocardial infarction.
HypertriglyceridemiaNiacin is also indicated as adjunctive therapy for treatment of adult patients with very high serum triglyceride levels (Types IV and V hyperlipidemia; Table 6) who present a risk of pancreatitis and who do not respond adequately to a determined dietary effort to control them. Such patients typically have serum TG levels over 2000 mg/dL and have elevations of VLDL-C as well as fasting chylomicrons (Type V hyperlipidemia; Table 6). Patients who consistently have total serum or plasma TG below 1000 mg/dL are unlikely to develop pancreatitis. Therapy with niacin may be considered for those patients with TG elevations between 1000 and 2000 mg/dL who have a history of pancreatitis or of recurrent abdominal pain typical of pancreatitis. Some Type IV patients with TG under 1000 mg/dL may, through dietary or alcohol indiscretion, convert to a Type V pattern with massive TG elevations accompanying fasting chylomicronemia, but the influence of niacin therapy on risk of pancreatitis in such situations has not been adequately studied. Drug therapy is not indicated for patients with Type I hyperlipoproteinemia, who have elevations of chylomicrons and plasma TG, but who have normal levels of VLDL-C. Inspection of plasma refrigerated for 14 hours is helpful in distinguishing Types I, IV, and V hyperlipoproteinemia.2
Lovastatin HypercholesterolemiaLovastatin is indicated as an adjunct to diet for the reduction of elevated TC and LDL-C levels in patients with primary hypercholesterolemia (Frederickson Types IIa and IIb; Table 6), when the response to diet restricted in saturated fat and cholesterol and to other nonpharmacological measures alone has been inadequate.
Primary Prevention of Cardiovascular EventsIn individuals without symptomatic cardiovascular disease, average to moderately elevated TC and LDL-C, and below average HDL-C, lovastatin is indicated to reduce the risk of:
- Myocardial infarction - Unstable angina - Coronary revascularization procedures Secondary Prevention of Cardiovascular EventsLovastatin is also indicated to slow the progression of coronary atherosclerosis in patients with coronary heart disease as part of a treatment strategy to lower TC and LDL-C to target levels.
The National Cholesterol Education Program (NCEP) Treatment Guidelines are
summarized below:
Table 6 Classification of Hyperlipoproteinemias
|
|
|
| Lipid Elevations |
|
| Type | Lipoproteins Elevated |
|
|
|
|
|
| Major |
| Minor |
| I (rare) | Chylomicrons | TG |
| ↑→TC |
| IIa | LDL | TC |
| - |
| IIb | LDL, VLDL | TC |
| TG |
| III (rare) | IDL | TC/TG |
| - |
| IV | VLDL | TG |
| ↑→TC |
| V (rare) | Chylomicrons, VLDL | TG |
| ↑→TC |
General Recommendations
Prior to initiating therapy with a lipid-lowering agent, secondary causes for hypercholesterolemia (e.g., poorly controlled diabetes mellitus, hypothyroidism, nephrotic syndrome, dysproteinemias, obstructive liver disease, other drug therapy, alcoholism) should be excluded, and a lipid profile performed to measure TC, HDL-C, and TG. For patients with TG less than 400 mg/dL, LDL-C can be estimated using the following equation:
LDL-C = TC – [(0.20 x TG) + HDL-C]
For TG levels greater than 400 mg/dL, this equation is less accurate and LDL-C concentrations should be determined by ultracentrifugation. Lipid determinations should be performed at intervals of no less than 4 weeks and dosage adjusted according to the patient's response to therapy. The NCEP Treatment Guidelines are summarized in Table 7.|
Risk Category |
LDL Goal (mg/dL) | LDL Level at Which to Initiate Therapeutic Lifestyle Changes (mg/dL) | LDL Level at Which to Consider Drug Therapy (mg/dL) |
| CHD† or CHD risk equivalents (10-year risk greater than 20%) |
less than 100 |
greater than or equal to 100 |
greater than or equal to130 (100-129:drug optional) †† |
|
2+ Risk factors (10-year risk less than or equal to 20%) |
less than 130 |
greater than or equal to 130 |
10-year risk 10%-20%: greater than or equal to 130 10-year risk less than 10%: greater than or equal to 160 |
| 0-1 Risk factor ††† |
less than 160 |
greater than or equal to 160 |
greater than or equal to190 (160-189:LDL-lowering drug optional) |
† CHD, coronary heart disease
†† Some authorities recommend use
of LDL-lowering drugs in this category if an LDL-C level of less than 100 mg/dL cannot
be achieved by therapeutic lifestyle changes. Others prefer use of drugs that
primarily modify triglycerides and HDL-C, e.g., nicotinic acid or fibrate.
Clinical judgement also may call for deferring drug therapy in this subcategory.
††† Almost all people with 0-1
risk factor have 10-year risk less than 10%; thus, 10-year risk assessment in people
with 0-1 risk factor is not necessary.
After the LDL-C goal has been achieved, if the TG is still greater than or equal to 200 mg/dL, non-HDL-C (TC minus HDL-C) becomes a secondary target of therapy. Non-HDL-C goals are set 30 mg/dL higher than LDL-C goals for each risk category.
CONTRAINDICATIONS
ADVICOR is contraindicated in patients with a known hypersensitivity to niacin, lovastatin or any component of this medication, active liver disease or unexplained persistent elevations in serum transaminases (see WARNINGS), active peptic ulcer disease, or arterial bleeding.
Pregnancy and lactation – Atherosclerosis is a chronic process and the discontinuation of lipid-lowering drugs during pregnancy should have little impact on the outcome of long-term therapy of primary hypercholesterolemia. Moreover, cholesterol and other products of the cholesterol biosynthesis pathway are essential components for fetal development, including synthesis of steroids and cell membranes. Because of the ability of inhibitors of HMG-CoA reductase, such as lovastatin, to decrease the synthesis of cholesterol and possibly other products of the cholesterol biosynthesis pathway, ADVICOR is contraindicated in women who are pregnant and in lactating mothers. ADVICOR may cause fetal harm when administered to pregnant women. ADVICOR should be administered to women of childbearing age only when such patients are highly unlikely to conceive. If the patient becomes pregnant while taking this drug, ADVICOR should be discontinued immediately and the patient should be apprised of the potential hazard to the fetus (see PRECAUTIONS, Pregnancy).
WARNINGS
ADVICOR should not be substituted for equivalent doses of immediate-release (crystalline) niacin. For patients switching from immediate-release niacin to NIASPAN, therapy with NIASPAN should be initiated with low doses (i.e., 500 mg once daily at bedtime) and the NIASPAN dose should then be titrated to the desired therapeutic response (see DOSAGE AND ADMINISTRATION).
Liver DysfunctionCases of severe hepatic toxicity, including fulminant hepatic necrosis, have occurred in patients who have substituted sustained-release (modified-release, timed-release) niacin products for immediate-release (crystalline) niacin at equivalent doses.
ADVICOR should be used with caution in patients who consume substantial quantities of alcohol and/or have a past history of liver disease. Active liver disease or unexplained transaminase elevations are contraindications to the use of ADVICOR.
Niacin preparations and lovastatin preparations have been associated with abnormal liver tests. In studies using NIASPAN alone, 0.8% of patients were discontinued for transaminase elevations. In studies using lovastatin alone, 0.2% of patients were discontinued for transaminase elevations.4 In three safety and efficacy studies involving titration to final daily ADVICOR doses ranging from 500 mg/10 mg to 2500 mg/40 mg, ten of 1028 patients (1.0%) experienced reversible elevations in AST/ALT to more than 3 times the upper limit of normal (ULN). Three of ten elevations occurred at doses outside the recommended dosing limit of 2000 mg/40 mg; no patient receiving 1000 mg/20 mg had 3-fold elevations in AST/ALT.
In clinical studies with ADVICOR, elevations in transaminases did not appear to be related to treatment duration; elevations in AST and ALT levels did appear to be dose related. Transaminase elevations were reversible upon discontinuation of ADVICOR.
Liver function tests should be performed on all patients during therapy with ADVICOR. Serum transaminase levels, including AST and ALT (SGOT and SGPT), should be monitored before treatment begins, every 6 to 12 weeks for the first 6 months, and periodically thereafter (e.g., at approximately 6-month intervals). Special attention should be paid to patients who develop elevated serum transaminase levels, and in these patients, measurements should be repeated promptly and, if confirmed, then performed more frequently. If the transaminase levels show evidence of progression, particularly if they rise to 3 times ULN and are persistent, or if they are associated with symptoms of nausea, fever, and/or malaise, the drug should be discontinued.
Skeletal Muscle LovastatinLovastatin and other inhibitors of HMG-CoA reductase occasionally cause myopathy, which is manifested as muscle pain or weakness associated with grossly elevated creatine kinase (> 10 times ULN). Rhabdomyolysis, with or without acute renal failure secondary to myoglobinuria, has been reported rarely and can occur at any time. In a large, long-term, clinical safety and efficacy study (the EXCEL study)5,6 with lovastatin, myopathy occurred in up to 0.2% of patients treated with lovastatin 20 to 80 mg for up to 2 years. When drug treatment was interrupted or discontinued in these patients, muscle symptoms and creatine kinase (CK) increases promptly resolved. The risk of myopathy is increased by concomitant therapy with certain drugs, some of which were excluded by the EXCEL study design.
Potent inhibitors of CYP3A4: The risk of myopathy appears to be increased by high levels of HMG-CoA reductase inhibitory activity in plasma. Lovastatin is metabolized by the cytochrome P450 isoform 3A4. Certain drugs which share this metabolic pathway can raise the plasma levels of lovastatin and may increase the risk of myopathy. These include cyclosporine, itraconazole, ketoconazole and other antifungal azoles, the macrolide antibiotics erythromycin and clarithromycin, and the ketolide antibiotic telithromycin, HIV protease inhibitors, the antidepressant nefazodone, or large quantities of grapefruit juice (>1 quart daily).
ADVICORMyopathy and/or rhabdomyolysis have been reported when lovastatin is used in combination with lipid-altering doses (≥1g/day) of niacin. Physicians contemplating the use of ADVICOR, a combination of lovastatin and niacin, should weigh the potential benefits and risks, and should carefully monitor patients for any signs and symptoms of muscle pain, tenderness, or weakness, particularly during the initial month of treatment or during any period of upward dosage titration of either drug. Periodic CK determinations may be considered in such situations, but there is no assurance that such monitoring will prevent myopathy.
In clinical studies, no cases of rhabdomyolysis and one suspected case of myopathy have been reported in 1079 patients who were treated with ADVICOR at doses up to 2000 mg/40 mg for periods up to 2 years.
Patients starting therapy with ADVICOR should be advised of the risk of myopathy, and told to report promptly unexplained muscle pain, tenderness, or weakness. A CK level above 10 times ULN in a patient with unexplained muscle symptoms indicates myopathy. ADVICOR therapy should be discontinued if myopathy is diagnosed or suspected.
In patients with complicated medical histories predisposing to rhabdomyolysis, such as preexisting renal insufficiency, dose escalation requires caution. Also, as there are no known adverse consequences of brief interruption of therapy, treatment with ADVICOR should be stopped for a few days before elective major surgery and when any major acute medical or surgical condition supervenes.
Use of ADVICOR with other DrugsGemfibrozil, particularly with higher doses of lovastatin:The incidence and severity of myopathy may be increased by concomitant administration of ADVICOR with drugs that can cause myopathy when given alone, such as gemfibrozil and other fibrates. The dose of lovastatin should not exceed 20 mg daily in patients receiving concomitant medication with gemfibrozil.
The use of ADVICOR in combination with fibrates should be avoided unless the benefit of further alterations in lipid levels is likely to outweigh the increased risk of this drug combination.
Cyclosporine or danazol, with higher doses of lovastatin:In patients taking concomitant cyclosporine, danazol or fibrates, the dose of ADVICOR should generally not exceed 1000 mg/20 mg (see DOSAGE AND ADMINISTRATION), as the risk of myopathy may increase at higher doses. Interruption of ADVICOR therapy during a course of treatment with a systemic antifungal azole or a macrolide antibiotic, or a ketolide antibiotic should be considered.
PRECAUTIONS
GeneralBefore instituting therapy with a lipid-altering medication, an attempt should be made to control dyslipidemia with appropriate diet, exercise, and weight reduction in obese patients, and to treat other underlying medical problems (see INDICATIONS AND USAGE).
Patients with a past history of jaundice, hepatobiliary disease, or peptic ulcer should be observed closely during ADVICOR therapy. Frequent monitoring of liver function tests and blood glucose should be performed to ascertain that the drug is producing no adverse effects on these organ systems.
Diabetic patients may experience a dose-related rise in fasting blood sugar (FBS). In three clinical studies, which included 1028 patients exposed to ADVICOR (6 to 22% of whom had diabetes type II at baseline), increases in FBS above normal occurred in 46 to 65% of patients at any time during study treatment with ADVICOR. Fourteen patients (1.4%) were discontinued from study treatment: 3 patients for worsening diabetes, 10 patients for hyperglycemia and 1 patient for a new diagnosis of diabetes. In the studies in which lovastatin and NIASPAN were used as active controls, 24 to 41% of patients receiving lovastatin and 43 to 58% of patients receiving NIASPAN also had increases in FBS above normal. One patient (1.1%) receiving lovastatin was discontinued for hyperglycemia. Diabetic or potentially diabetic patients should be observed closely during treatment with ADVICOR, and adjustment of diet and/or hypoglycemic therapy may be necessary.
In one long-term study of 106 patients treated with ADVICOR, elevations in prothrombin time (PT) greater than 3 times ULN occurred in 2 patients (2%) during study drug treatment. In a long-term study of 814 patients treated with ADVICOR, 7 patients were noted to have platelet counts less than 100,000 during study drug treatment. Four of these patients were discontinued, and one patient with a platelet count less than 100,000 had prolonged bleeding after a tooth extraction. Prior studies have shown that NIASPAN can be associated with dose-related reductions in platelet count (mean of –11% with 2000 mg) and increases of PT (mean of approximately +4%). Accordingly, patients undergoing surgery should be carefully evaluated. In controlled studies, ADVICOR has been associated with small but statistically significant dose-related reductions in phosphorus levels (mean of -10% with 2000 mg/40 mg). Phosphorus levels should be monitored periodically in patients at risk for hypophosphatemia. In clinical studies with ADVICOR, hypophosphatemia was more common in males than in females. The clinical relevance of hypophosphatemia in this population is not known.
NiacinCaution should also be used when ADVICOR is used in patients with unstable angina or in the acute phase of MI, particularly when such patients are also receiving vasoactive drugs such as nitrates, calcium channel blockers, or adrenergic blocking agents.
Elevated uric acid levels have occurred with niacin therapy; therefore, in patients predisposed to gout, niacin therapy should be used with caution. Niacin is rapidly metabolized by the liver, and excreted through the kidneys. ADVICOR is contraindicated in patients with significant or unexplained hepatic dysfunction (see CONTRAINDICATIONS and WARNINGS) and should be used with caution in patients with renal dysfunction.
LovastatinLovastatin may elevate creatine phosphokinase and transaminase levels (see WARNINGS and ADVERSE REACTIONS). This should be considered in the differential diagnosis of chest pain in a patient on therapy with lovastatin.
Endocrine function – HMG-CoA reductase inhibitors interfere with cholesterol synthesis and as such might theoretically blunt adrenal and/or gonadal steroid production. Results of clinical studies with drugs in this class have been inconsistent with regard to drug effects on basal and reserve steroid levels. However, clinical studies have shown that lovastatin does not reduce basal plasma cortisol concentration or impair adrenal reserve, and does not reduce basal plasma testosterone concentration. Another HMG-CoA reductase inhibitor has been shown to reduce the plasma testosterone response to human chorionic gonadotropin (HCG). In the same study, the mean testosterone response to HCG was slightly but not significantly reduced after treatment with lovastatin 40 mg daily for 16 weeks in 21 men. The effects of HMG-CoA reductase inhibitors on male fertility have not been studied in adequate numbers of male patients. The effects, if any, on the pituitary-gonadal axis in premenopausal women are unknown. Patients treated with lovastatin who develop clinical evidence of endocrine dysfunction should be evaluated appropriately. Caution should also be exercised if an HMG-CoA reductase inhibitor or other agent used to lower cholesterol levels is administered to patients also receiving other drugs (e.g., ketoconazole, spironolactone, cimetidine) that may decrease the levels or activity of endogenous steroid hormones.
CNS toxicity – Lovastatin produced optic nerve degeneration (Wallerian degeneration of retinogeniculate fibers) in clinically normal dogs in a dose-dependent fashion starting at 60 mg/kg/day, a dose that produced mean plasma drug levels about 30 times higher than the mean drug level in humans taking the highest recommended dose (as measured by total enzyme inhibitory activity). Vestibulocochlear Wallerian-like degeneration and retinal ganglion cell chromatolysis were also seen in dogs treated for 14 weeks at 180 mg/kg/day, a dose which resulted in a mean plasma drug level (Cmax) similar to that seen with the 60 mg/kg/day dose.
CNS vascular lesions, characterized by perivascular hemorrhage and edema, mononuclear cell infiltration of perivascular spaces, perivascular fibrin deposits and necrosis of small vessels, were seen in dogs treated with lovastatin at a dose of 180 mg/kg/day, a dose which produced plasma drug levels (Cmax) which were about 30 times higher than the mean values in humans taking 80 mg/day.
Similar optic nerve and CNS vascular lesions have been observed with other drugs of this class.
Cataracts were seen in dogs treated with lovastatin for 11 and 28 weeks at 180 mg/kg/day and 1 year at 60mg/kg/day.
Information for PatientsPatients should be advised of the following:
- to report promptly unexplained muscle pain, tenderness, or weakness (see WARNINGS, Skeletal Muscle); - to take ADVICOR at bedtime, with a low-fat snack. Administration on an empty stomach is not recommended; - to carefully follow the prescribed dosing regimen (see DOSAGE AND ADMINISTRATION); - that flushing is a common side effect of niacin therapy that usually subsides after several weeks of consistent niacin use. Flushing may last for several hours after dosing, may vary in severity, and will, by taking ADVICOR at bedtime, most likely occur during sleep. If awakened by flushing, especially if taking antihypertensives, rise slowly to minimize the potential for dizziness and/or syncope; - that taking aspirin (up to approximately 30 minutes before taking ADVICOR) or another non-steroidal anti-inflammatory drug (e.g., ibuprofen) may minimize flushing; - to avoid ingestion of alcohol or hot drinks around the time of ADVICOR administration, to minimize flushing; - should not be administered with grapefruit juice; - that if ADVICOR therapy is discontinued for an extended length of time, their physician should be contacted prior to re-starting therapy; re-titration is recommended (see DOSAGE AND ADMINISTRATION); - to notify their physician if they are taking vitamins or other nutritional supplements containing niacin or related compounds such as nicotinamide (see Drug Interactions); - to notify their physician if symptoms of dizziness occur; - if diabetic, to notify their physician of changes in blood glucose; - that ADVICOR tablets should not be broken, crushed, or chewed, but should be swallowed whole. Drug InteractionsNiacinAntihypertensive Therapy – Niacin may potentiate the effects of ganglionic blocking agents and vasoactive drugs resulting in postural hypotension.
Aspirin: Concomitant aspirin may decrease the metabolic clearance of niacin. The clinical relevance of this finding is unclear.
Bile Acid Sequestrants – An in vitro study was carried out investigating the niacin-binding capacity of colestipol and cholestyramine. About 98% of available niacin was bound to colestipol, with 10 to 30% binding to cholestyramine. These results suggest that 4 to 6 hours, or as great an interval as possible, should elapse between the ingestion of bile acid-binding resins and the administration of ADVICOR.
Other – Concomitant alcohol or hot drinks may increase the side effects of flushing and pruritus and should be avoided around the time of ADVICOR ingestion. Vitamins or other nutritional supplements containing large doses of niacin or related compounds such as nicotinamide may potentiate the adverse effects of ADVICOR.
LovastatinSerious skeletal muscle disorders, e.g., rhabdomyolysis, have been reported during concomitant therapy of lovastatin or other HMG-CoA reductase inhibitors with cyclosporine, danazol, itraconazole, ketoconazole, gemfibrozil, niacin, erythromycin, clarithromycin, telithromycin, nefazodone or HIV protease inhibitors. (See WARNINGS, Skeletal Muscle).
Coumarin Anticoagulants – In a small clinical study in which lovastatin was administered to warfarin-treated patients, no effect on PT was detected. However, another HMG-CoA reductase inhibitor has been found to produce a less than two seconds increase in PT in healthy volunteers receiving low doses of warfarin. Also, bleeding and/or increased PT have been reported in a few patients taking coumarin anticoagulants concomitantly with lovastatin. It is recommended that in patients taking anticoagulants, PT be determined before starting ADVICOR and frequently enough during early therapy to insure that no significant alteration of PT occurs. Once a stable PT has been documented, PT can be monitored at the intervals usually recommended for patients on coumarin anticoagulants. If the dose of ADVICOR is changed, the same procedure should be repeated.
Antipyrine – Lovastatin had no effect on the pharmacokinetics of antipyrine or its metabolites. However, since lovastatin is metabolized by the cytochrome P450 isoform 3A4 enzyme system, this does not preclude an interaction with other drugs metabolized by the same isoform.
Propranolol – In normal volunteers, there was no clinically significant pharmacokinetic or pharmacodynamic interaction with concomitant administration of single doses of lovastatin and propranolol.
Digoxin – In patients with hypercholesterolemia, concomitant administration of lovastatin and digoxin resulted in no effect on digoxin plasma concentrations.
Oral Hypoglycemic Agents – In pharmacokinetic studies of lovastatin in hypercholesterolemic, non-insulin dependent diabetic patients, there was no drug interaction with glipizide or with chlorpropamide.
Drug/Laboratory Test InteractionsNiacin may produce false elevations in some fluorometric determinations of plasma or urinary catecholamines. Niacin may also give false-positive reactions with cupric sulfate solution (Benedict's reagent) in urine glucose tests.
Carcinogenesis, Mutagenesis, Impairment of FertilityNo studies have been conducted with ADVICOR regarding carcinogenesis, mutagenesis, or impairment of fertility.
NiacinNiacin, administered to mice for a lifetime as a 1% solution in drinking water, was not carcinogenic. The mice in this study received approximately 6 to 8 times a human dose of 3000 mg/day as determined on a mg/m2 basis. Niacin was negative for mutagenicity in the Ames test. No studies on impairment of fertility have been performed.
LovastatinIn a 21-month carcinogenic study in mice, there was a statistically significant increase in the incidence of hepatocellular carcinomas and adenomas in both males and females at 500 mg/kg/day. This dose produced a total plasma drug exposure 3 to 4 times that of humans given the highest recommended dose of lovastatin (drug exposure was measured as total HMG-CoA reductase inhibitory activity in extracted plasma). Tumor increases were not seen at 20 and 100 mg/kg/day, doses that produced drug exposures of 0.3 to 2 times that of humans at the 80 mg/day dose. A statistically significant increase in pulmonary adenomas was seen in female mice at approximately 4 times the human drug exposure. (Although mice were given 300 times the human dose on a mg/kg body weight basis, plasma levels of total inhibitory activity were only 4 times higher in mice than in humans given 80 mg of lovastatin.)
There was an increase in incidence of papilloma in the non-glandular mucosa of the stomach of mice beginning at exposures of 1 to 2 times that of humans. The glandular mucosa was not affected. The human stomach contains only glandular mucosa.
In a 24-month carcinogenicity study in rats, there was a positive dose-response relationship for hepatocellular carcinogenicity in males at drug exposures between 2 to 7 times that of human exposure at 80 mg/day (doses in rats were 5, 30, and 180 mg/kg/day).
An increased incidence of thyroid neoplasms in rats appears to be a response that has been seen with other HMG-CoA reductase inhibitors.
A drug in this class chemically similar to lovastatin was administered to mice for 72 weeks at 25, 100, and 400 mg/kg body weight, which resulted in mean serum drug levels approximately 3, 15, and 33 times higher than the mean human serum drug concentration (as total inhibitory activity) after a 40 mg oral dose. Liver carcinomas were significantly increased in high-dose females and mid- and high-dose males, with a maximum incidence of 90% in males. The incidence of adenomas of the liver was significantly increased in mid- and high-dose females. Drug treatment also significantly increased the incidence of lung adenomas in mid- and high-dose males and females. Adenomas of the Harderian gland (a gland of the eye of rodents) were significantly higher in high-dose mice than in controls.
No evidence of mutagenicity was observed in a microbial mutagen test using mutant strains of Salmonella typhimurium with or without rat or mouse liver metabolic activation. In addition, no evidence of damage to genetic material was noted in an in vitro alkaline elution assay using rat or mouse hepatocytes, a V-79 mammalian cell forward mutation study, an in vitro chromosome aberration study in CHO cells, or an in vivo chromosomal aberration assay in mouse bone marrow.
Drug-related testicular atrophy, decreased spermatogenesis, spermatocytic degeneration and giant cell formation were seen in dogs starting at 20 mg/kg/day. Similar findings were seen with another drug in this class. No drug-related effects on fertility were found in studies with lovastatin in rats. However, in studies with a similar drug in this class, there was decreased fertility in male rats treated for 34 weeks at 25 mg/kg body weight, although this effect was not observed in a subsequent fertility study when this same dose was administered for 11 weeks (the entire cycle of spermatogenesis, including epididymal maturation). In rats treated with this same reductase inhibitor at 180 mg/kg/day, seminiferous tubule degeneration (necrosis and loss of spermatogenic epithelium) was observed. No microscopic changes were observed in the testes from rats of either study. The clinical significance of these findings is unclear.
PregnancyPregnancy Category X— See CONTRAINDICATIONS.
ADVICOR should be administered to women of childbearing potential only when such patients are highly unlikely to conceive and have been informed of the potential hazard. Safety in pregnant women has not been established and there is no apparent benefit to therapy with ADVICOR during pregnancy (see CONTRAINDICATIONS). Treatment should be immediately discontinued as soon as pregnancy is recognized.
NiacinAnimal reproduction studies have not been conducted with niacin or with ADVICOR. It is also not known whether niacin at doses typically used for lipid disorders can cause fetal harm when administered to pregnant women or whether it can affect reproductive capacity. If a woman receiving niacin or ADVICOR for primary hypercholesterolemia (Types IIa or IIb) becomes pregnant, the drug should be discontinued.
LovastatinRare reports of congenital anomalies have been received following intrauterine exposure to HMG-CoA reductase inhibitors. In a review7 of approximately 100 prospectively followed pregnancies in women exposed to lovastatin or another structurally related HMG-CoA reductase inhibitor, the incidences of congenital anomalies, spontaneous abortions and fetal deaths/stillbirths did not exceed what would be expected in the general population. The number of cases is adequate only to exclude a 3- to 4-fold increase in congenital anomalies over the background incidence. In 89% of the prospectively followed pregnancies, drug treatment was initiated prior to pregnancy and was discontinued at some point in the first trimester when pregnancy was identified.
Lovastatin has been shown to produce skeletal malformations at plasma levels 40 times the human exposure (for mouse fetus) and 80 times the human exposure (for rat fetus) based on mg/m2 surface area (doses were 800 mg/kg/day). No drug-induced changes were seen in either species at multiples of 8 times (rat) or 4 times (mouse) based on surface area. No evidence of malformations was noted in rabbits at exposures up to 3 times the human exposure (dose of 15 mg/kg/day, highest tolerated dose).
Labor and DeliveryNo studies have been conducted on the effect of ADVICOR, niacin or lovastatin on the mother or the fetus during labor or delivery, on the duration of labor or delivery, or on the growth, development, and functional maturation of the child.
Nursing MothersNo studies have been conducted with ADVICOR in nursing mothers.
Because of the potential for serious adverse reactions in nursing infants from lipid-altering doses of niacin and lovastatin (see CONTRAINDICATIONS), ADVICOR should not be taken while a woman is breastfeeding.
Niacin has been reported to be excreted in human milk. It is not known whether lovastatin is excreted in human milk. A small amount of another drug in this class is excreted in human breast milk.
Pediatric UseNo studies in patients under 18 years-of-age have been conducted with ADVICOR. Because pediatric patients are not likely to benefit from cholesterol lowering for at least a decade and because experience with this drug or its active ingredients is limited, treatment of pediatric patients with ADVICOR is not recommended at this time.
Geriatric UseOf the 214 patients who received ADVICOR in double-blind clinical studies, 37.4% were 65 years-of-age and older, and of the 814 patients who received ADVICOR in open-label clinical studies, 36.2% were 65 years-of-age and older. Responses in LDL-C, HDL-C, and TG were similar in geriatric patients. No overall differences in the percentage of patients with adverse events were observed between older and younger patients. No overall differences were observed in selected chemistry values between the two groups except for amylase which was higher in older patients.
ADVERSE REACTIONS
OverviewIn controlled clinical studies, 40/214 (19%) of patients randomized to ADVICOR discontinued therapy prior to study completion. Of the 214 patients enrolled 18 (8%) discontinued due to flushing. In the same controlled studies, 9/94 (10%) of patients randomized to lovastatin and 19/92 (21%) of patients randomized to NIASPAN also discontinued treatment prior to study completion secondary to adverse events. Flushing episodes (i.e., warmth, redness, itching and/or tingling) were the most common treatment-emergent adverse events, and occurred in 53% to 83% of patients treated with ADVICOR. Spontaneous reports with NIASPAN and clinical studies with ADVICOR suggest that flushing may also be accompanied by symptoms of dizziness or syncope, tachycardia, palpitations, shortness of breath, sweating, chills, and/or edema.
Adverse Reactions InformationBecause clinical studies are conducted under widely varying conditions, adverse reaction rates observed in clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in clinical practice. The adverse reaction information from clinical studies does, however provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
The data described in this section reflect the exposure to ADVICOR in two double-blind, controlled clinical studies of 400 patients. The population was 28 to 86 years-of-age, 54% male, 85% Caucasian, 9% Black, and 7% Other, and had mixed dyslipidemia (Frederickson Types IIa and IIb).
In addition to flushing, other adverse events occurring in 5% or greater of patients treated with ADVICOR are shown in Table 8 below.
| Adverse Event | ADVICOR | NIASPAN | Lovastatin |
| Total Number of Patients | 214 | 92 | 94 |
|
|
|
|
|
| Cardiovascular
| 163 (76%) | 66 (72%) | 24 (26%) |
| Flushing | 152 (71%) | 60 (65%) | 17 (18%) |
|
|
|
|
|
| Body as a Whole
| 104 (49%) | 50 (54%) | 42 (45%) |
| Asthenia | 10 (5%) | 6 (7%) | 5 (5%) |
| Flu Syndrome | 12 (6%) | 7 (8%) | 4 (4%) |
| Headache | 20 (9%) | 12 (13%) | 5 (5%) |
| Infection | 43 (20%) | 14 (15%) | 19 (20%) |
| Pain | 18 (8%) | 3 (3%) | 9 (10%) |
| Pain, Abdominal | 9 (4%) | 1 (1%) | 6 (6%) |
| Pain, Back | 10 (5%) | 5 (5%) | 5 (5%) |
|
|
|
|
|
| Digestive System
| 51 (24%) | 26 (28%)
| 16 (17%)
|
| Diarrhea | 13 (6%) | 8 (9%) | 2 (2%) |
| Dyspepsia | 6 (3%) | 5 (5%) | 4 (4%) |
| Nausea | 14 (7%) | 11 (12%) | 2 (2%) |
| Vomiting | 7 (3%) | 5 (5%) | 0 |
|
|
|
|
|
| Metabolic and Nutrit. System
| 37 (17%) | 18 (20%)
| 13 (14%)
|
| Hyperglycemia | 8 (4%) | 6 (7%) | 6 (6%) |
|
|
|
|
|
| Musculoskeletal System
| 19 (9%) | 9 (10%)
| 17 (18%) |
| Myalgia | 6 (3%) | 5 (5%) | 8 (9%) |
|
|
|
|
|
| Skin and Appendages
| 38 (18%) | 19 (21%)
| 11 (12%)
|
| Pruritus | 14 (7%) | 7 (8%) | 3 (3%) |
| Rash | 11 (5%) | 11 (12%) | 3 (3%) |
Note: Percentages are calculated from the total number of patients in each column.
The following adverse events have also been reported with niacin, lovastatin, and/or other HMG-CoA reductase inhibitors, but not necessarily with ADVICOR, either during clinical studies or in routine patient management.
| Body as a Whole: | chest pain; abdominal pain; edema; chills; malaise |
| Cardiovascular: | atrial fibrillation; tachycardia; palpitations, and other cardiac arrhythmias; orthostasis; hypotension; syncope |
| Eye: | toxic amblyopia; cystoid macular edema; ophthalmoplegia; eye irritation |
| Gastrointestinal: | activation of peptic ulcers and peptic ulceration; dyspepsia; vomiting; anorexia; constipation; flatulence, pancreatitis; hepatitis; fatty change in liver; jaundice; and rarely, cirrhosis, fulminant hepatic necrosis, and hepatoma |
| Metabolic: | gout |
| Musculoskeletal: | muscle cramps; myopathy; rhabdomyolysis; arthralgia |
| Nervous: | dizziness; insomnia; dry mouth; paresthesia; anxiety; tremor; vertigo; memory loss; peripheral neuropathy; psychic disturbances; dysfunction of certain cranial nerves |
| Skin: | hyper-pigmentation; acanthosis nigricans; urticaria; alopecia; dry skin; sweating; and a variety of skin changes (e.g., nodules, discoloration, dryness of mucous membranes, changes to hair/nails) |
| Respiratory: | dyspnea; rhinitis |
| Urogenital: | gynecomastia; loss of libido; erectile dysfunction |
| Hypersensitivity reactions: | An apparent hypersensitivity syndrome has been reported rarely, which has included one or more of the following features: anaphylaxis, angioedema, lupus erythematous-like syndrome, polymyalgia rheumatica, vasculitis, purpura, thrombocytopenia, leukopenia, hemolytic anemia, positive ANA, ESR increase, eosinophilia, arthritis, arthralgia, urticaria, asthenia, photosensitivity, fever, chills, flushing, malaise, dyspnea, toxic epidermal necrolysis, erythema multiforme, including Stevens-Johnson syndrome. |
| Other: | migraine |
Elevations in serum transaminases (see WARNINGS - Liver Dysfunction), CPK and fasting glucose, and reductions in phosphorus. Niacin extended-release tablets have been associated with slight elevations in LDH, uric acid, total bilirubin, and amylase. Lovastatin and/or HMG-CoA reductase inhibitors have been associated with elevations in alkaline phosphatase, γ-glutamyl transpeptidase and bilirubin, and thyroid function abnormalities.
HematologyNiacin extended-release tablets have been associated with slight reductions in platelet counts and prolongation in PT (see WARNINGS).
DRUG ABUSE AND DEPENDENCE
Neither niacin nor lovastatin is a narcotic drug. ADVICOR has no known addiction potential in humans.
OVERDOSAGE
Information on acute overdose with ADVICOR in humans is limited. Until further experience is obtained, no specific treatment of overdose with ADVICOR can be recommended. The patient should be carefully observed and given supportive treatment.
NiacinThe s.c. LD50 of niacin is 5 g/kg in rats.
The signs and symptoms of an acute overdose of niacin can be anticipated to be those of excessive pharmacologic effect: severe flushing, nausea/vomiting, diarrhea, dyspepsia, dizziness, syncope, hypotension, possibly cardiac arrhythmias and clinical laboratory abnormalities. Insufficient information is available on the potential for the dialyzability of niacin.
LovastatinAfter oral administration of lovastatin to mice the median lethal dose observed was greater than 15 g/m2.
Five healthy human volunteers have received up to 200 mg of lovastatin as a single dose without clinically significant adverse experiences. A few cases of accidental overdose have been reported; no patients had any specific symptoms, and all patients recovered without sequelae. The maximum dose taken was 5 to 6 g. The dialyzability of lovastatin and its metabolites in man is not known at present.
DOSAGE AND ADMINISTRATION
The patient should be placed on a standard cholesterol-lowering diet before receiving ADVICOR or its individual active components and should continue on this diet during treatment with lipid-altering therapy (see NCEP Treatment Guidelines for details on dietary therapy).
ADVICORADVICOR should be taken at bedtime, with a low-fat snack. ADVICOR tablets should be taken whole and should not be broken, crushed, or chewed before swallowing. Patients not currently on Niaspan must start Advicor at the lowest initial ADVICOR dose, a single 500 mg/20 mg tablet once daily at bedtime. The dose of ADVICOR should not be increased by more than 500 mg daily (based on the NIASPAN component) every 4 weeks. The dose of ADVICOR should be individualized based on targeted goals for cholesterol and triglycerides, and on patient response. Doses of ADVICOR greater than 2000 mg/40 mg daily are not recommended. If ADVICOR therapy is discontinued for an extended period (greater than 7 days), reinstitution of therapy should begin with the lowest dose of ADVICOR.
Flushing of the skin (see ADVERSE REACTIONS) may be reduced in frequency or severity by pretreatment with aspirin (taken up to approximately 30 minutes prior to ADVICOR dose) or other non-steroidal anti-inflammatory drugs. Flushing, pruritus, and gastrointestinal distress are also greatly reduced by slowly increasing the dose of niacin and avoiding administration on an empty stomach.
Equivalent doses of ADVICOR may be substituted for equivalent doses of NIASPAN but should not be substituted for other modified-release (sustained-release or time-release) niacin preparations or immediate-release (crystalline) niacin preparations (see WARNINGS). Patients previously receiving niacin products other than NIASPAN should be started on NIASPAN with the recommended NIASPAN titration schedule, and the dose should subsequently be individualized based on patient response. A relative bioavailability study results indicated that ADVICOR tablet strengths (i.e. two tablets of 500 mg/20 mg and one tablet of 1000 mg/40 mg) are not interchangeable.
NIASPANNIASPAN should be taken at bedtime, after a low-fat snack, and doses should be individualized according to patient response. Therapy with NIASPAN must be initiated at 500mg qhs in order to reduce the incidence and severity of side effects which may occur during early therapy. NIASPAN must be titrated and the dose should not be increased by more than 500 mg every 4 weeks up to a maximum dose of 2000 mg a day. The recommended dose escalation is shown in Table 9 below. Patients already receiving a stable dose of NIASPAN may be switched directly to a niacin-equivalent dose of ADVICOR.
Table 9. Recommended Dosing
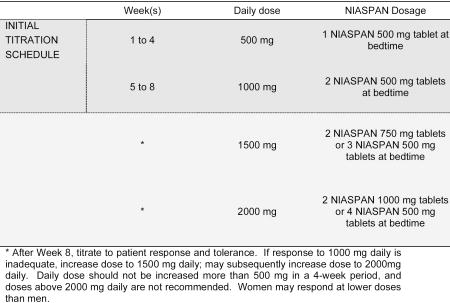
The daily dosage of NIASPAN should not be increased by more than 500 mg in any 4-week period. The recommended maintenance dose is 1000 mg (two 500 mg tablets) to 2000 mg (two 1000 mg tablets or four 500 mg tablets) once daily at bedtime. Doses greater than 2000 mg daily are not recommended. Women may respond at lower NIASPAN doses than men.
Flushing of the skin (see ADVERSE REACTIONS) may be reduced in frequency or severity by pretreatment with aspirin (taken 30 minutes prior to NIASPAN dose) or non-steroidal anti-inflammatory drugs. Tolerance to this flushing develops rapidly over the course of several weeks. Flushing, pruritus, and gastrointestinal distress are also greatly reduced by slowly increasing the dose of niacin and avoiding administration on an empty stomach.
Equivalent doses of NIASPAN should not be substituted for sustained-release (modified-release, timed-release) niacin preparations or immediate-release (crystalline) niacin (see WARNINGS). Patients previously receiving other niacin products should be started with the recommended NIASPAN titration schedule (see Table 9), and the dose should subsequently be individualized based on patient response. Single-dose bioavailability studies have demonstrated that NIASPAN tablet strengths are not interchangeable.
If NIASPAN therapy is discontinued for an extended period, reinstitution of therapy should include a titration phase (see Table 9).
NIASPAN tablets should be taken whole and should not be broken, crushed or chewed before swallowing.
Concomitant Therapy Concomitant Therapy with LovastatinPatients already receiving a stable dose of lovastatin who require further TG-lowering or HDL-raising (e.g., to achieve NCEP non-HDL-C goals), may receive concomitant dosage titration with NIASPAN per NIASPAN recommended initial titration schedule (see Table 9, DOSAGE AND ADMINISTRATION section). For patients already receiving a stable dose of NIASPAN who require further LDL-lowering (e.g., to achieve NCEP LDL-C goals; Table 7), the usual recommended starting dose of lovastatin is 20 mg once a day. Dose adjustments should be made at intervals of 4 weeks or more. Combination therapy with NIASPAN and lovastatin should not exceed doses of 2000 mg and 40 mg daily, respectively.
Dosage in Patients with Renal or Hepatic InsufficiencyUse of NIASPAN in patients with renal or hepatic insufficiency has not been studied. NIASPAN is contraindicated in patients with significant or unexplained hepatic dysfunction (see WARNINGS, PRECAUTIONS). NIASPAN should be used with caution in patients with renal insufficiency (see CLINICAL PHARMACOLOGY).
LovastatinThe usual recommended starting dose is 20 mg once a day given with the evening meal. The recommended dosing range is 10-80 mg/day in single or two divided doses; the maximum recommended dose is 80 mg/day. Doses should be individualized according to the recommended goal of therapy (see NCEP Guidelines and CLINICAL PHARMACOLOGY). Patients requiring reductions in LDL cholesterol of 20% or more to achieve their goal (see INDICATIONS AND USAGE) should be started on 20 mg/day of lovastatin. A starting dose of 10 mg may be considered for patients requiring smaller reductions. Adjustments should be made at intervals of 4 weeks or more.
Cholesterol levels should be monitored periodically and consideration should be given to reducing the dosage of lovastatin if cholesterol levels fall significantly below the targeted range.
Dosage in Patients taking Cyclosporine or DanazolIn patients taking cyclosporine or danazol concomitantly with lovastatin (see WARNINGS, Myopathy/Rhabdomyolysis), therapy should begin with 10 mg of lovastatin and should not exceed 20 mg/day.
Dosage in Patients taking Amiodarone or VerapamilIn patients taking amiodarone or verapamil concomitantly with lovastatin, the dose should not exceed 40 mg/day (see WARNINGS, Myopathy/Rhabdomyolysis and PRECAUTIONS, Drug Interactions, Other drug interactions).
Dosage in Patients with Renal InsufficiencyIn patients with severe renal insufficiency (creatinine clearance less than 30 mL/min), dosage increases above 20 mg/day should be carefully considered and, if deemed necessary, implemented cautiously (see CLINICAL PHARMACOLOGY and WARNINGS, Myopathy/Rhabdomyolysis).
HOW SUPPLIED
ADVICOR is an unscored capsule-shaped tablet containing either 500, 750, or 1000 mg of extended-release niacin, and 20 mg of immediate-release lovastatin (ADVICOR 500 mg/20 mg, 750 mg/20 mg, 1000 mg/20 mg), or 1000 mg of extended-release niacin and 40 mg of immediate-release lovastatin (ADVICOR 1000 mg/40 mg). Tablets are color-coated and debossed with “KOS” on one side and the tablet strength code on the other side. ADVICOR 500 mg/20 mg tablets are light yellow, code “502”. ADVICOR 750 mg/20 mg tablets are light orange, code “752”. ADVICOR 1000 mg/20 mg tablets are dark pink/light purple, code “1002”. ADVICOR 1000 mg/40 mg tablets are reddish brown, code “1004.” Tablets are supplied in bottles as shown below.
500 mg/20 mg tablets:
bottles of 30 - NDC # 54868-4807-1
bottles of 60 - NDC # 54868-4807-0
bottles of 90 - NDC # 54868-4807-2
750 mg/20 mg tablets:
bottles of 30 - NDC # 54868-4999-1
bottles of 60 - NDC # 54868-4999-0
1000 mg/20 mg tablets:
bottles of 30 - NDC # 54868-5087-0
1000 mg/40 mg tablets:
bottles of 30 - NDC # 54868-5653-0
Store at room temperature (20° to 25°C or 68° to 77°F).
NIASPAN is a registered trademark of Abbott Laboratories, and Mevacor is a registered trademark of Merck & Co., Inc.
REFERENCES
- Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001; 285:2486-2497.
- Nikkila EA. In: The Metabolic Basis of Inherited Disease, 5th ed., Chap 30, 622-642, 1983.
- Grundy SM, et al. Circulation 2004; 110:227-239.
- Downs JR, et al. JAMA 1998; 279:1615-1622.
- Bradford RH, et al. Arch Intern Med 1991;151:43-49.
- Bradford RH, et al. Am J Cardiol 1994; 74:667-673.
- Manson JM, et al. Reprod Toxicol 1996; 10(6): 439-446.
Mfr. for:
Abbott Laboratories
North Chicago, IL 60064,
U.S.A.
2007 Abbott Laboratories, North Chicago, IL 60064, U.S.A.
Printed in
U.S.A.
U.S. Patent Nos. 6,080,428; 6,129,930; 6,406,715 B1; 6,676,967;
6,746,691;
6,818,229; 7,011,848; and other patents pending.
PRINCIPAL DISPLAY PANEL
Advicor, Niacin extended-Release/Lovastatin Tablets
500 mg/20 mg
Advicor, Niacin extended-Release/Lovastatin Tablets
750 mg/20 mg
Advicor, Niacin extended-Release/Lovastatin Tablets
1000 mg/20 mg
Advicor, Niacin extended-Release/Lovastatin Tablets
1000 mg/40 mg
| ADVICOR
niacin and lovastatin tablet, extended release |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021249 | 06/03/2003 | |
| ADVICOR
niacin and lovastatin tablet, film coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021249 | 02/18/2004 | |
| ADVICOR
niacin and lovastatin tablet, film coated |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021249 | 06/07/2004 | |
| ADVICOR
niacin and lovastatin tablet, film coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Marketing Information | |||
| Marketing Category | Application Number or Monograph Citation | Marketing Start Date | Marketing End Date |
| NDA | NDA021249 | 08/08/2006 | |
| Labeler - Physicians Total Care, Inc. (194123980) |
| Establishment | |||
| Name | Address | ID/FEI | Operations |
| Physicians Total Care, Inc. | 194123980 | repack, relabel | |