LUPRON DEPOT-PED- leuprolide acetate
AbbVie Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use LUPRON DEPOT-PED safely and effectively. See full prescribing information for LUPRON DEPOT-PED.
LUPRON DEPOT-PED (leuprolide acetate for depot suspension) Injection, Powder, Lyophilized, For Suspension Initial U.S. Approval: 1993 RECENT MAJOR CHANGESINDICATIONS AND USAGELUPRON DEPOT-PED is a gonadotropin releasing hormone (GnRH) agonist indicated in the treatment of children with central precocious puberty. (1) DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS7.5 mg, 11.25 mg, and 15 mg intramuscular injections in a prefilled dual chamber syringe. (3) WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
To report SUSPECTED ADVERSE REACTIONS, contact AbbVie Inc. at 1-800-633-9110 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION. Revised: 06/2013 |
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
LUPRON DEPOT-PED is indicated in the treatment of children with central precocious puberty (CPP).
CPP is defined as early onset of secondary sexual characteristics (generally earlier than 8 years of age in girls and 9 years of age in boys) associated with pubertal pituitary gonadotropin activation. It may show a significantly advanced bone age that can result in diminished adult height.
Prior to initiation of treatment a clinical diagnosis of CPP should be confirmed by measurement of blood concentrations of luteinizing hormone (LH) (basal or stimulated with a GnRH analog), sex steroids, and assessment of bone age versus chronological age. Baseline evaluations should include height and weight measurements, diagnostic imaging of the brain (to rule out intracranial tumor), pelvic/testicular/adrenal ultrasound (to rule out steroid secreting tumors), human chorionic gonadotropin levels (to rule out a chorionic gonadotropin secreting tumor), and adrenal steroid measurements to exclude congenital adrenal hyperplasia.
2 DOSAGE AND ADMINISTRATION
2.1 Dose and Principles of Dosing
LUPRON DEPOT-PED must be administered under the supervision of a physician.
LUPRON DEPOT-PED is administered as a single intramuscular injection once a month. The starting dose will be dictated by the child's weight, as indicated in the table below.
| Table 1. Dosing Recommendations Based on Body Weight for LUPRON DEPOT-PED–1 Month Formulations | |
|---|---|
| Body Weight | Recommended Dose |
| ≤ 25 kg | 7.5 mg |
| > 25-37.5 kg | 11.25 mg |
| > 37.5 kg | 15 mg |
The dose of LUPRON DEPOT-PED must be individualized for each child. If adequate hormonal and clinical suppression is not achieved with the starting dose, it should be increased to the next available higher dose (e.g. 11.25 mg or 15 mg at the next monthly injection). Similarly, the dose may be adjusted with changes in body weight. The injection site should be varied periodically.
The goal of therapy is to suppress pituitary gonadotropins and peripheral sex steroids, and to arrest progression of secondary sexual characteristics. Hormonal and clinical parameters should be monitored after 1–2 months of initiating therapy and with each dose change to ensure adequate pituitary gonadotropin suppression. Once a dose that results in adequate hormonal suppression is found, it can often be maintained for the duration of therapy in most children. It is recommended, however, that adequate hormonal suppression be verified in such patients as weight can increase significantly while on therapy.
Each LUPRON DEPOT-PED strength and formulation has different release characteristics. Do not use partial syringes or a combination of syringes to achieve a particular dose.
LUPRON DEPOT-PED should be discontinued at the appropriate age of onset of puberty at the discretion of the physician.
For optimal performance of the prefilled dual chamber syringe (PDS), read and follow the instructions in Section 2.2.
2.2 Reconstitution and Administration Instructions
- The lyophilized microspheres are to be reconstituted and administered as a single intramuscular injection.
- Since LUPRON DEPOT-PED does not contain a preservative, the suspension should be injected immediately or discarded if not used within two hours.
- As with other drugs administered by injection, the injection site should be varied periodically.
- The LUPRON DEPOT-PED powder should be visually inspected and the syringe should NOT BE USED if clumping or caking is evident. A thin layer of powder on the wall of the syringe is considered normal prior to mixing with the diluent. The diluent should appear clear.
-
To prepare for injection, screw the white plunger into the end stopper until the stopper begins to turn.
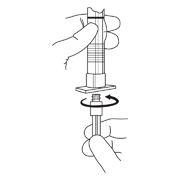
-
Hold the syringe UPRIGHT. Release the diluent by SLOWLY PUSHING (6 to 8 seconds) the plunger until the first stopper is at the blue line in the middle of the barrel.

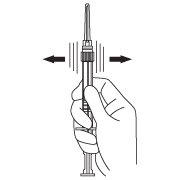
-
Keep the syringe UPRIGHT. Mix the microspheres (powder) thoroughly by gently shaking the syringe until the powder forms a uniform suspension. The suspension will appear milky. If the powder adheres to the stopper or caking/clumping is present, tap the syringe with your finger to disperse. DO NOT USE if any of the powder has not gone into suspension.
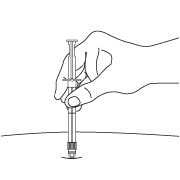
- Hold the syringe UPRIGHT. With the opposite hand pull the needle cap upward without twisting.
-
Keep the syringe UPRIGHT. Advance the plunger to expel the air from the syringe.
Now the syringe is ready for injection. -
After cleaning the injection site with an alcohol swab, the intramuscular injection should be performed by inserting the needle at a 90 degree angle into the gluteal area, anterior thigh, or shoulder; injection sites should be alternated.
NOTE: Aspirated blood would be visible just below the luer lock connection if a blood vessel is accidentally penetrated. If present, blood can be seen through the transparent LuproLoc® safety device. If blood is present remove the needle immediately. Do not inject the medication.
- Inject the entire contents of the syringe intramuscularly at the time of reconstitution. The suspension settles very quickly following reconstitution; therefore, LUPRON DEPOT-PED should be mixed and used immediately.
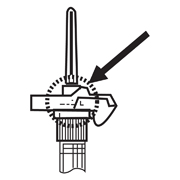
-
Withdraw the needle. Once the syringe has been withdrawn, activate immediately the LuproLoc® safety device by pushing the arrow on the lock upward towards the needle tip with the thumb or finger, as illustrated, until the needle cover of the safety device is fully extended over the needle and a CLICK is heard or felt.

3 DOSAGE FORMS AND STRENGTHS
LUPRON DEPOT-PED–1 Month (7.5 mg, 11.25 mg, and 15 mg) is supplied in a prefilled dual chamber syringe.
4 CONTRAINDICATIONS
- Hypersensitivity to GnRH, GnRH agonists or any of the excipients in LUPRON DEPOT-PED. Reports of anaphylactic reactions to GnRH agonists have been reported in the medical literature.
- All formulations of LUPRON DEPOT may cause fetal harm if administered to a pregnant woman. When LUPRON DEPOT was administered subcutaneously to rabbits it produced a dose related increase in major fetal abnormalities, and fetal mortality. The possibility exists that spontaneous abortion may occur if the drug is administered during pregnancy. LUPRON DEPOT-PED is contraindicated in women who are or may become pregnant. If this drug is inadvertently used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus.
5 WARNINGS AND PRECAUTIONS
5.1 Initial Rise of Gonadotropins and Sex Steroid Levels
During the early phase of therapy, gonadotropins and sex steroids rise above baseline because of the initial stimulatory effect of the drug. Therefore, an increase in clinical signs and symptoms of puberty may be observed [see Clinical Pharmacology (12.3)].
5.2 Convulsions
Postmarketing reports of convulsions have been observed in patients on leuprolide acetate therapy. These included patients with a history of seizures, epilepsy, cerebrovascular disorders, central nervous system anomalies or tumors, and patients on concomitant medications that have been associated with convulsions such as bupropion and SSRIs. Convulsions have also been reported in patients in the absence of any of the conditions mentioned above.
5.3 Monitoring and Laboratory Tests
Response to LUPRON DEPOT-PED should be monitored with a GnRHa stimulation test, basal LH or serum concentration of sex steroid levels beginning 1-2 months following initiation of therapy, with changing doses, or potentially during therapy in order to confirm maintenance of efficacy. Measurement of bone age for advancement should be done every 6-12 months.
Once a therapeutic dose has been established, gonadotropin and sex steroid levels will decline to prepubertal levels. Noncompliance with drug regimen or inadequate dosing may result in inadequate control of the pubertal process with gonadotropins and/or sex steroids increasing above prepubertal levels [see Clinical Studies (14) and Adverse Reactions (6)].
6 ADVERSE REACTIONS
The most common adverse reactions with GnRH agonists including LUPRON DEPOT-PED are injection site reactions/pain including abscess, general pain, headache, emotional lability and hot flushes/sweating.
During the early phase of therapy, gonadotropins and sex steroids rise above baseline because of the natural initial stimulatory effect of the drug (hormonal flare effect). Therefore, an increase in clinical signs and symptoms may be observed [see Warnings and Precautions (5.1)].
6.1 LUPRON DEPOT-PED–1 Month (7.5 mg, 11.25 mg, and 15 mg Injection) - Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
In two studies of children with central precocious puberty, in 2% or more of the patients receiving the drug, the following adverse reactions were reported to have a possible or probable relationship to drug as ascribed by the treating physician. Reactions which are not considered drug-related are excluded.
| Table 2. Percentage of Patients with Treatment-Emergent Adverse Reactions Occurring in ≥2% of Pediatric Patients Receiving LUPRON DEPOT-PED–1 Month | ||
|---|---|---|
| * Most events were mild or moderate in severity. | ||
| Number of Patients (N = 421) |
||
| N | (%) | |
| Body as a Whole | ||
| Injection Site Reactions Including Abscess* | 37 | (9) |
| General Pain | 12 | (3) |
| Headache | 11 | (3) |
| Cardiovascular System | ||
| Vasodilation | 9 | (2) |
| Integumentary System (Skin and Appendages) | ||
| Acne/Seborrhea | 13 | (3) |
| Rash Including Erythema Multiforme | 12 | (3) |
| Nervous System | ||
| Emotional Lability | 19 | (5) |
| Urogenital System | ||
| Vaginitis/Vaginal Bleeding/Vaginal Discharge | 13 | (3) |
The following treatment-emergent adverse reactions were reported in less than 2% of the patients and are listed below by body system.
Body as a Whole – aggravation of preexisting tumor and decreased vision, allergic reaction, body odor, fever, flu syndrome, hypertrophy, infection; Cardiovascular System – bradycardia, hypertension, peripheral vascular disorder, syncope; Digestive System – constipation, dyspepsia, dysphagia, gingivitis, increased appetite, nausea/vomiting; Endocrine System – accelerated sexual maturity, feminization, goiter; Hemic and Lymphatic System – purpura; Metabolic and Nutritional Disorders – growth retarded, peripheral edema, weight gain; Musculoskeletal System – arthralgia, joint disorder, myalgia, myopathy; Nervous System – depression, hyperkinesia, nervousness, somnolence; Respiratory System – asthma, epistaxis, pharyngitis, rhinitis, sinusitis; Integumentary System (Skin and Appendages) – alopecia, hair disorder, hirsutism, leukoderma, nail disorder, skin hypertrophy; Urogenital System – cervix disorder/neoplasm, dysmenorrhea, gynecomastia/breast disorders, menstrual disorder, urinary incontinence.
Laboratory: The following laboratory events were reported as adverse reactions: antinuclear antibody present and increased sedimentation rate.
6.2 Postmarketing
The following adverse events have been observed with this or other formulations of leuprolide acetate injection. As leuprolide has multiple indications, and therefore patient populations, some of these adverse events may not be applicable to every patient.
Allergic reactions (anaphylactic, rash, urticaria, and photosensitivity reactions) have also been reported.
Gastrointestinal Disorders: nausea, abdominal pain, vomiting;
General Disorders and Administration Site Conditions: chest pain, injection site reactions including induration and abscess have been reported;
Investigations: decreased WBC, weight increased;
Metabolism and Nutrition Disorders: diabetes mellitus;
Musculoskeletal and Connective Tissue Disorders: tenosynovitis-like symptoms;
Nervous System Disorders: neuropathy peripheral, convulsion, spinal fracture/paralysis;
Skin and Subcutaneous Tissue Disorders: hot flush, flushing, hyperhidrosis;
Reproductive System and Breast Disorders: prostate pain;
Vascular Disorders: hypertension, hypotension.
Pituitary apoplexy: During post-marketing surveillance, rare cases of pituitary apoplexy (a clinical syndrome secondary to infarction of the pituitary gland) have been reported after the administration of gonadotropin-releasing hormone agonists. In a majority of these cases, a pituitary adenoma was diagnosed, with a majority of pituitary apoplexy cases occurring within 2 weeks of the first dose, and some within the first hour. In these cases, pituitary apoplexy has presented as sudden headache, vomiting, visual changes, ophthalmoplegia, altered mental status, and sometimes cardiovascular collapse. Immediate medical attention has been required.
See other LUPRON DEPOT and LUPRON Injection package inserts for other events reported in different patient populations.
7 DRUG INTERACTIONS
No pharmacokinetic-based drug-drug interaction studies have been conducted; however, drug interactions are not expected to occur [see Clinical Pharmacology (12.3)].
7.1 Drug/Laboratory Test Interactions
Administration of LUPRON DEPOT-PED in therapeutic doses results in suppression of the pituitary-gonadal system. Therefore, diagnostic tests of pituitary gonadotropic and gonadal functions conducted during treatment and up to six months after discontinuation of LUPRON DEPOT-PED may be affected. Normal pituitary-gonadal function is usually restored within six months after treatment with LUPRON DEPOT-PED is discontinued.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
LUPRON DEPOT-PED is contraindicated in women who are or may become pregnant while receiving the drug [see Contraindications (4)].
Safe use of leuprolide acetate in pregnancy has not been established in clinical studies. Before starting and during treatment with leuprolide acetate, it is advisable to establish whether the patient is pregnant. Leuprolide acetate is not a contraceptive. If contraception is required, a non-hormonal method of contraception should be used.
When LUPRON DEPOT was administered subcutaneously to groups of rabbits as one time dosing on day 6 of pregnancy at test dosages of 0.00024, 0.0024, and 0.024 mg/kg (1/1200 to 1/12 of the human pediatric dose) it produced a dose-related increase in major fetal abnormalities. Similar studies in rats failed to demonstrate an increase in fetal malformations. There was increased fetal mortality and decreased fetal weights with the two higher doses of LUPRON DEPOT in rabbits and with the highest dose in rats. No fetal malformations but increase in fetal resorptions and mortality were observed in rat and rabbit when the daily injection formulation of leuprolide acetate was dosed subcutaneously once daily at lower doses (0.1-1 mcg/kg/day in rabbit; 10 mcg/kg/day in rat) during the period of organogenesis. The effects on fetal mortality are logical consequences of the alterations in hormonal levels brought about by this drug. Therefore, the possibility exists that spontaneous abortion may occur if the drug is administered during pregnancy.
8.3 Nursing Mothers
It is not known whether leuprolide acetate is excreted in human milk. LUPRON DEPOT-PED should not be used by nursing mothers.
10 OVERDOSAGE
In early clinical trials using leuprolide acetate in adult patients, doses as high as 20 mg/day for up to two years caused no adverse effects differing from those observed with the 1 mg/day dose.
In rats, subcutaneous administration of leuprolide acetate as a single dose 333 times the recommended human pediatric dose, expressed on a per body weight basis, resulted in dyspnea, decreased activity, and local irritation at the injection site. There is no evidence at present that there is a clinical counterpart of this phenomenon.
In cases of overdosage, standard of care monitoring and management principles should be followed.
11 DESCRIPTION
Leuprolide acetate is a synthetic nonapeptide analog of naturally occurring gonadotropin-releasing hormone (GnRH or LH-RH). The analog possesses greater potency than the natural hormone. The chemical name is 5-oxo-L-prolyl-L-histidyl-L-tryptophyl-L-seryl-L-tyrosyl-D-leucyl-L-leucyl-L-arginyl-N-ethyl-L-prolinamide acetate (salt) with the following structural formula:
LUPRON DEPOT-PED is available in a prefilled dual-chamber syringe containing sterile lyophilized microspheres which, when mixed with diluent, become a suspension intended as a single intramuscular injection.
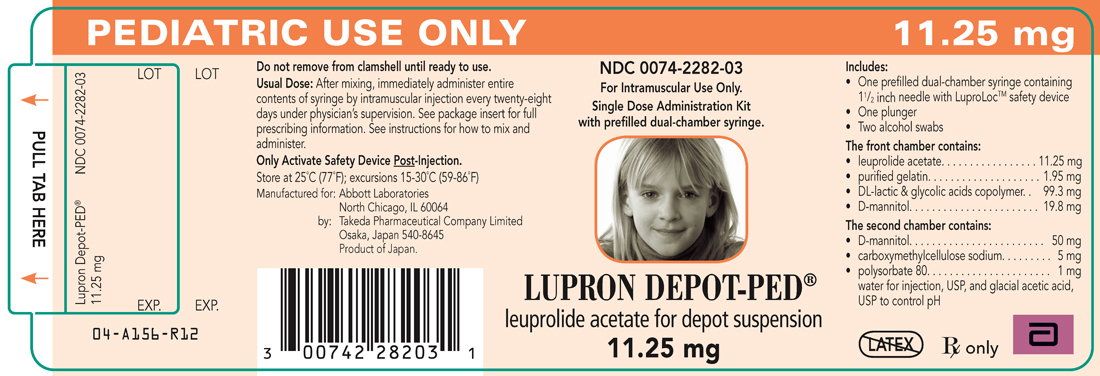
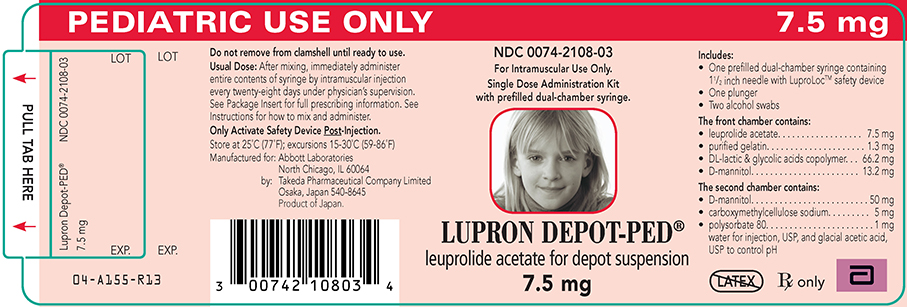
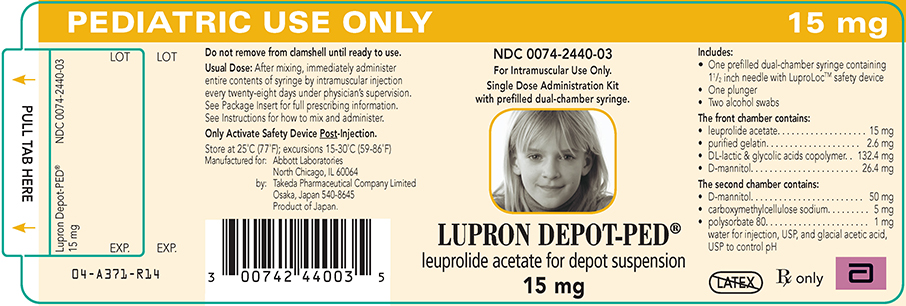
The front chamber of LUPRON DEPOT-PED 7.5 mg, 11.25 mg, and 15 mg prefilled dual-chamber syringe contains leuprolide acetate (7.5/11.25/15 mg), purified gelatin (1.3/1.95/2.6 mg), DL-lactic and glycolic acids copolymer (66.2/99.3/132.4 mg), and D-mannitol (13.2/19.8/26.4 mg). The second chamber of diluent contains carboxymethylcellulose sodium (5 mg), D-mannitol (50 mg), polysorbate 80 (1 mg), water for injection, USP, and glacial acetic acid, USP to control pH.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Leuprolide acetate, a GnRH agonist, acts as a potent inhibitor of gonadotropin secretion when given continuously and in therapeutic doses. Human studies indicate that following an initial stimulation of gonadotropins, chronic stimulation with leuprolide acetate results in suppression or "downregulation" of these hormones and consequent suppression of ovarian and testicular steroidogenesis. These effects are reversible on discontinuation of drug therapy.
12.3 Pharmacokinetics
Absorption
Following a single LUPRON DEPOT-PED–1 Month 7.5 mg injection to adult patients, mean peak leuprolide plasma concentration was almost 20 ng/mL at 4 hours and then declined to 0.36 ng/mL at 4 weeks. However, intact leuprolide and an inactive major metabolite could not be distinguished by the assay which was employed in the study. Nondetectable leuprolide plasma concentrations have been observed during chronic LUPRON DEPOT-PED 7.5 mg administration, but testosterone levels appear to be maintained at castrate levels.
In a study of 55 children with central precocious puberty, doses of 7.5 mg, 11.25 mg and 15.0 mg of LUPRON DEPOT-PED were given every 4 weeks and in a subset of 22 children, trough leuprolide plasma levels were determined according to weight categories as summarized below:
| * Group average values determined at Week 4 immediately prior to leuprolide injection. Drug levels at 12 and 24 weeks were similar to respective 4 week levels. | |||
| Patient Weight Range (kg) | Group Weight Average (kg) | Dose (mg) | Trough Plasma Leuprolide Level Mean ±SD (ng/mL)* |
| 20.2 - 27.0 | 22.7 | 7.5 | 0.77±0.033 |
| 28.4 - 36.8 | 32.5 | 11.25 | 1.25±1.06 |
| 39.3 - 57.5 | 44.2 | 15.0 | 1.59±0.65 |
Distribution
The mean steady-state volume of distribution of leuprolide following intravenous bolus administration to healthy male volunteers was 27 L. In vitro binding to human plasma proteins ranged from 43% to 49%.
Metabolism
In healthy male volunteers, a 1 mg bolus of leuprolide administered intravenously revealed that the mean systemic clearance was 7.6 L/h, with a terminal elimination half-life of approximately 3 hours based on a two compartment model.
In rats and dogs, administration of 14C-labeled leuprolide was shown to be metabolized to smaller inactive peptides, a pentapeptide (Metabolite I), tripeptides (Metabolites II and III) and a dipeptide (Metabolite IV). These fragments may be further catabolized.
The major metabolite (M-I) plasma concentrations measured in 5 prostate cancer patients reached maximum concentration 2 to 6 hours after dosing and were approximately 6% of the peak parent drug concentration. One week after dosing, mean plasma M-I concentrations were approximately 20% of mean leuprolide concentrations.
Excretion
Following administration of LUPRON DEPOT 3.75 mg to 3 patients, less than 5% of the dose was recovered as parent and M-I metabolite in the urine.
Specific Populations
The pharmacokinetics of the drug has not been determined in patients with hepatic and renal impairment.
Drug-Drug Interactions
No pharmacokinetic-based drug-drug interaction studies have been conducted with LUPRON DEPOT-PED–1 Month. However, because leuprolide acetate is a peptide that is primarily degraded by peptidase and not by cytochrome P-450 enzymes as noted in specific studies, and the drug is only about 46% bound to plasma proteins, drug interactions are not expected to occur.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
A two-year carcinogenicity study was conducted in rats and mice. In rats, a dose-related increase of benign pituitary hyperplasia and benign pituitary adenomas was noted at 24 months when the drug was administered subcutaneously at high daily doses (0.6 to 4 mg/kg). There was a significant but not dose-related increase of pancreatic islet-cell adenomas in females and of testicular interstitial cell adenomas in males (highest incidence in the low dose group). In mice, no leuprolide acetate-induced tumors or pituitary abnormalities were observed at a dose as high as 60 mg/kg for two years. Adult patients have been treated with leuprolide acetate for up to three years with doses as high as 10 mg/day and for two years with doses as high as 20 mg/day without demonstrable pituitary abnormalities.
Following subcutaneous administration of LUPRON DEPOT to male and female rats before mating there was atrophy of the reproductive organs and suppression of reproductive performance.
Following a study with leuprolide acetate, immature male rats demonstrated tubular degeneration in the testes even after a recovery period. In spite of the failure to recover histologically, the treated males proved to be as fertile as the controls. Also, no histologic changes were observed in the female rats following the same protocol. In both sexes, the offspring of the treated animals appeared normal. The effect of the treatment of the parents on the reproductive performance of the F1 generation has been evaluated using LUPRON DEPOT formulation to groups of rats as one-time subcutaneous dose of 0.024 mg/kg (1/12 of the pediatric dose) on Day 15 of gestation or dosing on parturition day at doses up to 8 mg/kg (27 fold of the pediatric dose). There was no effect on growth, morphological development and reproductive performance of F1 generation.
14 CLINICAL STUDIES
14.1 LUPRON DEPOT-PED–1 Month
In children with central precocious puberty (CPP), therapeutic doses of LUPRON DEPOT-PED reduce stimulated and basal gonadotropins to prepubertal levels. Testosterone and estradiol are also reduced to prepubertal levels in males and females respectively. Reduction of gonadotropins and sex steroids allow a return to age-appropriate physical and psychological growth and development. The following effects have been noted with the chronic administration of leuprolide: cessation of menses (in girls), normalization and stabilization of linear growth and bone age advancement, stabilization of clinical signs and symptoms of puberty.
55 CPP subjects (49 females and 6 males, naïve to previous GnRHa treatment), were treated with LUPRON DEPOT-PED–1 month formulations until age appropriate for entry into puberty (see treatment period data below) and a subset of 40 subjects were then followed post-treatment (see follow-up period data below).
During the treatment period, LUPRON DEPOT-PED suppressed gonadotropins and sex steroids to prepubertal levels. Suppression of peak stimulated LH concentrations to < 1.75 mIU/mL was achieved in 96% of subjects by month 1. The number and percentage of subjects with suppression of peak stimulated LH < 1.75 mIU/mL and mean ± SD peak stimulated LH over time is shown in Table 3. The mean ± SD age at the start of treatment was 7 ± 2 years and the duration of treatment was 4 ± 2 years. Six months after the treatment period was finished, the mean peak stimulated LH was 20.6 ± SD 13.7 mIU/mL (n=30).
| Table 3: The number and percentage of patients with peak stimulated LH < 1.75 mIU/mL and Mean (SD) peak LH at each clinic visit | |||
|---|---|---|---|
| Weeks on Study | n with peak stimulated LH < 1.75 mIU/mL/ N with a LH measurement for that week | Mean (SD) peak LH | |
| n/N | % | ||
| Baseline | 0/55 | 0% | 35.0 (21.32) |
| Week 4 | 53/55 | 96.4% | 0.8 (0.57) |
| Week 12 | 48/54 | 88.9% | 1.1 (1.77) |
| Week 24 | 48/53 | 90.6% | 0.8 (0.79) |
| Week 36 | 51/54 | 94.4% | 0.6 (0.43) |
| Week 48 | 51/54 | 94.4% | 0.6 (0.47) |
| Week 72 | 52/52 | 100% | 0.5 (0.30) |
| Week 96 | 46/46 | 100% | 0.4 (0.33) |
| Week 120 | 40/40 | 100% | 0.4 (0.27) |
| Week 144 | 36/36 | 100% | 0.4 (0.24) |
| Week 168 | 27/28 | 96.4% | 1.2 (4.58) |
| Week 216 | 18/19 | 94.7% | 0.5 (0.90) |
| Week 240 | 16/17 | 94.1% | 0.4 (0.62) |
| Week 264 | 14/15 | 95.3% | 0.4 (0.41) |
| Week 288 | 11/11 | 100% | 0.3 (0.22) |
| Week 312 | 9/9 | 100% | 0.4 (0.20) |
| Week 336 | 6/6 | 100% | 0.3 (0.10) |
| Week 360 | 6/6 | 100% | 0.3 (0.13) |
| Week 384 | 5/5 | 100% | 0.2 (0.10) |
| Week 408 | 3/3 | 100% | 0.2 (0.09) |
| Week 432 | 2/2 | 100% | 0.3 (0.04) |
| Week 456 | 2/2 | 100% | 0.2 (0.04) |
| Week 480 | 1/1 | 100% | 0.2 (NA) |
| Week 504 | 1/1 | 100% | 0.2 (NA) |
Suppression (defined as regression or no change) of the clinical/physical signs of puberty was achieved in most patients. In females, suppression of breast development ranged from 66.7 to 90.6% of subjects during the first 5 years of treatment. The mean stimulated estradiol was 15.1 pg/mL at baseline, decreased to the lower level of detection (5.0 pg/mL) by Week 4 and was maintained there during the first 5 years of treatment. In males, suppression of genitalia development ranged from 60% to 100% of subjects during the first 5 years of treatment. The mean stimulated testosterone was 347.7 ng/dL at baseline and was maintained at levels no greater than 25.3 ng/dL during the first 5 years of treatment.
A “flare effect” of transient bleeding or spotting during the first 4 weeks of treatment was observed in 19.4% (7/36) females who had not reached menarche at baseline. After the first 4 weeks and for the remainder of the treatment period, no subject reported menstrual-like bleeding, and only rare spotting was noted.
In many subjects, growth rate decreased on treatment, as did bone age: chronological age ratio. Through year 5, the mean growth rate ranged between 3.4 and 5.6 cm/yr. The mean ratio of bone age to chronological age decreased from 1.5 at baseline to 1.1 by end of treatment. The mean height standard deviation score changed from 1.6 at baseline to 0.7 at the end of the treatment phase.
35 females and 5 males participated in a post-treatment follow-up period to assess reproductive function (in females) and final height. At 6 months post-treatment, most subjects reverted to pubertal levels of LH (87.9%) and clinical signs of resumption of pubertal progression were evident with increase in breast development in girls (66.7%) and increase in genitalia development in boys (80%).
Of the 40 patients evaluated in the follow-up, 33 were observed until they reached final or near-final adult height. These patients had a mean increase in final adult height compared to baseline predicted adult height. The mean final adult height standard deviation score was -0.2.
After stopping treatment, regular menses were reported for all female subjects who reached 12 years of age during follow-up; mean time to menses was approximately 1.5 years; mean age of onset of menstruation after stopping treatment was 12.9 years. Data to assess reproductive function was collected in a post-study survey of 20 girls who reached adulthood (ages 18-26): menstrual cycles were reported to be normal in 80% of women; 12 pregnancies were reported for a total of 7 of the 20 subjects, including multiple pregnancies for 4 subjects.
16 HOW SUPPLIED/STORAGE AND HANDLING
| Kit with prefilled dual-chamber syringe | 7.5 mg | NDC 0074-2108-03 |
| Kit with prefilled dual-chamber syringe | 11.25 mg | NDC 0074-2282-03 |
| Kit with prefilled dual-chamber syringe | 15 mg | NDC 0074-2440-03 |
Each syringe contains sterile lyophilized microspheres of leuprolide acetate incorporated in a biodegradable lactic acid/glycolic acid copolymer. When mixed with 1 milliliter of accompanying diluent, LUPRON DEPOT-PED is administered as a single intramuscular injection.
- one prefilled dual-chamber syringe containing 1½ inch needle with LuproLoc® safety device
- one plunger
- two alcohol swabs
- a complete prescribing information enclosure
Store at 25°C (77°F); excursions permitted to 15–30°C (59–86°F) [See USP Controlled Room Temperature]
17 PATIENT COUNSELING INFORMATION
Prior to starting therapy with LUPRON DEPOT-PED, patients should be informed that:
- All formulations are contraindicated in women who are or may become pregnant. If this drug is used during pregnancy, or if the patient becomes pregnant while taking the drug, the patient should be informed of the potential risk to the fetus.
- Continuous therapy is important and that adherence to a monthly drug administration schedule must be accepted if therapy is to be successful. If the monthly injection schedule is not followed, pubertal development may begin again.
- During the first weeks of treatment, signs of puberty, e.g., vaginal bleeding, may occur. This is a common initial effect of the drug. If these symptoms continue beyond the second month of treatment, the physician should be notified.
- The most common side effects related to treatment with 1-month or 3-month LUPRON DEPOT-PED in clinical studies are: pain, acne/seborrhea, injection site reactions including pain, swelling and abscess, rash including erythema multiforme, vaginitis/bleeding/discharge, increased weight, headache, and altered mood.
- After injection, some pain and irritation is expected; however if more severe symptoms occur, the physician should be contacted. Any unusual signs or symptoms should be reported to the physician.
Manufactured for
AbbVie Inc.
North Chicago, IL 60064
by Takeda Pharmaceutical Company Limited
Osaka, Japan 540-8645
For Intramuscular Use Only. Single Dose Administration Kit with prefilled dual-chamber syringe.
LUPRON DEPOT-PED® leuprolide acetate for depot suspension 11.25 mg
For Intramuscular Use Only. Single Dose Administration Kit with prefilled dual-chamber syringe.
LUPRON DEPOT-PED® leuprolide acetate for depot suspension 7.5 mg
For Intramuscular Use Only. Single Dose Administration Kit with prefilled dual-chamber syringe.
LUPRON DEPOT-PED® leuprolide acetate for depot suspension 15 mg
| LUPRON DEPOT-PED
leuprolide acetate kit |
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
| LUPRON DEPOT-PED
leuprolide acetate kit |
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
| LUPRON DEPOT-PED
leuprolide acetate kit |
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
|
||||||||||||||
| Labeler - AbbVie Inc. (078458370) |